Relapsed Malignant Germ Cell Tumor Metastasized in Bone Marrow: A Rare Finding
- 1. Department of Pediatric Hematology and Oncology, The Indus Hospital and Health Network, Pakistan
- 2. Department of Hematology, The Indus Hospital and Health Network, Pakistan
Abstract
The mediastinal germ cell tumors (GCT) are malignant cancer type and exhibits poor prognosis particularly due to the extensive tissue invasion, thus complete resection via surgery is challenging. The primary sites of invasion mainly include liver, lungs and bones whereas, the bone marrow is considered as a rare site of metastasis. Here we report a case of 14-year child with relapsed mediastinal GCT and bone marrow metastasis. Initially, the patient was presented with fever and respiratory symptoms. As per computer tomography (CT) scan, morphological analysis, immunohistochemistry, and elevated levels of AFP (4948 ng/dl), the patient was diagnosed with GCT. The initial chemotherapy (6 cycles of JEB; Carboplatin, Etoposide, Bleomycin) resulted in decreased AFP levels (6.0 ng/dl) and reduction in the mediastinal mass. It was followed by complete tumor excision. On follow-up AFP levels were found rising and staging work-up showed the recurrence of the disease with distant metastasis. The patient underwent first cycle of second line chemotherapy (TIP; Paclitaxil, Ifosfamide, Cisplatin). However, due to persistent thrombocytopenia and gradual increase in AFP levels, there was suspicion of bone marrow involvement. Further bilateral bone marrow examination was found consistent with metastatic disease. Hence, treatment was continued with three more cycles of TIP. Due to extensive dissemination surgical excision was not possible hence patient was kept on supportive and palliative care. Unfortunately, the efforts remained unfruitful and due to progressive disease the patient died two months after the termination of therapy.
Keywords
Bone marrow; Chemotherapy; Mediastinal germ cell tumor; Yolk sac tumor; Immunohistochemistry
Citation
Ambreen F, Shaikh S, Meraj F, Mushtaq M, Ashraf S (2021) Relapsed Malignant Germ Cell Tumor Metastasized in Bone Marrow: a Rare Find ing. JSM Clin Case Rep 9(2): 1190.
ABBREVIATIONS
GCT: Germ Cell tumor; YST: Yolk Sac Tumor; MGCT: Mediastinal Germ Cell Tumor: CT: Computed Tomography Scan; AFP: Alpha-fetoprotein
INTRODUCTION
Yolk sac tumors (YST), also called endodermal sinus tumors are infrequent cancer types that is typically initiated in the germ cells and can affect both males and females [1]. Such tumors are most commonly found in the pediatrics population and rarely in patients >40 years of age. Of all the childhood cancers, ~ 3.5 % of cases are relevant to the germ cell tumors (GCTs) in the pediatric population under the age of 15 years. However, the frequency increases up to 16% for the ages between 15 and 19 [2]. YSTs, exhibit a microcystic reticular pattern and are cytokeratinpositive. Increased expression of α fetoprotein (AFP) has been seen in most of the cases signifying the efficiency of AFP as a diagnostic marker and monitoring of therapy [3,4].
The GCTs in regions other than gonads are rare and frequently arise in the body’s middle axis for instance the mediastinum, retroperitoneum, brain, and sacrococcygeal [5,6]. Mediastinal germ cell tumors in particular are a diverse group of neoplasms of benign and malignant nature and are predominantly traced in the anterior mediastinum. These tumors are very rare in children and are originated in the mediastinum from the abnormally migrated primitive germ cells during embryogenesis and are predominantly traced in the anterior mediastinum and are accounts for ~10% to 20% of all childhood mediastinal tumors [7,8].
These tumors frequently form giant masses consequently invading the adjacent tissues and the vital organs. Hence, the treatment is challenging and requires stringent plans and advanced surgical interventions [9]. Though the gonadal and mediastinal GCTs share common histologic features, themediastinal GCT generally exhibits a poorer prognosis in comparison to the gonadal site [10,11]. Whereas, the prognostic factors include age at the time of onset, stage of the disease, metastasis, and disease remission after chemotherapy [12,13]. However, the involvement of bone marrow is rarely seen in patients suffering from MGCTs. Below is the case report of a 14- year boy with relapse mediastinal GCT and presented the bone marrow metastasis.
CASE PRESENTATION
Clinical History
The 14-year-old male patient first time presented with complains of intermittent fever for 2 months, cough, neck swelling, and difficulty in breathing for 15 days. CT scan of the chest indicated mass in the antero-superior mediastinum (13.1*11.6*8.1cm) compressing the nearby organs. CT guided mediastinal mass biopsy revealed two linear cores exhibiting predominantly necrosis with acute and chronic inflammatory infiltrate. Focally viable cells were identified. It was followed by the immunohistochemistry analysis, where CKLMW (8/18), CKAE1/AE3, and SALL-4 were found positive, indicating the possibility of germ cell tumor.
