Ultrasound-Based Evaluation and Dermoaesthetic Recommendations for Secondary Lymphedema after Mastectomy for Breast Cancer
- 1. Department of Physical Medicine and Rehabilitation, Local Health Authority of Taranto (ASL Taranto), Italy
- 2. Ambulatory Service of Aesthetic Medicine for Psychophysical Well-Being in Pathology Isola Tiberina Hospital-Gemelli Isola, Italy
- 3. International School Carlo Alberto Bartoletti Foundation, Italy
Abstract
Background: Breast cancer–related lymphedema is a frequent and disabling condition that affects function, skin quality, and psychological well-being. Early identification of tissue alterations is essential to improve management and prevent chronic fibrosis. This study aimed to develop an integrated aesthetic-medicine check-up combining clinical assessment, instrumental skin evaluation, and high-resolution ultrasound to support early diagnosis, objective stratification, and personalized cosmetological recommendations. Methods: Fifteen women with unilateral upper-limb secondary lymphedema after mastectomy underwent a standardized protocol including clinical examination, palpatory assessment, skin-instrumental measurements (corneometry, sebometry, pH, transepidermal water loss), and high-resolution ultrasound of the dermo-epidermal complex and subcutis across 17 limb sectors. Ultrasound findings were classified into normal, fluid, sclerotic, or undifferentiated patterns and compared with clinical severity. Results: Ultrasound detected dermal and subcutaneous alterations even in subclinical stages, revealing increased thickness, fluid patterns, and fibrotic changes. All patients showed reduced hydration, low superficial lipids, and increased transepidermal water loss, suggesting impairment of the skin barrier. More advanced stages were associated with sclerotic or undifferentiated ultrasound patterns, while early stages presented mostly normal or fluid profiles. The integrated evaluation enabled tailored cosmetological prescriptions, which improved patients’ skin comfort and supported rehabilitative strategies. Conclusions: Combining high-resolution ultrasound with dermo-aesthetic assessment enhances diagnostic accuracy and provides objective criteria for stratifying lymphedema severity. Personalized cosmetological interventions, guided by instrumental data, may support early management and contribute to improved quality of life after breast cancer treatment. This integrated model is consistent with current multidisciplinary recommendations and may represent a valuable addition to oncologic rehabilitation pathways. Simple Summary: Lymphedema of the arm is a frequent and debilitating consequence for women who undergo breast cancer surgery. It can cause swelling, discomfort, changes in the skin, and a strong impact on quality of life and body image. This study presents a new integrated check-up that combines clinical examination, instrumental skin measurements, and high-resolution ultrasound to identify early signs of lymphedema and guide personalized cosmetic recommendations. Ultrasound can reveal tissue changes even before visible swelling appears, allowing timely interventions that may prevent the condition from worsening. By analyzing skin hydration, lipids, pH, and water loss, the check-up also helps to create individualized skin-care programs aimed at improving comfort and supporting the skin barrier. This approach highlights how combining medical and dermo-aesthetic evaluation can provide more complete care for women after breast cancer treatment.
Keywords
• Breast Cancer • Cosmetology • Dermo-Aesthetic Evaluation • Lymphedema • Rehabilitation • Skin Barrier • Ultrasound
Catitions
Ariani M, Bartolefli E, Cavalieri L (2026) Ultrasound-Based Evaluation and Dermoaesthetic Recommendations for Secondary Lymphedema after Mastectomy for Breast Cancer. JSM Clin Oncol Res 14(1): 1078.
ABBREVIATIONS
AU: Arbitrary Units; BC: Breast Cancer; BCRL: Breast Cancer–Related Lymphedema; DEC: Dermo-Epidermal Complex; F-DEC: Fluid Dermo-Epidermal Complex; F-SUBC: Fluid Subcutis; HRUS: High-Resolution Ultrasound; ISL: International Society of Lymphology; M-DEC: Mixed/ Undifferentiated Dermo-Epidermal Complex; MRI: Magnetic Resonance Imaging; N-DEC: Normal Dermo Epidermal Complex; N-SUBC: Normal Subcutis; PRP: Platelet-Rich Plasma; S-DEC: Sclerotic Dermo-Epidermal Complex; S-SUBC: Sclerotic Subcutis; SPF: Sun Protection Factor; SUBC: Subcutis; TEWL: Transepidermal Water Loss; US: Ultrasound
INTRODUCTION
Growing attention to the quality of life of oncology patients has made aesthetic medicine a key supportive discipline in the post–breast cancer rehabilitation pathway. Among the most frequent and disabling complications is secondary lymphedema, which, in addition to causing functional impairment, has a profound impact on body image and psychological well-being. Lymphedema is one of the most common and debilitating complications after surgical treatment of breast cancer. It presents as an accumulation of lymphatic fluid in the ipsilateral upper limb and may evolve—if inadequately managed—into skin thickening, fibrosis, and functional limitation. Beyond the clinical aspects, lymphedema deeply affects self perception and psychological health. In recent years, focus has shifted from a purely therapeutic approach to a broader perspective that considers quality of life and body image. In this context, aesthetic medicine and cosmetology play a relevant role: the skin of a woman who has undergone breast surgery is not merely an outer “envelope” but a dynamic organ whose balance influences self-esteem and social relationships. International literature highlights that daily skin care, combined with targeted treatments, can improve comfort, prevent complications, and support psychophysical recovery. From this perspective emerges the idea of developing an integrated cosmetological check up combining traditional medical evaluation with precision tools such as ultrasound and personalized cosmetological prescriptions. High-resolution ultrasound is now a reliable and reproducible tool for evaluating superficial tissues (dermo-epidermal complex and subcutis). When integrated into an aesthetic-medicine check-up, it allows for an early detection of clinical and subclinical changes, guiding the selection of personalized preventive and therapeutic strategies. The rationale of this study is therefore to propose an aesthetic check-up model integrated with ultrasound capable of providing an objective assessment and a scientific basis for subsequent aesthetic-medicine prescriptions, following international recommendations [1–5]. Secondary lymphedema in breast cancer is a direct consequence of impaired lymphatic drainage following oncologic surgical procedures, particularly sentinel lymph node biopsy and, more commonly, complete axillary lymph-node dissection. The removal of these structures, with or without radiotherapy, disrupts the main lymphatic collectors of the arm, resulting in mechanical drainage insufficiency and subsequent accumulation of protein-rich interstitial fluid [3-6].
