Conservative Retrieval of Fractured Abutment Screw
- 1. Department of Periodontics, Krishnadevaraya College of Dental Science, India
Abstract
Failure of implant components can occur due to biological or mechanical factors. Biological factors comprise ineffective osseointegration and occurrence of periimplantitis. Mechanical failures include crown breakage, framework fracture, screw loosening, and screw fracture. Dental implants can be rendered ineffective due to such complications related to implant components. One of the most serious mechanical consequences of implant treatment is screw loosening and fracture, which is now becoming increasingly common. Removal of fractured fragments is deemed necessary for the sake of prosthetic restoration. Various techniques have been defined for the removal of the fractured segment from the screw hole. This case report presents a rare incident of implant abutment screw fracture and the utility of a piezoelectric ultrasonic scaler in conservatively retrieving the fractured abutment screw fragment.
Keywords
• Dental implants
• Abutment screw fracture
• Retrieval methods
Citation
Rajan R, Shamsuddeen S, Prabhuji MLV (2021) Conservative Retrieval of Fractured Abutment Screw – A Case Report. JSM Dent Surg 4(1): 1033.
INTRODUCTION
Dental implants have become widely recognized and highly effective for the treatment of missing teeth. Osseointegration is an important biological parameter for the success of implant. While the overall success rate of osseointegrated dental implants is very high, dental implants seldom fail [1]. Various complications may arise during implant treatment. Esthetic, phonetic, functional, biological, mechanical, and ergonomic are the six major categories of latent complications [2]. Mechanical complications comprise of problems of retention, framework fractures, crown fractures, screw loosening, and screw fracture. In implant dentistry two types of screws are used: Abutment and prosthetic screws are made from a range of materials, including gold, commercially pure titanium, and surface-treated or coated titanium alloys. One of the most frequent mechanical complications is abutment screw loosening followed by the screw fracture with most common causes being ill-fitting superstructure, bruxism or overloading. A five?year period study has revealed that the incidence of fracture of abutment screw is 3.9% and loosening of abutment screw is 6.7% [3].
Abutment screw fracture can be unusual but a distressing complication of implant prosthetic treatment. The principal reason for screw fracture is unobserved screw loosening, inadequate tightening, excessive occlusal forces, overloading, fatigue, malocclusion, repeated loosening and retightening of screw, non-passive fit of superstructure and Para functional habits [4]. Retrieval of fractured screw fragments is defined by a simplified technique. This comprises screw fragment to be retrieved without damaging or varying the surface characteristics of the component as well as avoiding damage to the implant’s internal threads [5]. According to the location of the fractured abutment screw, different methods are used to hold the broken fragments or screw.
Different methods of abutment screw retrieval are discussed below
Explorer or probe: When the screw fracture happens at or below the head of implant, retrieval can be accomplished by releasing the screw fragment and locking it in a counterclockwise direction.
Ultrasonic scaler: Placing the thin tip of an ultrasonic scaler directly on the top of the abutment screw can gradually reverse out the screw from ultrasonic scaler oscillation. To decrease friction and ease of holding, lubricant such as eugenol or mineral oil can be used to support in screw retrieval.
Forceps, hemostat: When the screw fracture happens above the head of implant, artery forceps/hemostats can be used to hold the broken piece.
High- and low-speed handpiece: 1 mm slot is prepared across the most occlusal portion of the fragmented screw using high-speed handpiece fitted with a diamond bur.
A low-speed contra-angle handpiece with a 1/4 round carbide bur in reverse mode aids in screw removal. It holds the head of the fragment and mainly acts as a screwdriver.
Screw retrieval kit
If the abutment fracture is deep and cannot be removed with existing treatments, a screw retrieval kit is another option for removing the abutment screw.
- ITI® Dental Implant System (Institut Straumann AG, Switzerland), comprises of drills, two drill guides and six manual tapping instruments
- IMZ® Twin Plus Implant System1 (Dentsply Friadent, Germany)
- Screw Removal Kit Replace (Nobel Biocare™, Yorba Linda, California, USA)
- Certain®-Screw Removal Kit (Biomet 3i™, Florida, USA) [1].
The steps involved in implant screw retrieval kit are:
- Appropriate drill guide is inserted onto the implant platform.
- Reverse pushing motion is made using contra-angle hand piece with the pilot drill at 1,000-1,250 RPM and copious irrigation to create a 1-2 mm deep into the fractured screw head. For the next drill, created purchase point should be tapped.
- Metal shavings are then suctioned and the area is irrigated.
- Finally, the broken screw is retrieved out of the screw chamber using the tap drill at 70-80 rpm.
Accessory Instruments
If the implant is buried under the soft tissue, a minor soft tissue procedure can be done to expose the implant. In these circumstances, soft tissue laser can be used in circular fashion for removal of the tissue. Electrosurgery is another procedure employed in such cases [6].
The aim of this case report is to present an alternative simple method for retrieval of fractured implant abutment screw and new abutment was placed to permit the patient to wear the existing prosthesis.
CASE PRESENTATION
A 56 year old female patient presented to the Department of Periodontics, Krishnadevaraya Dental College, Bengaluru with a chief complaint of dislodged healing abutment with respect to an implant placed in the mandibular right first molar since 1 month. The patient stated that implant was placed 1 year back and was restored using cement retained metal ceramic crown. Intraoral examination revealed that the implant head was enclosed by the soft tissue. There was presence of suppuration (Figure 1).
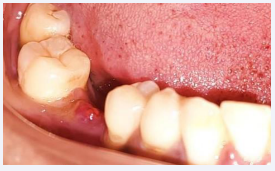
Figure 1: Implant head covered by soft tissue.
Further radiographic assessment confirmed the presence of the fractured abutment screw threaded into the implant with no indication of any damage to implant body and evidence of marginal bone loss (Figure 2).
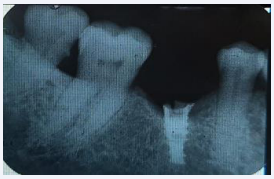
Figure 2: Radiograph showing fractured fragment within the implant body.
To retrieve the broken fragment the following steps were undertaken
1. After anesthetizing the area, horizontal incision was given on most fluctuant area and pus was drained by using curette.
2. Implant exposure was done using the diode laser (810 nm wavelength), which was inserted at the center of the site and worked in a spiral pattern outward until the entire cover screw was exposed. Then curette was used to release the tissue over the cover screw (Figure 3).