Repeated CT chest with contrast was performed which showed large multi-lobulated centrally necrotic peripherally enhancing mass identified in anterosuperior mediastinum extending from C6/C7 down till D7/D8 vertebral level measuring 13.1x11-6 x 8.1cm, no definite infiltration in the chest wall and surrounding structures was found, serum tumor markers alphafetoprotein (AFP) was raised (4948ng/dl) and BHCG was within normal range.
After diagnosis of mediastinal GCT stage III high risk on radiological findings, staging work up was done including bone scan which showed no distant bone metastasis. It was followed by the administration of the neoadjuvant chemotherapy according to the United Kingdom Children’s Cancer Study Group (UKCCSG) 2004 Protocol. Chemotherapy included 6 cycles of JEB (Carboplatin, Etoposide, Bleomycin) with monitoring of AFP after every cycle. The treatment resulted in decreased AFP levels from 4948ng/dl to 6.0 ng/dl at the end of chemotherapy. Reassessment CT scan showed significant reduction w in mediastinal mass measuring 4.4x6.3cm with reduced mediastinal shift. No evidence of pleural effusion or pneumothorax was seen and most of the vital organs appeared unremarkable. Afterward cardiothoracic surgery for excision of tumor mass was done histopathology report revealed thymic tissue exhibiting a relatively circumscribed lesion with extensive areas of necrosis, hemorrhage and infarction showing features of yolk sac tumor. Cytokeratin AE1/AE3, Alypican-3, and SALL-4 were found positive in the immuno-hitochemical stains while the results were found negative for OCT ¾, CD30, EMA. All of the five lymph nodes recovered from right mediastinum exhibited benign reactive changes. The residual tumor comprised less than 5%. Post-operatively serial AFP levels were performed and found to be raised from 25ng/dL to 393ng/dL.
Then exactly after two months’ patient relapsed and presented to the hospital in severely sick condition with respiratory distress. Chest X-ray revealed the recurrence of soft tissue mass in mediastinum with pleural effusion and AFP value of 5259ng/dl. Patient got admitted in ICU for stabilization. Restaging CT chest and abdomen with contrast showed soft tissue density lesion of 2.6 x 2.6 cm in the anterior mediastinum with locally extensive infiltration and distant metastasis to lungs, liver and bones. Based on radiological reoccurrence of the disease and raised AFP levels, the patient was given second line chemotherapy (Ifosfamide, Cisplatin and Paclitaxil) which resulted in reduction in AFP levels from 5259 ng/dl to 1175 ng/ dl. During first course of the treatment the patient suffered from persistent thrombocytopenia. The patient was not responding to the treatment thus further tests were performed to get more detailed insight of disease condition. Pleural fluid cytology and bilateral bone marrow aspirate and trephine were examined whereas, the details are discussed below Pleural fluid for cytology was found negative for malignancy.
Bone Marrow Aspirate and Trephine Biopsy
Bilateral bone marrow aspirate and trephine were performed. The left side biopsy was reported as hypocellular with no malignant cell infiltration. However, right side bone marrow aspirate showed few scattered atypical mononuclear cells were seen characterized by medium sized, bizarre shaped nuclei, nuclear pleomorphism and moderate to abundant amount of basophilic cytoplasm. Cellular right sided biopsy exhibited effaced architecture and diffuse infiltration by atypical mononuclear cells in a heavily fibrotic background. Furthermore, immunohistochemistry was performed and CKAE1/AE3 was found positive in right sided trephine while negative in left sided trephine. Reticulin stain revealed diffuse and dense increase in reticulin with extensive intersections, Grade MF-2 was observed in right sided section while scattered linear reticulin with no intersections (Grade MF-0) was observed in the left sided section. Hence it was concluded that the tumor has metastasized to the right side of the bone marrow which is considered a rare site of metastasis for germ cell tumors.
