Return to the OR: A Case of an Extremely Rare Omental Ectopic Pregnancy
- 1. Department of Obstetrics and Gynecology, Inspira Health Network, USA
- 2. Inspira Health Urogynecology, USA
Abstract
We present a case of a 24-year-old gravida 2, para 1 woman at an unknown gestational age with an omental ectopic pregnancy. She had started bleeding three weeks prior and she assumed that was her last menstrual period. Initial working diagnosis was an aborted tubal pregnancy after the first diagnostic laparoscopy. It was then subsequently discovered to be omental in location during a second diagnostic laparoscopic procedure searching for its location, in the setting of persistently rising quantitative bHCG levels. We encourage diligent exploration of the abdominal cavity in the setting of pregnancy of unknown location, even when bilateral adnexa and the pelvis appear normal during surgical exploration.
Keywords
Omental ectopic; Abdominal pregnancy; Laparoscopy; Omentectomy
Citation
Chavez RS, Walsh S, Chong W (2022) Return to the OR: A Case of an Extremely Rare Omental Ectopic Pregnancy. JSM Clin Case Rep 10(1): 1195.
ABBREVIATIONS
OR: Operating Room, bHCG: beta Human Chorionic Gonadotropin, ER: Emergency Department, mmHg: millimeters of mercury, mIntlUnit/mL: milli- international units/milliliter, IV: Intravenous, mL: milliliter, IM: Intramuscular, mm: millimeter, cm: centimeter
INTRODUCTION
Ectopic pregnancy occurs in approximately 1.5% to 2.0% of all pregnancies [1]. Approximately 95% of ectopic pregnancies occur in the fallopian tube [2]. Abdominal pregnancy is rare and occurs in approximately 0.34% to 1.3% of all pregnancies, with only approximately 9% of those abdominal ectopics being found in the omentum [3]. Omental ectopic is a very rare occurrence. There were only 16 reported cases of primary omental pregnancy in the literature between 1958 to 2012 [4].
Abdominal pregnancy affects 1 in 10,000 deliveries [4]. Omental ectopic pregnancy is a rare, potentially life threatening, form of ectopic pregnancy with difficult diagnosis based on the pregnancy location. Prompt diagnosis and treatment is key during these cases. Ectopic pregnancy remains the leading cause of first trimester pregnancy-related death. Maternal mortality from abdominal pregnancy is 7.7 times higher than tubal ectopic pregnancy [1,3], most often from hemorrhagic shock secondary to rupture of ectopic pregnancy [1]. These statistics underscore the importance of timely diagnosis and management of an omental pregnancy.
CASE PRESENTATION
A 24-year-old gravida 2, para 1 at an unknown gestational age presented to the ER at another community hospital with 7 out of 10 severity abdominal pain that was associated with nausea and vomiting. It had started that morning with mild menstrual-like cramping and then evolved into severe pain. On arrival, her vital signs were stable and as follows: blood pressure 140/94 mmHg, heart rate 70 beats per minute, respiratory rate 16 breaths per minute, and temperature 36.9 degrees in Celsius. The ER physician described her presenting exam as having mild-moderate tenderness to palpation in the bilateral lower abdominal quadrants and suprapubic area without guarding or rebound. The pelvic exam is described as having a small amount of yellowish-green discharge, positive cervical motion tenderness, no bleeding, no adnexal tenderness, and no palpable adnexal masses. She was unaware of her pregnancy and pregnancy was diagnosed upon testing in the ER. She assumed the vaginal bleeding she had 3 weeks prior was her last menstrual period. A pelvic ultrasound was performed showing a large amount of complex fluid in the pelvis consistent with hemoperitoneum as well as bilateral adnexal lesions difficult to characterize with the largest being 4cm in size. Please see Figure 1 for sonographic findings.
The intake quantitative bHCG was 4,595 mIntlUnit/ mL on admission. Findings were consistent with a ruptured ectopic pregnancy, and she was transferred to our hospital for further gynecologic care. Upon arrival vital signs were as follows: blood pressure 105/63mmHg, heart rate 66 beats per minute, respiratory rate 16 breaths per minute, and temperature 37.1 degrees in Celsius. She was now complaining of 10 out of 10 severity abdominal pain. Her exam at this time revealed a non distended, diffusely tender abdomen that was soft to palpation, no guarding; with rebound tenderness noted which was greater on her right side in comparison to her left side. A pelvic exam was deferred at that time. In the ER she was given IV fluids, as well as IV ondansetron for her nausea, and IV hydromorphone for her pain.
The findings and initial assessment were discussed with the patient and the management options including diagnostic laparoscopy, possible open, with possible interventions including possible salpingectomy. Risks, benefits, and alternatives were discussed with the patient, and she agreed to proceed with diagnostic laparoscopy with possible interventions including salpingectomy. Consent forms were then signed with the patient with a witness present.