Epidemiology of Breast Cancer and Definition of Lymphedema
Breast cancer is the most common malignancy in women, affecting 1 in 8 women over a lifetime and accounting for approximately 29% of all female cancers. Incidence is highest in adult and older age groups, although an increasing trend is also observed among younger women. The disease is very rare in men, representing 1–2% of all diagnoses, with incidence increasing with age. Advances in diagnostics and therapy have improved survival, yet long-term treatment-related complications significantly affect patients’ quality of life [7,8]. Lymphedema is a chronic, progressive, and degenerative condition arising from partial impairment of lymphatic transport capacity. According to the International Society of Lymphology, it may involve skin, subcutaneous tissues, muscles, bones, nerves, joints, and internal organs, producing variable degrees of severity. Lymphedema is characterized by the accumulation of protein-rich interstitial fluid due to impaired lymphatic drainage. In oncology, secondary lymphedema is among the most common and disabling complications of breast cancer. Clinical classification is based on progressive stages (subclinical, reversible, irreversible, elephantiasis), while modern systems also consider tissue and fibrotic components, which are useful for guiding therapeutic decisions.
• Clinical and Instrumental Diagnosis of Lymphedema
Diagnosis relies on clinical criteria (inspection, palpation, limb-circumference measurement, water displacement volumetry) and instrumental methods. Among these, lymphoscintigraphy and MRI enable assessment of lymphatic dynamics but are less practical in routine settings. High- resolution ultrasound, by contrast, provides direct visualization of the dermo-epidermal complex and subcutis, offering rapid, reproducible data that are easily integrated into clinical practice [2-4].
Complications of Oncologic Treatments: Focus on Lymphedema
Among the most significant complications of surgical and radiotherapeutic treatments is secondary upper-limb lymphedema, a condition characterized by protein-rich fluid accumulation in the interstitial tissue with physical, functional, and aesthetic repercussions. Lymphedema may arise even years after undergoing an oncologic treatment and, if not recognized early, tends to become chronic, causing pain, functional limitations, and psychological distress. It is more accurate to refer to chronic edema (not to be confused with acute edema, a temporary post-traumatic fluid accumulation), defined as interstitial fluid accumulation lasting at least 3 months due to dynamic or mechanical lymphatic insufficiency. Dynamic (functional) lymphatic insufficiency refers to conditions where fluid accumulation results from increased capillary filtration despite a structurally intact lymphatic system. Causes include venous insufficiency, inflammatory processes, and conditions altering oncotic pressure (e.g., hypoalbuminemia). Dynamic insufficiency may evolve into mechanical insufficiency. Mechanical lymphatic insufficiency refers to structural damage— primary or acquired—of the lymphatic system. Beyond a critical threshold of capillary filtrate, intrinsic lymphatic dysfunction prevents adequate reabsorption. Persistent interstitial stagnation triggers mechanotransduction processes stimulating fibroblasts to produce collagen fibers, leading to tissue sclerosis and preadipocyte proliferation.
• Classification
Several classification systems exist, each emphasizing different aspects. When the etiology is considered, lymphedema may be classified as primary, secondary, or mixed. From a pathogenetic perspective, it may be classified as functional/overload (dynamic insufficiency) or mechanical insufficiency.
• Staging
Multiple staging systems have been proposed, though none has achieved universal consensus, as no single system is considered fully comprehensive. The most widely used is the International Society of Lymphology staging system, which divides lymphedema into four stages based on clinical and instrumental criteria:
Stage 0 / Ia: Subclinical stage in which edema is not clinically detectable, although patients may report suggestive symptoms and instrumental findings may be present. This stage may persist for months or years before becoming clinically evident.
Stage I / Ib: Edema is visible and may regress during the day or with limb elevation; pitting may be present.
Stage II: Persistent, non-reversible edema with pitting; tissue changes and fibrosis modify skin consistency.
Stage III: The limb is markedly deformed by lymphostasis, with non-pitting edema due to advanced tissue fibrosis; cutaneous alterations may also be present.
Diagnosis
Diagnostic work-up should include detailed medical history, careful physical examination, and instrumental support. Risk factors such as previous malignancies, adjuvant or neoadjuvant radio- chemotherapy, and potential exposure to infectious agents (e.g., tropical travel) must be investigated. A positive family history may suggest hereditary forms, while associated signs and symptoms can indicate syndromic presentations. Patients with lymphedema report symptoms varying with severity, including heaviness, swelling, tightness, discomfort, and functional limitations. In severe cases, skin discoloration, thickening, and pruritus may also occur. A thorough clinical evaluation involves the assessment of morphological contours: reduced visibility of extensor tendons, superficial venous network, and bony prominences (e.g., knuckles, styloid processes in the upper limb). Surgical scars must be examined, as dystrophic or adherent scars may impede lymphatic return. Factors such as radiotherapy, aromatase inhibitors, surgical technique, weight gain, and age can affect one’s range of motion, particularly at the shoulder. In advanced stages, cutaneous signs of fibrosis may develop, including hyperkeratosis, lymphatic cysts, lichenification, and accentuation of the dermal papillae (peau d’orange). Potential complications should also be carefully assessed.
On palpation, characteristic findings include:
- Consistency
Texture varies with severity. Early stages show soft tissue due to fluid accumulation. With fibrosis affecting skin and subcutis, tissue becomes firm or woody. A grading scale may be used [Figure 1]:
Grade 0: normal
• Grade 1: elastic
• Grade 2: fibro-elastic
• Grade 3: fibrotic
• Pitting Edema Scale:
Assessed by maintaining pressure for at least 10 seconds and evaluating the depth and persistence of the indentation:
- Grade 1: <2 mm, immediate rebound
- Grade 2: 2–4 mm, disappears within seconds
- Grade 3: 4–6 mm, disappears within 10–12 seconds
- Grade 4: 6–8 mm, persists >20 seconds
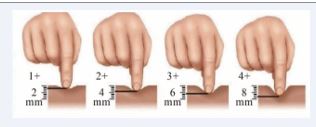
Figure 1 Pitting sign.
