Serotonin Syndrome and the Emergence of New Legal Highs
- 1. Mid Cheshire Hospital Trust, UK
Abstract
A 47 year old man known to have been taking citalopram for several years was admitted with a mixed overdose of methadrone and the newer recreational drug (or ‘legal high’), NRG-3. He displayed signs and symptoms of serotonin syndrome which required treatment in the form of sedation and intubation and was admitted for a short stay on the Intensive Care Unit. He made a full recovery with no apparent physical or psychological sequelae and was discharged home after having a psychiatric review. The popularity and emergence of new ‘legal highs’ should alert the treating doctor to the possibility of various and largely unknown side effects. Many of the newer legal highs are molecularly related to each other and can be expected to share similar pharmacological properties, including their side effects and their propensity to precipitate a serotonin syndrome.
Keywords
Serotonin syndrome; Legal highs; Methadrone; NRG introduction
Citation
Doherty S, Ng P (2014) Serotonin Syndrome and the Emergence of New Legal Highs. JSM Clin Case Rep 2(1): 1011.
INTRODUCTION
‘Legal highs’ are increasingly popular synthetic drugs designed for recreational use. Newer legal highs are based on more familiar drugs such as methadrone (which was once legal) and chemically altered to offer a supposedly new alternative high. This has the convenience of bypassing the law as there is no legislation regarding these newer compounds. Many patients present to the Emergency Department with symptoms of intoxication from these drugs but little is actually known about their effects and how to best treat them. Furthermore, with the increasing number of designer drugs, a more varied presentation is inevitable. There is also no guarantee of knowing what is actually contained within the drug that is being purchased. The case reported here demonstrates the relationship between serotonin syndrome with methadrone and a newer compound, by the name of NRG-3, with concurrent chronic citalopram use.
CASE PRESENTATION
A usually fit and well 47 year old gentleman with a background of depression was seen in the Emergency Department. His partner had found him to be aggressive and agitated after reportedly taking methadrone and a drug called NRG-3, which he had purchased over the internet. He had been taking thesedrugs over the preceding 3 days for recreational purposes and he denied any suicidal ideation. He was also taking citalopram 20mg once daily as well as inhalers for asthma.
On examination, his blood pressure was 134/82mmHg but he was noted to be tachycardic with a heart rate of 122 beats per minute in sinus rhythm. He was flushed and pyrexial with a temperature of 40°C and respiratory rate of 30 breaths per minute. He was restless and agitated with spontaneous choreic movements of his limbs and trunk. Clonus was easily inducible and his reflexes were globally brisk. However, there was no muscle rigidity or hypertonia.
He was given a total of 25mg of IV diazepam to control the abnormal movements with no clinical effect or evidence of respiratory depression. An anaesthetic opinion was sought and he subsequently responded to 50mg of propofol which controlled the choreic movements but this also caused respiratory depression requiring intubation. His blood results showed a normal full blood examination and clotting, a creatinine kinase of 12,961 U/L but normal renal function with the exception of a raised urea of 13.4 mmol/L. His C-reactive protein was raised at 204 mg/L and he had a mild hypoglycaemia at 3.6 mmol/L. An arterial blood gas revealed he had a metabolic acidosis with a pH of 7.09 and bicarbonate of 15.7 mmol/L.
He was diagnosed with serotonin syndrome as per the Hunter Serotonin Toxicity Criteria and transferred to ITU [1]. He received supportive treatment which included intravenous sodium bicarbonate. He was extubated and stepped down toward level care after 2 days. He unfortunately had a further pyrexial episode of 38.8°C which was attributed to an infected central line, which was removed and IV antibiotics administered as per hospital guidelines. He was later seen by psychiatry liaison services and declared that he did not intend to use recreational drugs again. He also stated that in hindsight he suffered with visual hallucinations on admission. Coping strategies were put in place and he declined referral to counselling services. He was subsequently discharged.
DISCUSSION
Methadrone (also known as Meow Meow, M-CAT, white magic, meph, MC, drone, charge, bubble, bounce, 4-MMC) is a fine white/yellow powder that is either snorted or wrapped in paper and swallowed (i. e. ‘bombed’) but it may also be in the form of capsules or pills. It can also be smoked but is rarely injected. It may be sold as plant food or bath salts and labelled as ‘not for human consumption’ in order to bypass the law [2]. There have been only two case reports of serotonin syndrome associated with methadrone [3,4]. Nevertheless, the UK National Poisons Information Service does recognise serotonin syndrome as an effect of methadrone, the treatment of which is largely supportive with supplementary benzodiazepines to control sympathetic overdrive [5]. In 2010, the UK Advisory Council on the Misuse of Drugs banned certain derivatives of cathinones as they were recognised as stimulant drugs of abuse [6]. Despite this, many more drugs have still been derived and produced from the common basic structural compound and advertised as legal highs even after this generic ban and hence, although unknown to many, making them illegal (Figure 1).
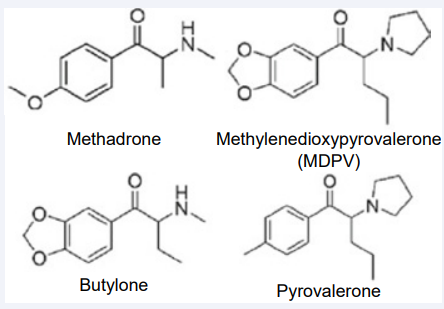
Figure 1 Common synthetic cathinones of abuse.
