Sarcoidosis and Hypercalcemia: A Case Report
- 1. Tracheal Diseases Research Center, National Research Institute of Tuberculosis and Lung Diseases (NRITLD), Shahid Beheshti University of Medical Sciences, Iran
- 2. Chronic Respiratory Diseases Research Center, National Research Institute of Tuberculosis and Lung Diseases (NRITLD), Shahid Beheshti University of Medical Sciences, Iran
- 3. Department of Clinical Immunology and Allergy, National Research Institute of Tuberculosis and Lung Diseases, Shahid Beheshti University of Medical Sciences, Iran
Abstract
Sarcoidosis is a chronic, multi-systemic disease with granulomatous condition and unknown etiology. Hypercalcemia is an uncommon medical condition which may arise as a consequence of a reduced renal excretion, hyperparathyroidism and cancer. Here, we report a case of 50-years old man with renal failure associated with sarcoidosis. Clinical manifestation and histological sections are also presented.
Keywords
Hypercalcemia; Sarcoidosis; Renal failure
Citation
Kiani A, Abedini A, Yasari F, Mansouri D, Abooshahab R (2017) Sarcoidosis and Hypercalcemia: A Case Report. JSM Clin Case Rep 5(1): 1127.
ABBREVIATIONS
ESRD: End Stage Renal Disease; TBN: Thickness in Trabecular Number
INTRODUCTION
Sarcoidosis is a chronic and multi-systemic disease with unknown cause that can affect all organs of the body such as eyes, skin and lymph nodes; However lungs are the most commonly involved organ [1,2].
This disorder, which has been observed in all parts of the world, comprises all races and ages, but clinical symptoms and severity vary among different ethnic groups [2]. Considering various clinical appearance and the severity of the disease compared to other diseases, the diagnosis of non-specific sarcoidosis is based on clinical manifestations, computer imaging, physiological studies, pathological examinations (indicative of non-caseating granuloma), and the absence of mycobacterial or fungal infections [3]. Steroids are the preferred treatment for sarcoidosis, and in all cases there is no indication of treatment [4,5]. Hypercalcemia is a challenging condition that can occur in patient with sarcoidosis [6]. Here, we report a case with severe hypercalcemia, associated with sarcoidosis.
CASE PRESENTATION
In March 2017, a 50-year old man, a possible case of sarcoidosis with hypercalcemia was presented at Masih Daneshvari Hospital, complaining of drowsiness, weakness and confusions. The patient had no family history of other disease like autoimmune disease but had a history of diabetes, anemia and smoking. His serum calcium and creatinine levels were 15.2 mg/ dL and 3.2 mg/dL, respectively. The test results were sent to the emergency room (ER) for further diagnosis. The notable initial lab tests are shown in Table 1.
Table 1: Laboratory test in admission.
|
Table 1: Laboratory test in admission. |
||
|
Laboratory Data |
Value |
Normal Range |
|
FBS Urea Creatinine Na K Ca T4 T3 TSH PTH TG Albumin Vit D3
P |
112 mg/dl 141 mg/dl 3.2 mg/dl 139 mEq/lit 4.2 mEq/lit 10.2 mg/dl 5.22 micg/dl 0.48 micg/dl 1.91 micIu/ml 15 pg/mL 105 mg/dl 3.5 g/dl 16.3 ng/ml
4.6 mg/dl |
70-110 10-50 0.9-1.3 135-145 3.5- 5.3 8.6- 10.3 4.87-11.72 0.58-1.59 0.35-4.94 10-55 Up to 200 3.8-5.1 Deficiency <10 Insufficiency 10-29 Sufficiency 30-100 Toxicity >100 Adult: 2.5-5 Child: 4-7 |
|
Abbreviations: FBS: Fasting Blood Sugar; Na: Sodium; K: Potassium; Ca: Calcium; T4: Thyroxin; T3: Triiodothyronine; TSH: Thyroid - Stimulating Hormone; PTH: Parathyroid Hormone; TG: Triglyceride; P: Phosphorus. |
||
The patient was diagnosed with End Stage Renal Disease (ESRD) and admitted to the patient services. Ultrasound examination of kidney did not reveal any changes in size or any kidney stones. Kidney liver biopsy has shown fibrosis around the atrophic region with thickness in trabecular number (TBN) and serial section were stained with H&E, PAS, Trichrom Jones and Congo Red Method. Maximum number of nine well preserved glomeruli with no significant pathologic changes has been observed. For ESRD management, the patient has been given non-calcium dialysis fluid. Diary and calcium supplements were discontinued. Also this patient had multiple cervical, mediastina and abdominal laps and skin lesions and subsequently underwent diagnostic biopsy of lymph node and skin. Specimen consist of three lymph nodes creamy in color, measuring 3.5×3×2 cm, 3.5×2×1.5 cm and 2×1×1 cm. Lymph node reveals numerous granulomas, composed of epithelioid histocytes and multinucleated giant cells without central caseous necrosis which was distinctive feature of non-necrotizing granulomas. Other exams show no heart involvement in sarcoidosis. Following the diagnosis of sarcoidosis, corticosteroid (Dexamethasone) has been prescribed. With the onset of treatment, the patient’s serum calcium (Figure 1) and creatinine level show downtrend.