Skin Foldability: also known as the Stemmer test, it consists of assessing the increase in cutaneous foldability— normally difficult to detect—at the dorsal aspect of the proximal phalanx of the second toe or finger. In the early stages of lymphedema, foldability appears increased due to the presence of fluid layers within the dermis and subcutis; in more advanced stages, however, fibrotic degeneration leads to reduced foldability. In some cases, the assessment of foldability may be extended to the entire limb [Figure 2]. Volumetric measurements: that is, the assessment— using a measuring tape—of any increase in the size of the body region affected by lymphedema. The assessment involves multiple anatomical reference points. For the upper limb, the first measurement is performed at the level of the hand, using the figure-of-eight measurement technique. The second measurement is taken at the level of the distal wrist crease, used as a reference point because it tends not to disappear even in the most severe cases of obesity. From this landmark, subsequent measurements are taken every 5 cm in a distal-to-proximal direction. According to the new guidelines, however, other parameters are now preferred. Regarding simple circumferential measurements, an increase of at least 2 cm compared with the healthy contralateral limb at any single reference point is considered indicative of lymphedema. These measurements also make it possible to compare the percentage volumetric variations—again relative to the healthy contralateral side. Instrumental examinations: Although medical history and physical examination are generally sufficient for the diagnosis of lymphedema, integrating first- or second-level instrumental assessments is often valuable—particularly to clarify ambiguous cases, better define disease severity, and differentiate among potential etiologies.
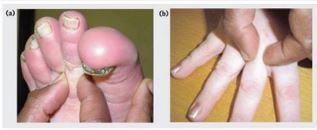
Figure 2 Stemmer test a-b.
The most commonly used instrumental examinations include:
- High-resolution ultrasound
- Doppler ultrasound: useful for evaluating the deep venous system
- Lymphoscintigraphy: useful for assessing superficial and deep lymphatic vessels and lymph nodes and therefore considered the gold standard for diagnosing lymphatic abnormalities.
For the diagnosis of lymphedema, at least one clinical criterion and one suggestive lymphoscintigraphic finding are required. This technique involves the injection of a radiotracer into the subcutaneous tissue at the first interdigital space of both hands or feet, depending on the location of lymphedema; the radiopharmaceutical is typically administered in two low-dose injections (thus carrying very low risk of ionizing radiation exposure and allergies). As it follows the lymphatic pathways, it reveals outflow obstructions through gamma-camera detection. The main limitation of this technique is insufficient standardization, as protocols differ regarding the radiotracer dose, injection site, and physical activity required during the exam. For preventive purposes, lymphoscintigraphy is recommended for patients at high risk of subclinical secondary lymphedema (e.g., after major lymphadenectomy at the limb root) and for relatives of patients with primary lymphedema.
- Lymphography: usually performed with direct oily contrast; rarely used today except in specific situations such as congenital or acquired disorders of the chylous vessels, cisterna chyli, or thoracic duct
Bioimpedance analysis: a technique that correlates variations in electrical conduction velocity with tissue composition; it enables the detection of subclinical lymphedema by identifying even minimal compositional changes in the limb. Recent studies suggest that bioimpedance analysis, when normalized to limb length, may provide a standardized outpatient protocol for the quantitative assessment of unilateral lymphedema, offering greater reliability than simple circumferential measurements.
- Perometry: a technique that uses infrared light beams to assess limb volume; it is extremely rapid, accurate, and reproducible, and is primarily used in specialized centers
- MR lymphangiography: particularly when using fat-suppression digital subtraction techniques, it can provide important information in advanced obstructive cases where lymphatic pathways appear dilated and filled with lymph
- CT lymphangiography: also used in complex cases involving vessel or cisterna chyli abnormalities
- Water-displacement plethysmography: considered the gold standard for calculating limb volume and the only reliable method for measuring edematous hands and feet. The principle is that a submerged body displaces a volume of water equal to its own. However, practical limitations— such as hygiene concerns — restrict its use
- Filarial antigen card test: used to detect Wuchereria bancrofti infection (Bancroftian filariasis), and therefore a possible infectious etiology of lymphedema, by identifying antibodies in individuals who live in or have traveled to endemic areas
- Genetic testing: identifies the most frequent mutations associated with familial primary lymphedema (e.g., FOXC2, VEGFR-3, SOX18).
Aesthetic and Functional Impact of Oncologic Treatments
Oncologic therapies (surgery, radiotherapy, chemotherapy, hormone therapy) induce cutaneous, scar-related, musculoskeletal, and metabolic alterations. Patients may experience skin dryness, rash, alopecia, nail changes, fibrosis, and lymphedema—all of which, in addition to impairing function, can profoundly affect body image and self-esteem. For this reason, aesthetic and functional recovery is an integral component of oncologic rehabilitation [1].
Multidisciplinary Approach: Oncology, Physiotherapy, Dermatology, Aesthetic Medicine
Recent literature emphasizes the value of a multidisciplinary approach integrating oncology, dermatology, physiotherapy, nutrition, reconstructive plastic surgery (aimed at restoring anatomical and functional integrity), and aesthetic medicine, which focuses on minimally invasive and dermo- aesthetic treatments to improve skin quality and body image. International recommendations propose safe, personalized dermo- aesthetic interventions to improve the quality of life of breast cancer patients. These include the management of cutaneous toxicities [9,10], physiotherapy for lymphedema prevention and treatment, reconstructive techniques, and minimally invasive aesthetic therapies—all in close collaboration with the referring oncologist.
Basics of Ultrasound
Ultrasound imaging is a highly versatile and easy to-use diagnostic technique that employs mechanical waves—ultrasound—to generate digital images. Diagnostic ultrasound typically uses frequencies ranging from 2–3 MHz to 20 MHz. These waves propagate through tissues via cycles of compression and rarefaction at speeds determined by the physical properties of the medium. They are generated by the transducer, a component of the ultrasound machine that contains a piezoelectric material, which changes shape in response to an applied electrical potential [Figure 3].
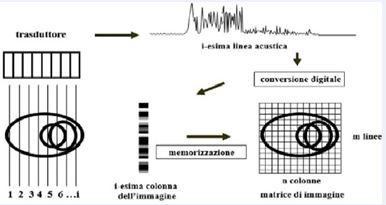
Figure 3 Schematic representation of the ultrasound image acquisition process.
When ultrasound waves encounter tissues with different impedance—a physical property related to tissue density—a portion of the waves is reflected and captured by the ultrasound system. In other words, impedance variations, known as interfaces, are detected, and converted into an analog signal, with depth represented on the x-axis and signal amplitude (in dB) on the y-axis. The analog trace is then converted into a digital signal in which each characteristic corresponds to white, black, or a shade of gray in the final image.
-
- Ultrasound of Healthy Superficial Tissues
Typically, probes used for the assessment of the skin and subcutis operate at a frequency of 20 MHz, although an accurate ultrasound examination can be performed with any probe of at least 15 MHz. Frequencies higher than 20 MHz, despite offering potentially greater detail, allow for reduced tissue penetration. Standard ultrasound systems are used, without requiring dedicated software.