Patient received total 4 courses of same chemotherapy. During, the end of chemotherapy the AFP levels were again rising, platelet count not recovered and still extensive disease on imaging. Surgical excision could not be possible. Thus patient was kept on palliative and supportive care. During the illness the patient was transfused with packed RBC and platelets Unfortunately, the efforts remained unfruitful and due to progressive disease the patient expired within two months after the termination of second line therapy
DISCUSSION
The involvement of bone marrow in patients with germ cell tumors is a rare event and is an indication of disease dissemination. The bone marrow metastasis was first reported in 1834, however, its physiopathology is not completely understood yet [14]. In past, a total of 3,620 bone marrow aspirates from patients with solid tumors were tested for bone marrow infiltration. The infiltration was observed in 9.1% of the tested cases and specifically associated with the patients suffering from breast cancer, prostate cancer, small lung cancer, and Ewing’s sarcoma [15]. The patient is presented with usually nonspecific clinical manifestations, however, may frequently exhibit generalized bone pain or pain may be limited to the back. Here we report the case study of metastasis relapse in the bone marrow of a primary mediastinal germ cell tumor. Previously Klaassen and coworkers (1992), reported bone marrow metastasis in three patients suffering from mediastinal germ cell tumor, and two of the patients suffered from extreme thrombocytopenia which is in agreement with the presented case report [16]. Although under routine circumstances the involvement of bone marrow is not always the first choice to be ruled out. However, in our case, the relapse of the disease with a severe condition in combination with treatment failure prompted us to examine the bone marrow. Upon analysis, the infiltration was observed in the sample collected from the right side section (Figure 1-3).
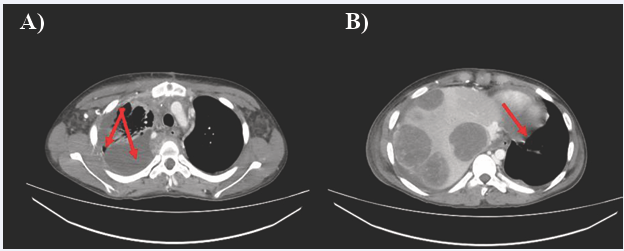
Figure 1 CT Scan chest with contrast, axial view a) indicating soft tissue density lesion in anterior mediastinum with collapsed lung causing b) contralateral mediastinal shift.
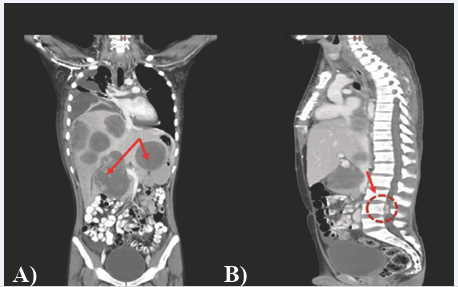
Figure 2 CT Scan chest, abdomen, pelvis with contrast a) coronal view: multiple hypodense lesions with specks of calcification in both lobes of liver (indicated by red arrow), b) sagittal view: the largest epidural component (2.3x1.1cm) along the L4 vertebra.
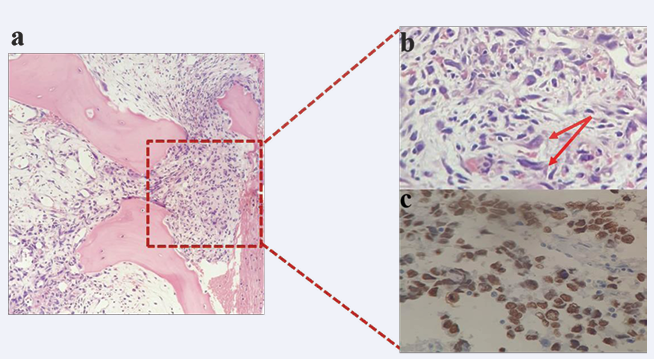
Figure 3 Bone marrow examination: a) Low power (10X) showing metastatic infiltration in bone marrow b) enlarged view (20X); red arrows indicating malignant cells c) immunohistochemistry for CKAE1/AE3 highlighting positivity in malignant cell.
Though the underlying molecular process involved in bone marrow metastasis was not ruled out some researchers have suggested that this dissemination is an outcome of malignant cell migration at the time of embryogenesis. Furthermore, it has also been proposed that the germ cells are widely distributed to various organs i.e. brain, bone marrow, thymus, and liver performing vital regulatory functions or are involved in the relay of immunological, genetic, or hematological functions. Nonetheless, in conclusion our data suggested atypical interaction between primary mediastinal YST and bone marrow cells, highlighting its clinical implications.
REFERENCES
1. Kattuoa Ml, Kumar A. Yolk Sac Tumors. Treasure Island, FL StatPearls. 2021.
7. Voss SD. Diagnostic Imaging in the Evaluation of Childhood Cancer. Oncology of Infancy and Childhood. 2009; 1015-1098.
10.Kakkar ?, Kaur K, Verma A. Pediatric mediastinal germ cell tumors. Mediastinum. 2019: 30.









































































































































{kind=link}