Vipoma: A Rare Tumour, a Rarer Cause of Acute Diarrhoea
- 1. Department of Gastroenterology, Mater Dei Hospital, Malta
- 2. Department of Surgery, Mater Dei Hospital, Malta
Abstract
Vasoactive intestinal peptide tumours (VIPomas) are rare pancreatic neuroendocrine tumours with an estimated incidence of between 0.2 to 0.5 per million per year that usually present with a conglomerate of findings related to the excessive secretion of vasoactive intestinal peptide (VIP) including profuse watery diarrhoea, dehydration, hypokalemia and hypoclorhydria occasionally referred to as VIPoma syndrome. VIPomas are usually considered as a cause of chronic diarrhoea and the onset of symptoms is often described as insidious.
Here we present a patient who developed acute diarrhoea with typical symptoms and laboratory findings of a VIPoma, later radiologically and histologically confirmed. Despite demonstrating the typical features of severe watery diarrhoea, dehydration and hypokalemia our case was atypical in its rapidity of onset and progression of the clinical syndrome. In view of the acuteness in onset and severity of her biochemical derangements the patient ended up developing an unfavourable outcome despite the absence of metastasis and a relatively young age which are usually regarded as good prognosticators.
Keywords
Diarrhoea; VIPoma; Hypokalemia; Octreotide
Citation
Schembri J, Sammut L, Ellul P (2013) Vipoma: A Rare Tumour, a Rarer Cause of Acute DiarrhoeaJSM Clin Case Rep 1(1): 1007.
ABBREVIATIONS
VIP: Vasoactive Intestinal Polypeptide; VIPoma: Vasoactive Intestinal Polypeptide Tumour; GP: General Practitioner; CT: Computed Tomography; WDHA: Watery Diarrhoea, Dehydration, Hypokalemia, Achlorydria; MEN1: Multiple Endocrine Neoplasia1
CASE PRESENTATION
A 51 year old woman who was largely independent despite suffering from a congenital myopathy presented to us with a 2 week history of abrupt onset diarrhoea. Prior to the onset of symptoms, the patient had had a regular bowel habit and was used to opening her bowels once daily. The diarrhoea was getting progressively worse and by the time of admission she was opening her bowels 15 times per day and she had also developed vomiting in the preceding 24 hours. The patient had seen her general practitioner (GP) on her first day of symptom onsetand had been prescribed an oral rehydration solution. Routine full blood count and renal profile at the time were normal, but since she had failed to improve after 3 days of conservative management the GP prescribed a two week course of empirical ciprofloxacin 500mg twice daily and metronidazole 400mg three times daily for a possible infectious gastroenteritis.
Despite empirical antibiotics the patient’s symptoms had continued to worsen. She was now opening her bowels 20 times daily with frequent nocturnal episodes. She had also become intolerant to oral fluids, thus necessitating her referral to the emergency department. On presentation she denied any abdominal pain, fever, bleeding per rectum or any recent travel. She had noticed that there had been some weight loss but this could not be quantified. Apart for the antibiotics, she was on no other medications.
On examination the patient was dehydrated, tachycardic (pulse rate > 120 beats per minute) and hypotensive (systolic blood pressure < 90mmHg). Abdominal examination revealed non-specific tenderness without any rigidity or guarding. Bowel sounds were increased and there was no lower limb oedema.
Initial blood investigations on admission demonstrated severe hypokalaemia - 1.73mmol/L (3.5-5.1mmol/L), hyponatremia – 124mmol/L (135-145mmol/L) and hyperchloremia - 123mmol/L (98-106mmol/L). Renal function on admission was normal, with a urea of 2.70mmol/L, creatinine of 37umol/L and eGFR of 167mls/min/1.73m2. Serum albumin was of 48.5g/L with a corrected calcium level of 2.67mmol/L. Magnesium levels were low at 0.65mmol/L. Full blood count was also initially normal with a white cell count of 7.70x109/L, haemoglobin of 160g/L and a platelet count of 342x109/L. Arterial blood gas analysis demonstrated severe metabolic acidosis (pH 7.201) with a low bicarbonate level of 8.9 mmol/L. The remaining blood investigations including blood cultures did not reveal any significant abnormality. Stool samples for Clostridium difficile toxins, bacteria and parasites were also negative.