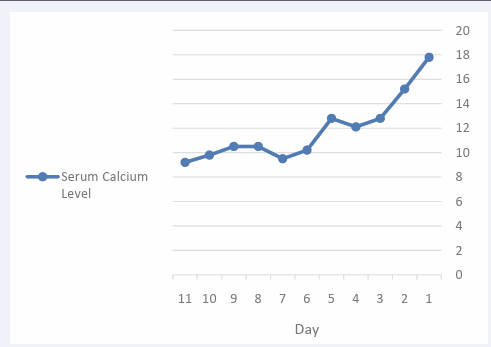
Figure 1 Electrospun nanofibers membrane of poly-ε-caprolactone visualization after 21 days of human Osteoblasts culture (Cells visualization in blue (nucleus /DAPI) and PLLFITC labelled nanofibers in green): colonization and proliferation of osteoblasts into the nanofibers membrane.
The latest creatinine was 2.1 mg/dl.
DISCUSSION
Sarcoidosis is a systemic, granulomatous disease with unknown etiology. Based on the literature reviews, hypercalcemia incidence in sarcoidosis is different [6,7]. Renal disease involvement in sarcoidosis can occur as a consequence of hypercalcemic nephropathy, granulomatous interstitial nephritis, glomerulonephritis, renal amyloidosis, or renal tubular dysfunction. Hypercalcemia can occur due to hyperparathyroidism, kidney impairment and malignancy [8]. But the exact mechanism leading to the increased levels of calcium is still not clear [9]. In 1939, Harrell et al. for the first time have reported hypercalcemia in association with sarcoidosis in six out of 11 patients diagnosed with sarcoidosis [10]. Also, high level of vitamin D3 has been seen in hypercalcemia associated with sarcoidosis. In 2012 and 2011, Hassler et al., and Amrein et al., respectively have reported that hypercalcemia was a consequence of Vitamin D supplementation in patient diagnosed with sarcoidosis [11,12].
Corticosteroid therapy is the first line to consider for hypercalcemia associated with sarcoidosis because it reduces the calcium level through the inhibition of osteoclast function and decrease of calcium absorption from the gastrointestinal tract [7].
In conclusion, we are reporting a patient with ESRD and hypercalcemia associated with sarcoidosis. Since the PTH level was normal, the initial diagnosis of hyperparathyroidism was rejected in regards to hypercalcemia, also based on the normal levels of phosphorus, secondary hyperparathyroidism was not a diagnosis and the kidney failure was attributed to hypercalcemia. Hypercalcemia is often asymptomatic, and diagnosis and treatment of sarcoidosis without pulmonary symptoms are often a challenging task. In this case, corticosteroid therapy was effective in hypercalcemia associated with sarcoidosis.
REFERENCES
2. Iannuzzi MC, Rybicki BA, Teirstein AS. Sarcoidosis. N Engl J Med. 2007; 357: 2153-2165.
6. Carmichael P, O’Donnell JP. The protean face of renal sarcoid. J Nephrol. 2003; 16: 721-717.
8. Jacobs T, Bilezikian J. Rare Causes of Hypercalcemia. J Clin Endocrinol Metab. 2005; 90: 6316-6322.
9. Lafferty F. Differential diagnosis of hypercalcemia. J Bone Miner Res. 2009; 6: 51-59.









































































































































{kind=link}