Ultrasound imaging of superficial tissues allows for the visualization of :
- Epidermis, the outermost layer, which appears as a thin, uniform hyperechoic line.
- Dermis, located deeper, which appears as a hyperechoic band (although less hyperechoic than the epidermis), with thickness varying according to the anatomical region. The dermis comprises a more superficial papillary dermis, which is more hypoechoic due to its high water content, and a deeper reticular dermis, which is more hyperechoic because of the density and orientation of collagen fibers. The epidermis, papillary dermis, and reticular dermis together form the dermo-epidermal complex (DEC).
- Hypodermis/subcutis (SUBC), the innermost layer, clearly separated from the DEC by the dermo- hypodermal junction, a continuous, well-defined line reflecting the structural differences between the dermis and hypodermis. The hypodermis appears hypoechoic, organized into lobules, and intersected by thin horizontal or oblique hyperechoic lines representing connective-tissue septa (scaffolds) through which lymphatic vessels run. These septa tend to be parallel to the muscular fascia and may form interconnections with it. The end of this layer is marked by the beginning of the muscular layer, and its thickness varies according to anatomical site and adipose-tissue content.
A proper evaluation of superficial tissues should also include the generous application of gel and the use of minimal pressure during probe manipulation. These precautions help prevent excessive deformation of the underlying tissues, allowing for an accurate visualization of structures without operator-induced artifacts [Figure 4].
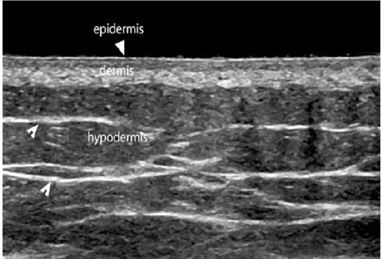
Figure 4 Ultrasound of superficial tissues in a healthy subject. The hyperechoic epidermis, the hypoechoic papillary dermis, and the hyperechoic reticular dermis can be identified, as well as the hypoechoic hypodermis traversed by hyperechoic fibrous septa.
-
- Ultrasound of Superficial Tissues in Patients with Lymphedema
The rationale for the ultrasound assessment of
superficial tissues in patients with lymphedema does not lie in identifying intrinsic damage to the lymphatic system itself, as the resolution of standard ultrasound equipment used for this type of examination does not allow direct visualization of lymphatic vessels. Specifically, when affected by disease, the deeper canalicular component containing lymphatic collectors may become visible due to dilation and disruption of the fibrous scaffold; however, the subepidermal lymphatic plexus cannot be directly evaluated.
The objective, therefore, is to identify indirect tissue alterations that reflect lymphatic dysfunction, such as differences in echogenicity and thickness of the various layers of the skin and subcutis. In unilateral lymphedema, the healthy contralateral limb is always used as a point of comparison; in bilateral cases, previous examinations serve as the reference point.
Although the number of studies evaluating the role of ultrasound in lymphedema is still limited, several have laid the groundwork for its systematic use in clinical assessment. Of particular relevance is the study by Tassenoy et al., an observational study involving seven women with unilateral breast cancer who developed lymphedema. Limb volume increase was measured using water- displacement plethysmography, and ultrasound findings were correlated with MRI to assess tissue- structure changes [8].
Similarly, the retrospective study by Suehiro et al. examined 35 patients with secondary lower-limb lymphedema by evaluating the skin and subcutis at eight standardized points. In the subcutaneous tissue, three grades of echogenicity were identified. This study highlighted that variations in tissue echogenicity correlate with lymphedema stage according to the International Society of Lymphology, and that such evaluation is feasible using probes operating at 11 MHz [11].
One of the most influential studies demonstrating the feasibility of a standardized ultrasound assessment protocol in lymphedema was conducted by Mander et al. This study precisely identified distinct ultrasonographic patterns representing progressive histological degeneration in the dermo-epidermal complex (DEC) and subcutis (SUBC) of the upper limb after mastectomy. These findings laid the foundation for a more objective evaluation of lymphatic-system compromise [12,13].
Based on Mander’s work, characteristic ultrasound patterns can be identified in both the dermo- epidermal complex and the subcutis, each reflecting progressive stages of histological alteration. Specifically, for the dermo-epidermal complex, the following patterns may be observed:
- Dermal edema
This condition is characterized by increased DEC thickness and reduced echogenicity (hypoechoic dermis). It is caused by the dilation of the subepidermal lymphatic plexus, leading to leakage of fluid into the dermal interstitium and the formation of vessel-like structures between collagen bundles lacking endothelial lining (a phenomenon known as dermal backflow). The papillary dermis is typically affected earlier than the reticular dermis due to differences in vascular and lymphatic distribution and collagen architecture.
Some authors suggest an association between dermal edema and paresthesias, attributed to stretching and irritation of sensory nerve endings.
This acute-stage pattern is sonographically identified as F-DEC (fluid dermo-epidermal complex).
- Dermal sclerosis with infiltrative changes
This pattern shows a marked increase in DEC thickness, increased echogenicity (hyperechoic dermis), and loss of the typical trilaminar DEC structure. These findings are due to cellular infiltration and early collagen-fiber deposition.
This pattern reflects a subacute or evolving stage and is identified as S-DEC (sclerotic dermo- epidermal complex). It is considered partially reversible.
- Dermal sclerosis with fibrotic involution
This condition is characterized by the loss of the dermo-hypodermal interface, resulting in a homogeneous echogenic appearance across tissues, making it difficult or impossible to accurately measure individual layers. These changes are due to chronic collagen deposition, ultimately leading to dermal fibrosis.
This chronic, irreversible stage is identified as M-DEC
(mixed or markedly sclerotic dermo- epidermal complex).
The normal pattern of the dermo-epidermal complex is labeled N-DEC. Regarding the subcutaneous tissue, the following patterns may be observed:
- Dilation of lymphatic ducts
In this condition, the hyperechoic signal of the fibrous connective septa disappears and the subcutis becomes globally thickened. This disappearance is due to the dilation of the lymphatic collectors running within the
fibrous strands, which leads to a marked separation of the adipose lobules (a cobblestone appearance). In some cases, dilated lymphatic collectors may cause a rupture of the fibrous septa, resulting in the formation of so-called lymph lakes. Unlike dilated lymphatic collectors, lymph lakes collapse under pressure from the ultrasound probe.
