Renal Cell Carcinoma Presenting as Pulmonary Embolism in a Patient with Hematuria-Management Challenges
- 1. Hospitalist-Internal Medicine, Genesis Health Care system, USA
- 2. Department of Hematology and Oncology, Genesis Health Care system, USA
- 3. Department of Pulmonary and Critical Care, Genesis Health Care system, USA
Abstract
Renal cell carcinoma is known to present as pulmonary embolism via tumor emboli with varied presentations. The literature sites various treatment modalities in the management of pulmonary embolism in the form of anticoagulation, thrombolysis, and surgical embolectomy. A 61 year old man who presented with hematuria and was diagnosed with pulmonary embolism and renal cell carcinoma posing a challenge in treatment is presented here.
Keywords
• Renal cell carcinoma
• Pulmonary embolism
• Hematuria
• Anticoagulation
Citation
Parmar R, Bastola S, Adamo J (2015) Renal Cell Carcinoma Presenting as Pulmonary Embolism in a Patient with Hematuria-Management Challenges. JSM Clin Oncol Res 3(1): 1045.
ABBREVIATIONS
RCC: Renal Renal Carcinoma; IVC: Inferior Vena Cava
INTRODUCTION
We report a case of a 61-year-old man who presented with hematuria and was diagnosed with a pulmonary embolism and renal cell carcinoma. The clinical situation posed several challenges in the management of his pulmonary embolism.
CASE PRESENTATION
A 61-year-old man with a history of hypertension and hypothyroidism presented to the hospital with gross hematuria, passing blood clots, and then developed urinary retention associated with abdominal pain. He denied chest pain, dyspnea, fever or cough. Physical examination was negative for any distress, clear lung exam, normal abdominal exam, and normal oxygen saturation.
Renal ultrasonography raised suspicion for a right renal mass and demonstrated a distended bladder with a Foley catheter in the place. The patient was seen by a urologist and underwent a retrograde pyelogram which showed a filling defect in proximal right ureter and right renal pelvis as well as lower portion of the right renal collecting system suspicious for multiple renal calculi. Computed tomography of the abdomen and pelvis revealed a pulmonary embolism in the posterior left lower lobe. CT also demonstrated diffuse abnormal heterogeneous appearance of the right kidney likely due to diffuse tumor replacement with tumor extension into the right renal vein partially extending into the inferior vena cava with mildly enlarged right pericaval lymph nodes, concerning for local metastasis.
Full anticoagulation was deemed unsafe because of heavy hematuria. Interventional Radiology was consulted to embolize the right renal artery which did stop bleeding temporarily after which a therapeutic dose enoxaparin was initiated. The patient started bleeding again and a second attempt to embolize was performed by the Interventional Radiologist but bleeding continued. It was unanimously decided to put patient on a prophylactic dose of enoxaparin while he underwent the remainder of his workup as the pulmonary embolism was not massive and the patient was hemodynamically stable. The patient was discharged home in stable condition after which he had a PET scan and was found to have no evidence of distant metastatic disease. He underwent nephrectomy and IVC thrombectomy. The histology of which confirmed renal cell carcinoma.
DISCUSSION
Pulmonary tumor embolism is a rare but well known cause of pulmonary embolism. Pulmonary tumor emboli are believed to arise from seeding of solid tumor into systemic circulation [1]. Renal cell carcinoma is a common solid tumor causing pulmonary emboli usually by direct extension (Figure 1)
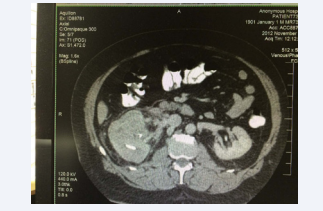
Figure 1 CT scan showing right sided renal mass
to renal vein and eventually to IVC [2]. This presentation can appear at any stage of RCC, sometime before the diagnosis where pulmonary embolism.
Different management modalities have been tried for pulmonary embolism with RCC. The first case was described in 1977 in which patient underwent surgical embolectomy [2]. There is a recent case report of RCC presenting as a massive pulmonary embolism (Figure 2)
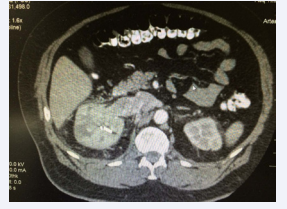
Figure 2 CT scan showing right sided renal mass.
extending to right heart where patient underwent thrombolysis [4]. Definitive treatment of RCC in the presence of intravascular tumor is surgical resection of tumor and thrombectomy which would improve the long term survival and prevent recurrent emboli [5]. Anticoagulation may be needed before surgery in presence of pulmonary embolism (Figures 3, 4)
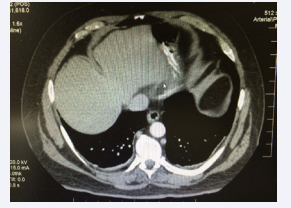
Figure 3 CT scan showing left sided filling defects.
Figure 4
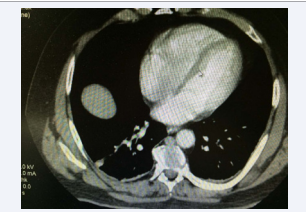
Figure 4 CT scan showing left sided filling defects
which could be challenging setting of severe hematuria or other bleeding [5-7]. As described in our case, if a patient has hematuria in presence of RCC and pulmonary embolism, management choices are limited and embolization of the kidney by interventional radiology is an option.









































































































