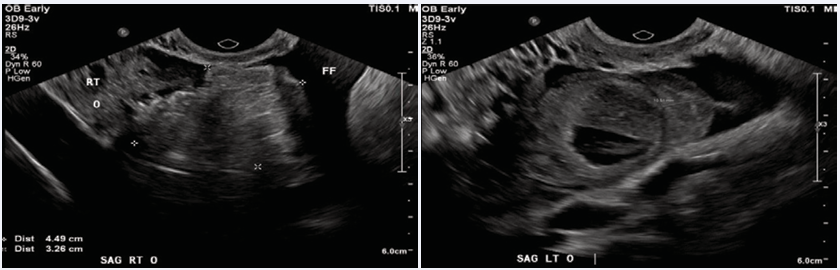
Figure 1 Sonographic findings via transvaginal ultrasound at the time of presentation. Left: Right ovary labeled as “RT O”. Free fluid labeled “FF”. The right adnexal mass measuring 4.49 cm x 3.26 cm marked by x around border. Right: Left ovary labeled “LT O”. Left adnexal mass noted at arrow. Free fluid labeled “FF”.
Upon entry into the intraperitoneal space, there was 450 mL of hemoperitoneum which was evacuated, however, an obvious gestational sac was not found in neither bilateral fallopian tube, bilateral ovaries, uterus, or anterior and posterior cul de-sacs. The overall appearance of omentum and bowels were normal without evidence of an ectopic. We conjectured that the ectopic pregnancy might have occurred at the fimbrial end of the fallopian tube and had ruptured or that a tubal ectopic pregnancy had spontaneously aborted from the tube in its entirety. The evacuated hemoperitoneum was sent to pathology to assess for chorionic villi in the event that the ectopic had been a spontaneously aborted tubal ectopic. As there was no obvious gestational sac found the procedure was terminated at this time and only diagnostic laparoscopy with evacuation of hemoperitoneum completed.
Considering high suspicion for ectopic pregnancy based on elevated bHCG level; patient’s clinical presentation; and no gestational sac seen intracavity of the uterus, the patient was admitted for close monitoring with serial quantitative bHCG levels with serial abdominal exams. Our new working diagnosis at this time was a pregnancy of unknown location.
The patient’s quantitative bHCG results continued to rise postoperatively. On postoperative day one it was 6,511 mIntlUnit/ mL and on postoperative day two it was 7,368 mIntlUnit/mL. The patient had increased pain on postoperative day two and a repeat pelvic ultrasound performed, which revealed a left adnexal echogenic mass concerning for ectopic pregnancy [Figure 2].
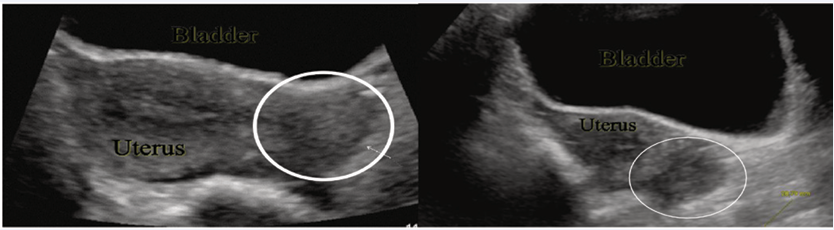
Figure 2 Sonographic findings via repeated transabdominal ultrasound on Postoperative Day 2. A 2.8cm left adnexal mass noted on left and right images.
No significant hemoperitoneum noted at this time.
Considering that pathology from the initial procedure was not yet available for review, decision was made to proceed for another diagnostic laparoscopy and dilation and curettage, after obtaining an informed consent from the patient. The uterine cavity was evacuated first via dilation and curettage, and then the laparoscopic portion of the procedure was performed. The trocars were placed through the incisions from the initial procedure. A 10mm trocar at the umbilicus was placed via an open method as well as two 5mm trocars 3cm superior and medial to the bilateral anterior superior iliac spines. Approximately 100 mL of hemoperitoneum was evacuated and again the same normal pelvic structures seen without evidence of ectopic. There was trailing clotted blood upward from the pelvis to the greater omentum. At this time the omentum was thoroughly inspected and the ectopic located in the greater omentum. See Figure 3 for the intraoperative findings of omental pregnancy.