NRG-3 (napthylpyrovalerone, NPV) is a compound that is derived from naphyrone (also known as rave, NRG1, energy-1) [2]. Like methadrone, it is part of the cathinone family of chemicals and is therefore a Class B recreational drug under the UK law. It is the latest in the ‘NRG’ series of legal highs and the literature regarding NRG3 (or even any NRG compound) is scarce. In addition to this, many so called ‘legal highs’ are often contaminated with= other compounds that may already be illegal. In one case report for example, analysis of NRG1 was found to contain the two illicit drugs β-keto-N-methylbenzodioxolylpropylamine (butylone) and
methylenedioxypyrovalerone (MPDV) and not NPV as expected [7]. However, it would not be unreasonable to believe that these drugs could be contaminated with non-consumable compounds, which is common with other well established recreational drugs (such as brick dust with heroin and talc powder with cocaine).
Little is known about the effects of naphyrone and much of it assumed to be similar to other cathinones. There has been one case report specifically linking NRG-3 consumption with psychotic episodes on 3 occasions in the same patient [8]. There were no case reports exist linking naphyrone with serotonin syndrome. However, drugs that are contaminated with other chemicals of the same family could be expected to give an augmented presentation of adverse effects. It may be more challenging for the clinician when the patient presents with a mixed overdose. It would not be uncommon for patients to take these ‘legal highs’ with other stimulant drugs such as other amphetamines or cocaine, or other drugs of the same family as in this case. Concomitant use of alcohol may mask the sympathetic features of stimulant drugs and therefore the diagnosis of an overdose of these drugs may be missed or delayed. Nevertheless, with the case of serotonin syndrome, any features that would normally be present but masked with concomitant alcohol (or other depressive agents such as benzodiazepines) may actually not be present when the GCS returns to normal given the self limiting nature of serotonin syndrome. Treatment would remain supportive and includes intubation for airway protection. The use of flumazenil in a suspected mixed overdose is usually avoided to prevent precipitating any features of toxicity from other drugs of which serotonin syndrome is no exception.
Another challenge to the clinician is proving the abuse of these novel drugs. Historically, we are guided by the history obtained from the patient and/or friends as there is often no test to detect the use of these drugs. There are some centres in the USA who routinely test for certain cathinones but with the continuing introduction of new members of this family it is likely that a lot of these are not detectable as no standard is available. The current
detection method for these drugs is liquid chromatography and mass spectometry, which can be used on blood or urine samples [9].
The diagnosis of serotonin syndrome itself can be difficult to make. The presentation is due to excess serotonergic activity in the nervous system leading to mental status changes, autonomic instability and neuromuscular hyperactivity. This is usually caused by medications resulting in reduced serotonin reuptake, increased serotonin synthesis or direct serotonin receptor activation (such as antidepressants and tramadol - especially
when combined). It is likely that the recreational drugs in this case, in combination of the chronic use of a selective serotonin reuptake inhibitor, have further increased the availability of serotonin by one or more of these mechanisms. Serotonin syndrome may also be precipitated when drugs are started that inhibit the metabolism of a culprit drug (e. g erythromycin inhibiting CYP3A4 which metabolises sertraline) [10]. Although there is an increased diagnostic awareness, it is likely that serotonin syndrome often goes unrecognised and the true incidence is unknown. The diagnosis may be confused with neuroleptic malignant syndrome (NMS) and can be difficult to distinguish. However, NMS can often be distinguished by its slower onset (usually 7 days after introduction of an antipsychotic agent) and its lead-pipe or cogwheeling rigidity, which was missing in this case. NMS does not usually have myoclonus, hyperreflexia or diarrhoea as can often be found in serotonin syndrome.
Most cases of serotonin syndrome require removal of the offending drug and simple supportive treatment often requiring benzodiazepines to control agitation and tremor. Cyproheptadine is an oral serotonin 2A antagonist which may be useful for reducing severe symptoms but evidence regarding its effectiveness in serotonin syndrome is lacking. Chlorpromazine is an antipsychotic agent with anticholinergic properties which may help symptoms but again evidence is lacking and this is not often used as it is contraindicated in hyperthermic patients and can cause NMS. Further possible treatment options include neuromuscular paralysis, sedation and intubation [10]. These are often reserved for severe cases with significant hyperthermia and evidence of rhabdomyolysis.
CONCLUSIONS
- The list of so called ‘legal highs’ are growing since they are becoming easier to make and reproduce. They are increasingly popular because they are easy to access as they are legally sold in shops or over the internet and are relatively cheap.
- The physician should bear in mind that the chemical content of recreational drugs may not be consistent (and not necessarily made up of purely legal compounds), and may therefore give a variable clinical presentation.
- Serotonin syndrome is a recognised complication of methadrone and probably a complication of naphyronelike drugs (such as NRG)
- Removal of the precipitating drug (s) is the mainstay of treatment for serotonin syndrome. The patient may require admission for supportive treatment with benzodiazepines, cyproheptadine and/or sedation.









































































































































{kind=link}