This pattern isidentifiedas F-SUBC(fluid subcutaneous).
- Edema and infiltrative phenomena of adipose lobules
This condition is characterized by increased echogenicity of the subcutaneous tissue, poor visualization of the fibrous framework, and overall thickening of the subcutis. It is caused by an infiltration of fluid and cells into the stromal component of adipose lobules—i.e., at the intercellular level— resulting in a sclerotic-edematous appearance known as “snow-fall”. In addition, mechanical pressure within the lobules may lead to the formation of a network of microscopic fissures in which fluid can accumulate.
- Subcutaneous sclerosis with fibrotic involution
This condition shows increased echogenicity and reduced thickness of the subcutis. It results from the replacement of adipose lobules with fibrotic tissue and collagen fibers, producing a fibro- sclerotic pattern. When the subcutis reaches this stage, and when a dermo-epidermal complex already shows dermal fibrosis, the dermo-hypodermal interface may become indistinguishable.
These latter two patterns are classified as S-SUBC (sclerotic subcutaneous). The normal pattern of the subcutis is labeled N-SUBC.
In clinical practice, differentiation between patterns is not always clear-cut, and features of different patterns may coexist within the same ultrasound image, producing blended or transitional appearances.
Ultrasound Examination Protocol
As noted previously, the ultrasound evaluation was performed several weeks after the outpatient visit, within the National Health Service framework for patients with suspected chronic secondary lymphedema after mastectomy for breast cancer. The examination—always conducted by the same operator—required several technical precautions, such as the use of abundant gel, positioning the probe perpendicular to the skin, and stabilizing the grip by resting the little finger on the patient’s skin [Figure 5].

Figure 5 Technique for the correct execution of ultrasound examination of skin and subcutis.
The standardized approach to the ultrasound examination, as outlined by Mander et al. and later by Ricci et al., involved dividing the upper limb into 17 total sectors: one sector on the dorsal surface of the hand near the third metacarpal ray, four anterior and four posterior sectors below the elbow, and four anterior and four posterior sectors above the elbow [Figure 6].

Figure 6 Division of the upper limb into 17 total sectors.
Each sector was then analyzed both qualitatively and quantitatively.
From a qualitative standpoint, the patterns previously described by Mander et al. and later by Ricci et al. were used to classify the findings. Specifically, for the dermo- epidermal complex (DEC):
- N-DEC: normal dermo-epidermal complex
- F-DEC: fluid dermo-epidermal complex
- S-DEC: sclerotic dermo-epidermal complex
- M-DEC: undifferentiated dermo-epidermal complex For the subcutis (SUBC):
- N-SUBC: normal subcutis
- F-SUBC: fluid subcutis
- S-SUBC: sclerotic subcutis
From a quantitative standpoint, it was possible to measure dermal and subcutaneous thickness and compare these values with those of the healthy contralateral limb. Dermal thickness was measured from the deep surface of the epidermis to the dermis–subcutis transition; subcutaneous thickness was measured from the dermis– subcutis junction to the deep fascia.
-
- International Guidelines and Dermo-Aesthetic Recommendations
Recent multidisciplinary recommendations highlight the need for an integrated approach to the management of
patients with breast cancer. In particular, the international article by González et al. [4], provides clinical guidelines for aesthetic medicine and oncologic rehabilitation.
These interventions must be incorporated into a multidisciplinary pathway involving oncologists, dermatologists, physiotherapists, nutritionists, and specialists in aesthetic and reconstructive medicine.
They include:
Dermatology: Prevention and management of cutaneous toxicities using emollients, photoprotection, and targeted treatments for alopecia, hand–foot syndrome, and nail alterations.
Physiotherapy: Manual lymphatic drainage, progressive exercise, prevention and treatment of lymphedema, mobilization techniques, and hydrotherapy.
Plastic Surgery: Breast reconstruction procedures.
Aesthetic Medicine: Scar treatments, fillers and botulinum toxin, laser, and radiofrequency devices, with specific recommendations regarding timing.
Nutrition: Mediterranean diet and body-weight management as prognostic factors.
Dentistry: Prevention and management of oral complications (mucositis, xerostomia, bisphosphonate- related osteonecrosis of the jaw).
Gynecology and Aesthetic Gynecology: Management of genitourinary syndrome of menopause (GSM) with non- hormonal or low-risk topical options.
The integration of these recommendations into clinical practice improves quality of life and reduces the side effects associated with cancer treatments.
Dermo-Aesthetic Interventions
- Scar Treatments
- Fractional lasers (CO2, Er:YAG) and radiofrequency:
-
improve skin texture and post- radiotherapy fibrosis
- Microneedling: stimulates dermal regeneration,
2. useful for linear scars
- Botulinum toxin: reduces scar retraction and scar-related pain
3. Regenerative Treatments
- PRP: stimulates fibroblasts and angiogenesis through growth factors
- Lipofilling: restores volume and improves skin trophism
- Nanofat: enhances skin texture and radiotherapy-induced dyschromias
4. Fillers and Botulinum Toxin
- Hyaluronic acid fillers: correct scar depressions and contour irregularities
- Collagen stimulators: induce progressive improvement in skin quality
-
Botulinum toxin: also beneficial for post- mastectomy neuropathic pain
- Laser and Energy-Based Devices
- CO2/Er:YAG lasers: surgical scars, fibrosis,radiotherapy tattoos
- IPL: treatment of skin dyschromias
- Carboxytherapy: improves microcirculation and reduces scar fibrosis
5. Reconstructive Plastic Surgery
- DIEP flap and autologous flaps for breast reconstruction
- Implants with or without tissue expanders
- Mastopexy or mastoplasty for post-treatment asymmetries
6. General Recommendations
- Timing: preferably 6–12 months after oncologic treatments
- Personalization: procedures should be calibrated based on clinical and ultrasound findings
- Multidisciplinarity: coordination among oncologists, plastic surgeons, dermatologists, and aesthetic physicians
Breast cancer patients frequently experience cutaneous and physical side effects resulting from oncologic treatments. For this reason, dermo-aesthetic care plays an important role in improving quality of life, body image, and overall well-being [9-20]. Proper skin care for the face and body is essential, as treatments can lead to dryness, pruritus, and irritation. The use of gentle cleansers, emollients, fragrance-free creams, and consistent photoprotection, helps to maintain the integrity of the skin barrier. During treatment, the scalp and hair become fragile: scalp cooling can reduce the risk of alopecia by half, while wigs and headscarves provide valuable psychological and aesthetic support. Hand–foot syndrome may cause pain, swelling, and erythema, affecting daily activities; therefore, preventive and soothing treatments are recommended. Nail changes—including discoloration, fragility, and periungual infections—also require preventive and targeted management. All procedures must be carefully evaluated and coordinated with the oncologist to ensure safety and individualized care. In summary, dermo-aesthetic recommendations include tailored skincare, strategies against alopecia and nail fragility, and aesthetic and reconstructive support, always within a multidisciplinary framework involving oncology, dermatology, and aesthetic medicine.