Immediate management entailed transfer to the high dependency unit with aggressive hydration via central line and magnesium, potassium and bicarbonate replacement. Despite of the above measures the patient’s general condition continued deteriorating and she was transferred to the intensive care unit min view of metabolic encephalopathy necessitating invasive ventilation.
Stool volume charting whilst in intensive care revealed that the patient was passing more than 5 litres of diarrhoea per day. Total body potassium depletion was very severe as the patient required a total of 1673mEq of potassium prior to correction of serum levels. Despite correction of serum levels maintenance potassium doses were still very elevated at 250mmol/L/day. She had also received a total of 1000mEq of bicarbonate via central venous catheter in view of the severe bicarbonate loss and subsequent metabolic acidosis. In view of the severity of her symptoms and electrolyte disturbances as well as non-specific physical findings on examination, a more obscure pathology was suspected and a computed tomography (CT) scan of the abdomen and pelvis was performed. This showed a large contrast-enhancing well defined mass within the tail of the pancreas measuring 60mm x 76mm and with focal necrotic changes (Figure 1).

Figure 1 Axial contrast-enhanced CT scan showing well defined, enhancing lesion in the tail of pancreas measuring 60x76mm in diameter with focal necrotic areas.
Since the imaging results and biochemical abnormalities were quite suggestive of a functional neuroendocrine tumour the lady was immediately commenced on subcutaneous octreotide, initially at a dose of 100mg every 6 hours and later increased to 200mg. This helped in decreasing the volume of diarrhoea to less than 1 litre per day as well as reducing the daily maintenance fluid and potassium requirements.
Blood investigations taken following the CT scan results later corroborated the diagnosis as serum VIP was in excess of >500pg/ml (normal <60pg/ml) and Chromogranin A was also elevated at 196ng/ml (normal <100ng/ml). A CT guided pancreatic biopsy (Figure 2) was performed and the histology definitively confirmed the diagnosis of a well differentiated neuroendocrine tumour in view of typical appearance (Figure 3) and strong synaptophysin positivity. Thus, the diagnosis of a VIPoma was made.

Figure 2 Selected image from the CT guided biopsy showing the co-axial 18G needle within the pancreatic lesion.
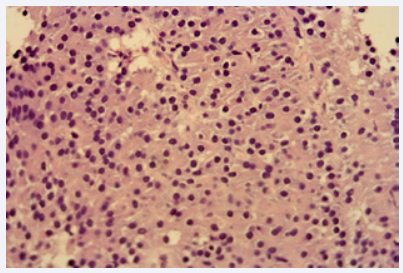
Figure 3 Pancreatic tail histology (hematoxylin and eosin staining) showing a well differentiated neuroendocrine tumour (G1). The biopsy shows solid sheets of neoplastic cells composed of relatively uniform cells with finely granular amphophilic and eosinophilic cytoplasm and a centrally located round to oval nucleus without distinct nucleoli.
Unfortunately, despite considerable improvement in biochemistry and daily stool volume our patient contracted ventilator associated pneumonia whilst in intensive care. This proved to be fatal as she succumbed to pulmonary sepsis after a 26- day hospital stay, 18 of which had been spent in intensive care.
DISCUSSION
The VIPoma syndrome was first described in 1958 by Verner and Morrison. It is thus also known as Verner Morrison syndrome or the WDHA syndrome, an acronym which stands for the profound chronic Watery diarrhoea, Dehydration, Hypokalemia and Achlorhydria which result from the excessive unregulated release of VIP by the tumour [1,2]. Adult VIPomas are usually pancreatic in origin, with rare cases caused by VIP-producing intestinal carcinoids, bronchial carcinomas, or phaeochromocytomas [3]. Mean age for adults at the time of diagnosis is 42 to 51 years and in some studies a female preponderance has been described. Other, even rarer, extra-pancreatic VIPomas have also been reported in the retroperitoneum, liver, oesophagus, and small intestine. VIPomas are usually large solitary tumours with less than 2% of them being multiple [4]. Despite this, various series have described the presence of metastasis in 29% to 78% of cases at the time of diagnosis or surgery [5,6].