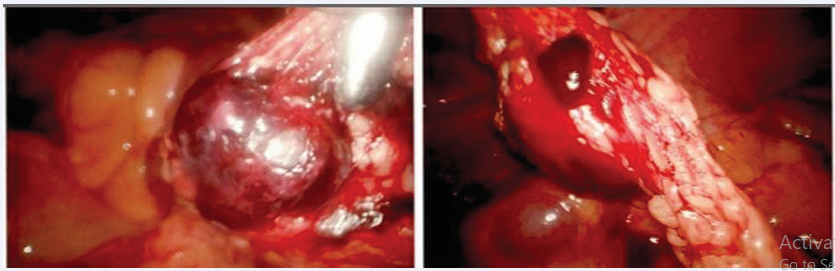
Figure 3 Ectopic pregnancy within the greater omentum.
A partial omentectomy was then performed by general surgery removing an
8.5 cm x 3.5 cm x 0.8 cm portion of omentum utilizing the LigaSure. The specimen was then placed into an Endo Catch bag and removed through the umbilical trocar site without having to extend the incision. The case was then concluded at this time. Minimal blood loss was noted, and the patient tolerated the procedure well.
Postoperatively, 100 mg IM Methotrexate (based on dosing of 50 milligrams per meters squared) was administered. Her subsequent recovery was uncomplicated, and she was discharged home the next day after reintervention. IM methotrexate after the conclusion of the second procedure was given because there was concern for persistent trophoblastic tissue remaining within the omentum although the likelihood was low. The patient was followed outpatient after discharge until her quantitative bHCG returned to nonpregnant levels to ensure that the ectopic pregnancy had been resolved in its entirety.
Final pathology for the first procedure showed blood clot only. The pathology from the second procedure showed the omentum with chorionic villi consistent with ectopic pregnancy and endometrial curettings with benign endometrium without evidence of chorionic villi or decidualized tissue.
DISCUSSION
Diagnosis and proper identification of omental ectopic pregnancy are often delayed because of the lack of presenting signs and symptoms [1]. There may not even be a delay in menstruation [4]. The most common symptom is severe lower abdominal pain [4]. In some cases, they do not involve vaginal bleeding, lower abdominal or pelvic pain, or reveal any adnexal masses through ultrasound examination, making it very difficult to diagnose [5].
The Studdiford criteria for a primary peritoneal (abdominal) pregnancy must include all three criteria: (1) bilaterally normal adnexa, (2) no uteroplacental fistula, and (3) early attachment of ectopic pregnancy to a peritoneal surface thus eliminating the possibility of secondary implantation after tubal abortion [3-6]. This case meets all Studdiford criteria for a primary abdominal pregnancy.
Current treatment interventions for ectopic pregnancy include surgical management and medical management with methotrexate. Case studies at this current time have utilized surgical management with partial omentectomy as treatment for omental ectopic pregnancy, most of which were laparotomy versus laparoscopy [1,3-6]. We utilized the laparoscopic approach initially considering the lower surgical morbidities and early recovery associated with laparoscopy compared to laparotomy. However, during the first laparoscopic survey, we were unable to identify the ectopic presence on omentum, since the omentum was displaced to the upper abdomen with Trendelenburg position for laparoscopic surgery. From managing this patient, we learned the importance of thorough abdominal survey (including running the bowels and omentum) at the time of intraabdominal entry, even if the ectopic appeared to be in the pelvis near the adnexa on pelvic ultrasound.
This case report is to remind obstetrics and gynecology providers of the difficulty in diagnosing and managing a pregnancy of unknown location when it occurs in a rare location, such as the omentum. Omental ectopic pregnancy is difficult to identify with imaging or surgical exploration. We also want to emphasize the importance of close monitoring and persistence in locating an abdominal ectopic, especially when there are signs of rupture. In addition to being difficult to locate physically, omental ectopic pregnancies do not always present similarly to an adnexal ectopic.
DECLARATION OF PATIENT CONSENT
The authors certify they have obtained the patient’s consent. The patient has given her written consent for her images and other clinical information to be reported in the journal. The patient understands her name and initials will not be published and due efforts will be made to conceal her identify, but anonymity cannot be guaranteed.
REFERENCES
2. Gala, RB. Chapter 7: Ectopic Pregnancy. In: Hoffman BL, Schorge JO, Bradshaw KD, Halvorson LM, Schaffer JI, Corton MM. eds. Williams Gynecology. 3edn. McGraw Hill; 2016.
6. Yip SL, Tan WK, Tan LK. Primary omental pregnancy. BMJ Case Rep. 2016.









































































































































{kind=link}