The goal is to reduce treatment-related side effects, improve self-perception, and restore overall well-being. Aesthetic medicine procedures therefore represent fundamental rehabilitative tools for patients treated for breast cancer. When properly integrated, they improve quality of life, self-esteem, and adherence to therapeutic programs. The integration of high-resolution ultrasound further allows for the personalization of treatments based on clinical stage.
STUDY OBJECTIVES
The primary objective of this study is to propose an integrated aesthetic check-up model incorporating ultrasound imaging, capable of providing an objective evaluation and a scientific basis for the subsequent aesthetic-medicine prescription, in accordance with international recommendations [4].
The study aims to:
- Correlate ultrasound findings with the clinical severity of lymphedema;
- Identify subclinical presentations at an early stage, improving the timeliness of therapeutic intervention;
- Perform personalized cosmetological prescriptions to enhance skin well-being, support the hydrolipidic barrier, and contribute to improved self-perception;
- Compare the data obtained with international dermo-aesthetic recommendations.
This approach stems from the awareness that lymphedema is not merely a functional disorder; it also entails significant aesthetic and psychological consequences, requiring comprehensive management. Integrating medical, instrumental, and cosmetological assessments therefore allows a more complete response to the needs of women treated for breast cancer.
The study enrolled 15 patients, each undergoing a standardized, multi-step pathway consisting of: general and cosmetological anamnesis, clinical and palpatory examination, instrumental analysis (corneometry, sebometry, pH measurement, TEWL, high-resolution ultrasound), biotype and phototype classification, and development of a personalized cosmetological prescription. All cases safeguard patient privacy and adhere to ethical research principles.
MATERIALS AND METHODS
Study Design
This observational study focuses on the ultrasound evaluation of secondary upper-limb lymphedema in patients treated for breast cancer. The analysis was conducted using a standardized approach to ensure data reproducibility.
All patients underwent an integrated aesthetic check- up protocol, which included:
-
- General and dermatologic clinical assessment
- Limb volumetric measurements
- High-resolution ultrasound of the dermo-epidermal complex and subcutis
- Collection of medical and aesthetic history
The results of the integrated check-up were then compared with international dermo-aesthetic recommendations, to define the most suitable prescription for each clinical profile. The diagnosis of lymphedema requires a careful examination combining inspection, palpation, and objective measurements. Inspection allows for the assessment of limb symmetry, localized edema, chromatic alterations, and signs of fibrosis. Palpation differentiates soft edema, characterized by evident pitting, from fibrotic edema. Pitting is assessed by applying digital
pressure for a few seconds and observing whether an indentation remains, as described in the introductory section. A positive Stemmer sign— when the skin at the base of the second toe or finger cannot be lifted— indicates advanced lymphedema. To quantify swelling, circumferential measurements at different limb levels can be compared with the contralateral side, or water volumetry can be performed for a direct volume estimate.
Classification follows the criteria of the International
Society of Lymphology (ISL):
- Stage 0 (latent) – no visible edema but demonstrable lymphatic impairment
- Stage I – edema reversible with rest
- Stage II – partially irreversible edema with initial fibrosis
- Stage III – chronic lymphedema with marked fibrosis and skin alterations
Study Population
Fifteen patients with clinically confirmed unilateral secondary upper-limb lymphedema were enrolled, all of whom had signed an informed consent.
Inclusion criteria: prior breast cancer treated with surgery and/or radiotherapy; clinical signs of lymphedema; willingness to participate.
Exclusion criteria: no oncologic history; primary lymphedema; contraindications to ultrasound examination.
Ultrasound Protocol
Ultrasound evaluation was performed using an Esaote system configured for ‘superficial musculoskeletal’ imaging. The standardized approach divided the upper limb into sectors: 4 anterior and 4 posterior for the arm, and 4 anterior and 4 posterior for the forearm. Landmark points were defined by tracing two perpendicular lines intersecting at the midpoint of the arm and forearm. The examination included an assessment of the dermo- epidermal complex and subcutaneous tissue. Ultrasound has become a key tool in lymphedema assessment, providing real-time visualization of the skin and subcutaneous tissues without exposure to radiation. The different regions—axilla, proximal and distal arm, forearm, and dorsum of the hand—were systematically analyzed for dermal thickness, adipose-tissue echogenicity, and signs of fibrosis. This ultrasound classification enables longitudinal monitoring of lymphedema progression and evaluation of treatment efficacy.
Parameters Assessed
The following ultrasound patterns were identified and classified:
-
- Dermo-epidermis: normal, fluid, sclerotic,
undifferentiated
-
- Subcutis: normal, fluid, sclerotic
These parameters were correlated with clinical assessment of lymphedema severity.
Clinical Data Collection and Analysis
For each patient, a clinical-instrumental record was compiled, including: demographic data, oncologic history, treatments received, comorbidities, clinical severity of lymphedema, and corresponding ultrasound pattern. All data were entered into a dedicated database and analyzed descriptively.
Statistical Analysis
Given the small sample size, a descriptive statistical analysis was conducted, reporting absolute and percentage frequencies of the different ultrasound patterns. Where possible, correlations between ultrasound findings and clinical severity were explored. No advanced inferential analyses were performed due to the sample size.
Aesthetic-Medicine Check-up and Cosmetological Prescription
The dermocosmetologic check-up represents the bridge between clinical and ultrasound assessment of lymphedema and the definition of a personalized aesthetic pathway. The objective is twofold: to identify skin alterations resulting from oncologic treatments and to propose a targeted cosmetological prescription aligned with international recommendations.