VIP is a 28 aminoacid polypeptide which is not specific to the gastrointestinal tract and is widely distributed throughout the body. It functions as a neurotransmitter and in the gut helps to regulate blood flow by inducing vasodilatation, smooth muscle activity, pancreatic and intestinal secretions and inhibit gastric acid production. Its action on VIP receptors on intestinal epithelial cells stimulates intestinal water, sodium, potassium and chloride secretion as well as inhibiting resorption [7]. These results in the cardinal features of the syndrome which are the presence of severe secretory diarrhoea (89% to 100%) associated with hypokalemia (67% to 100%) and volume depletion (44% to 100%). The diarrhoea is typically large in volume and secretory in nature, with all patients having more than 1 litre and most more than 3 litres per day [8]. The hypercalcemia (41% to 50%) and
hyperglycemia (18%) that may occur are usually mild [3]. The mechanism of the hypercalcemia is unclear, and may be the result of the ability of VIP to stimulate bone osteolytic activity, however one must also exclude the possibility of coexistant primary hyperparathyroidism as part of MEN1 [9]. The hyperglycemia has been attributed to the glycogenolytic effect of VIP on the liver. The pathogenesis of the hypo- or achlorhydria, which frequently occurs in patients with the VIPoma syndrome, is not entirely clear, but has been attributed to the known inhibitory effect of VIP on gastric acid secretion [10,11].
Our case demonstrated all the typical biochemical findings including a severe hypokalemia. Not only is the serum potassium usually below 2.5mmol/L, but since 98% of total body potassium is intracellular, aggressive potassium supplementation is essential. Our patient required a total of 1673mmol/L of potassium (delivered as potassium chloride infusions via central venous line) prior to achieving a serum level above 3.5mmol/L. There are 2 main mechanisms for the severe hypokalemia. The first is due to faecal loss. A secondary factor may be the secondary hyperaldosteronism that results from VIP stimulation of renin release.
The long-acting somatostatin analogues such as octreotide are the drugs of choice to control the diarrhoea. Octreotide will control short- and long-term diarrhoea in 78% to 100% of patients with a VIPoma [4]. In patients who do not respond to the somatastatin analogues or in those in whom symptoms recur, the administration of glucocorticoids along with octreotide has proven to be effective in a small number of cases [3].Plasma VIP concentrations decreased in 80% to 89% of patients taking octreotide. However plasma VIP concentration with octreotide treatment does not always mirror the clinical responses. Data demonstrates that in patients whose diarrhoea subsided with octreotide, plasma VIP levels may return to normal, decrease but not to a normal range, fluctuate between normal levels to pretreatment levels or not change at all [12]. Surgical cure should be considered for all patients without metastatic disease. Systemic chemotherapy, long-term somatostatin analogs, interferon alpha, embolization and radiofrequency can be used in patients with unresectable tumours [13,14].
CONCLUSION
Despite our case having the typical features of VIPoma i.e. large volume diarrhoea, hypotension, dehydration, severe hypokalaemia, acidosis, mild hypercalcaemia and a positive response to a somatostatin analogue it diverges from the typical description of WDHA syndrome in the acuity of the patient’s symptoms. VIPomas are classically slow-growing, and previously reported cases consistently describe chronic diarrhoea and a slowly progressing constellation of associated symptoms. Our patient not only developed acute diarrhoea which progressed rapidly over a period of two weeks, but she also denied any related symptoms prior to diarrhoea onset. Literature review only revealed one other similar case, also in a similarly aged lady [15]. Another difference is that VIPomas usually carry a good prognosis, especially if there is no evidence of metastasis on presentation whereas our patient passed away within a month of symptom onset. Whereas this could be related to the patient’s underlying myopathy our case demonstrates that in the presence of acute diarrhoea with typical biochemical features one should still entertain the possibility of a neuroendocrine tumour, and institute appropriate investigations to prevent any treatment delays.









































































































































{kind=link}