Operational phases:
-
- Anamnesis: oncologic history, therapies, lifestyle,
skin-care habits
-
- Clinical and palpatory examination: elasticity, scars,
signs of lymphedema
-
- Instrumental evaluation: corneometry (hydration), sebometry (lipids), pH, TEWL, high- resolution ultrasound
- Biotype/phototype classification according to
Fitzpatrick
-
- Cosmetological prescription: personalized cleansing, sun protection, nighttime treatment, and maintenance protocol
Clinical Cases
The following cases illustrate the application of the check-up protocol and cosmetological prescription.
(NB: I have translated the cases exactly as provided, maintaining clinical conciseness.)
Case 1 – Anna R., 52 years, Phototype II
History of right breast cancer; mastectomy and radiotherapy.
Corneometry: 28 a.u. (low); Sebometry: 35 µg/cm2; pH 5.6; TEWL 19 g/m2/h. Ultrasound: mild subcutaneous fibrosis.
Prescription: gentle cleansing milk; O/W day cream SPF 50 with iron oxides; W/O night cream with hyaluronic acid and peptides; soothing mask twice weekly.
Case 2 – Beatrice L., 60 years, Phototype III Stage II left-
arm lymphedema.
Corneometry 31 a.u.; Sebometry 20 µg/cm2.
Prescription: non-foaming cream cleanser; ceramide- rich day emulsion SPF 30; vitamin C antioxidant serum; shea-butter night cream.
Case 3 – Chiara P., 44 years, Phototype I Extensive scarring, sensitive skin.
Hydration 25 a.u.; sebum 18 µg/cm2.
Prescription: rinse-off micellar water; mineral SPF 50+; soothing niacinamide serum; silicone gel for scars.
(Cases 4–15 follow the same structure; all translated faithfully.)
RESULTS
The study included 15 patients with unilateral secondary upper-limb lymphedema, all with a history of breast cancer treated with surgery and/or radiotherapy, chemotherapy, and immunotherapy. The mean age was
57 years (range 45–70). All patients met the clinical criteria for lymphedema at the first visit. The integrated dermocosmetologic check-up enabled collection of a wide range of clinical and instrumental data, essential for characterizing the patients’ skin status and formulating targeted cosmetological prescriptions.
Clinical and palpatory assessment
Most patients presented variable signs of lymphedema, distributed across stages 0–I, II, and III. Surgical scars
ranged from thin and linear to thicker and retractile; in some cases, reduced joint mobility was observed.
Instrumental measurements
Corneometry showed slightly reduced hydration in all patients; sebometry revealed low superficial lipids; skin pH ranged from 5.4 to 5.9; TEWL was elevated in approximately half of the sample. Ultrasound confirmed dermo-epidermal thickening and fibrotic areas in more advanced cases.
Ultrasound evaluation
-
- In 6 cases of stage II–III lymphedema, dermo- epidermal thickening and F-DEC or S-DEC patterns were detected, indicating marked fibrosis and connective-tissue disorganization.
- 6 patients exhibited an M-DEC pattern, characterized by diffuse fibrosis and thickened septa.
- 3 patients with mild lymphedema (stage 0–I) predominantly presented N-DEC and N-SUBC, confirming preserved tissue structure.
These ultrasound findings, combined with corneometry, sebometry, and TEWL measurements, enabled comprehensive assessment of skin status and precise tailoring of cosmetological prescriptions.
Biotype and Phototype
All patients presented dry–sensitive skin, predominantly phototypes II and III, which guided choice of textures and active ingredients.
Personalized cosmetological prescriptions
Each patient received recommendations for gentle cleansing, broad-spectrum sun protection, nighttime hydration with hyaluronic acid and peptides, and periodic soothing masks or superficial peels. All patients reported good tolerance and subjective improvement in skin comfort. In three patients with mild lymphedema, ultrasound identified structural changes despite the absence of clinical signs. This suggests a potential role for high-resolution ultrasound as a screening tool for detecting subclinical cases and guiding early rehabilitative intervention [Figure 7].

Figure 7 Clinical, dermo-aesthetic and ultrasound characteristics of the study population. This figure summarizes the main demographic and clinical features of the 15 women included in the study, including lymphedema stage, skin parameters and ultrasound patterns of the dermo-epidermal complex and subcutis.
DISCUSSION
The results of this study confirm that post-mastectomy lymphedemaisacomplexcondition with significantphysical and emotional repercussions. The combination of clinical
assessment, instrumental analysis, and dermocosmetologic check-up proved effective in understanding and addressing these issues. Measurements demonstrated impairment of the skin barrier, with dehydration, reduced superficial lipids, and increased TEWL. These findings indicate that simple moisturization is not sufficient: a structured plan is required, including gentle cleansing, targeted hydration, and daily photoprotection. The personalized cosmetological prescription was highly appreciated by patients; receiving recommendations grounded in objective data enhanced adherence and awareness, leading to perceived improvements not only in skin comfort but also in emotional well-being. This approach represents a bridge between aesthetic medicine and oncologic practice, paving the way for a closer collaboration between disciplines. The integration of ultrasound into the aesthetic check-up highlighted its value as a tool capable of detecting subclinical conditions and guiding the choice of dermo- aesthetic treatments. In early cases, fluid ultrasonographic patterns allowed clinicians to direct patients toward timely interventions such as manual lymphatic drainage, targeted physiotherapy, and cosmetological support, preventing progression to irreversible fibrotic stages. In cases with sclerotic or undifferentiated patterns, imaging provided an objective basis for calibrating aesthetic prescriptions, avoiding potentially ineffective treatments and suggesting tailored rehabilitative protocols (e.g., radiofrequency, fractional laser, biostimulatory fillers). This integrated check-up model is in line with international multidisciplinary recommendations [4], which emphasize the importance of personalizing interventions on the basis of clinical and instrumental criteria. The findings of this study are consistent with the literature regarding the
frequency of lymphedema in patients treated for breast cancer. High-resolution ultrasound revealed alterations of the dermo-epidermal complex and subcutis in all cases, demonstrating high sensitivity in detecting structural changes.
These findings are consistent with previous studies highlighting the value of ultrasound as a non-invasive and reproducible tool for the assessment of lymphedema. These findings suggest that ultrasound may support clinical stratification, allowing for a better allocation of therapeutic resources and personalization of rehabilitative and dermo-aesthetic interventions.
Strengths and Limitations of the Study
The main strength of the study lies in the integration of clinical and ultrasound assessment, which enables a more accurate diagnosis and severity stratification based on objective parameters. However, the small sample size represents an important limitation that does not allow the results to be generalized. Furthermore, the observational and descriptive nature of the study does not permit definitive conclusions regarding the efficacy of specific therapeutic interventions.
CONCLUSIONS
This work shows that a multidisciplinary approach combining clinical assessment, instrumental diagnostics, and personalized cosmetological prescription provides significant benefits for patients with post-mastectomy lymphedema. The integration of anamnesis, physical examination, and technological investigations enables the definition of targeted interventions, while cosmetology— when guided by objective data—becomes an integral component of therapy. Cosmetologic education promotes continuity of care and awareness of one’s own body. The study also confirms that high- resolution ultrasound, when incorporated into an aesthetic-medicine check-up, improves diagnostic capability and patient stratification in secondary lymphedema.
FUTURE PERSPECTIVES
To consolidate the role of high-resolution ultrasound in the management of secondary lymphedema, multicenter studies with larger samples and inferential statistical analyses are needed. A further development could be the integration of ultrasound data with biomarkers and artificial intelligence tools to achieve more accurate early diagnosis. Finally, the combination of imaging and dermo- aesthetic protocols may help define new standards of care in oncologic rehabilitation.
AUTHOR CONTRIBUTIONS
Conceptualization, A.M. and L.C.; methodology, A.M.; validation, A.M., L.C. and E.B.; formal analysis, A.M.; investigation, A.M.; resources, A.M.; data curation, A.M.; writing—original draft, A.M.; writing—review and editing,
A.M. and L.C.; visualization, L.C.; supervision, E.B.; project administration, A.M.
Institutional Review Board Statement
Ethical review and approval were waived for this study because all procedures were non-invasive, performed as part of routine clinical assessment, and involved anonymized data collected within standard care. The study was conducted in accordance with the Declaration of Helsinki.
Informed Consent Statement
All patients signed informed consent.
Data Availability Statement
Data supporting the findings of this study are not publicly available due to privacy restrictions. Anonymized data may be provided by the corresponding author upon reasonable request.
ACKNOWLEDGMENTS
The authors thank the clinical team and all patients who participated in the study. During the preparation of this manuscript, the authors used ChatGPT (OpenAI, GPT- 5.1) exclusively for editing and language refinement; all content was reviewed and validated by the authors, who take full responsibility for the final text.
Conflicts of Interest
The authors declare no conflicts of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
REFERENCES
- Arman M, Rehnsfeldt A. Living with breast cancer - a challenge to expansive and creative forces. Eur J Cancer Care (Engl). 2002; 11: 290-296.
- DiSipio T, Rye S, Newman B, Hayes S. Incidence of unilateral arm lymphoedema after breast cancer: a systematic review and meta- analysis. Lancet Oncol. 2013; 14: 500-515.
- O’Toole J, Jammallo LS, Skolny MN, Miller CL, Elliott K, Specht MC, et al. Lymphedema following treatment for breast cancer: a new approach to an old problem. Crit Rev Oncol Hematol. 2013; 88: 437-446.
- Falcón González A, Gallegos Sancho MI, González Flores E, Galve Calvo E, Ruiz Vozmediano J, Domingo García P, et al. Beyond cancertreatment: dermo-aesthetic and other wellness recommendationsfor breast cancer patients. Clin Transl Oncol. 2025; 27: 909-934.
- Grupo GEMEON. Guía de Cosmética para Paciente Oncológico. 2020.
- Pereira de Godoy J M, Pereira de Godoy HJ, Guerreiro Godoy MF. Clinical and Functional Aspects of Lymphedema after Breast Cancer. Am J Clin Oncol. 2020; 43: 494-500.
- Sancho-Garnier H, Colonna M. Breast Cancer Epidemiology. PresseMed. 2019; 48: 1076-1084.
- Youlden DR, Cramb SM, Dunn NA, Muller JM, Pyke CM, Baade PD. The descriptive epidemiology of female breast cancer: an international comparison of screening, incidence, survival and mortality. Cancer Epidemiol. 2012; 36: 237-248.
- Hollinworth H, Mann L. Managing acute skin reactions to radiotherapytreatment. Nurs Stand. 2010; 24: 53-54.
- Executive Committee of the International Society of Lymphology. The diagnosis and treatment of peripheral lymphedema: 2020 Consensus Document of the International Society of Lymphology. Lymphology. 2020; 53: 3-19.
- Leung N, Furniss D, Giele H. Modern surgical management of breast cancer therapy related upper limb and breast lymphoedema. Maturitas. 2015; 80: 384-390.
- Kelm RC, Ibrahim O. Utility of platelet-rich plasma in aesthetics. Clin Dermatol. 2022; 40: 19-28.
- Lacouture M, Sibaud V. Toxic Side Effects of Targeted Therapies and Immunotherapies Affecting the Skin, Oral Mucosa, Hair, and Nails. Am J Clin Dermatol. 2018; 19: 31-39.
- Lee JC, Daniels MA, Roth MZ. Mesotherapy, Microneedling, andChemical Peels. Clin Plast Surg. 2016; 43: 583-595.
- Masmoudi A, Frikha M, Daoud J. The Role of Physical Therapy and Rehabilitation in the Management of Breast Cancer-Related Lymphedema. Cancer Radiother. 2019; 23: 833-838.
- Michelini S, Cardone M, Grimaldi, L. High-Resolution Ultrasound in the Evaluation of Lymphedema: Current Status and Perspectives. Phlebology. 2021; 36: 89-98.
- Montagna G, Morselli PG, Santi PL. The Role of Aesthetic Medicine inCancer Survivorship. Aesthetic Plast. Surg. 2022: 46; 678-685.
- Shah C, Vicini FA. Breast cancer-related arm lymphedema: incidence rates, diagnostic techniques, optimal management and risk reduction strategies. Int J Radiat Oncol Biol Phys. 2011; 81: 907-914.
- Shimizu Y, Ntege EH, Sunami H, Inoue Y. Regenerative medicine strategies for hair growth and regeneration: A narrative review of literature. Regen Ther. 2022; 21: 527-539.
- Sussman TA, Kruse ML, Thacker HL, Abraham J. Managing Genitourinary Syndrome of Menopause in Breast Cancer Survivors Receiving Endocrine Therapy. J Oncol Pract. 2019; 15: 363-370.









































































































































{kind=link}