Figure 3: Implant exposed using diode laser.
3. After locating the site of the screw fracture, the implant body was meticulously cleaned using an air/water spray from the 3-way syringe and dried with air.
4. The piezoelectric ultrasonic scaler tip (EMS-Tip P) was placed on upper surface of the fractured abutment screw.
5. The scaler tip was held firm on the upper surface of the fractured fragment and the oscillations were started with minimal power and copious irrigation.
6. When the vibrating scaler tip contacted the surface of the screw, a moderate reverse torque was applied alternatingly and fractured abutment fragment spun out of the implant body (Figure 4).
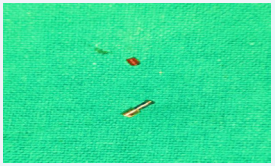
Figure 4: Fractured abutment screw.
7. As the fractured abutment screw fragment started loosening, the tip contacting the screw fragment was gradually decreased. The loosened abutment screw was then removed with a tweezer.
Using the air/water spray the internal surface of the implant was again cleaned.
9. The new abutment was then tried for the fit and preservation which helps to confirm the absence of damage of internal retentive structure of the implant.
10. New abutment was tightened to the implant body with a screw, existing prosthesis was cemented (Figure 5) and radiograph was taken (Figure 6).

Figure 5: New abutment tightened to the implant body with a screw and cemented with prosthesis.
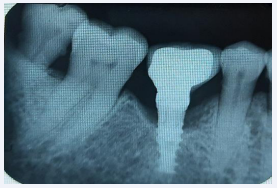
Figure 6: Radiograph after prosthesis placement.

Figure 7: 1 month follow up.
11. The patient was instructed on the use of 0.12% chlorhexidine mouthwash, systemic antibiotics (amoxicillin 500 mg thrice daily for 3 days and metronidazole 400 mg twice daily for 3 days) and
was seen intermittently for professional oral hygiene maintenance during the follow-up period.
DISCUSSION
A common complication of implant prosthetics is with components. The abutment screw connects the abutment to the fixture and can fracture under occlusal functional load. Fracture of an abutment screw is a challenging complication of implant-supported restorations. The fractured abutment screw has to be removed without hostile to the internal threads of the implant body to allow efficient functioning of the implant. The present situation demonstrates a complication in-built in the use of implant components. The abutment screw fracture due to occlusal overload is detected in this case as one of the most common complications. Repeated screw loosening and tightening may lead to fracture of abutment screws, imposing unwanted suffering to the patient [7]. As an innovative approach to treat this situation, ultrasonic was used and it resulted in a considerable reduction in bone loss. The tissue surrounding the implant was found to be healthy.
According to Misch, fractures of screw can be prevented by [8]:
• Confirming adequate fit of the prosthesis
• Avoiding excessive angulation of implants to occlusal load
• Using the correct fixation screw
• Avoiding occlusal overload of the prosthesis
• Screw tightening torque with a torque wrench applied heavily
• Reinforcing periodic maintenance
It is important to apply a gentle reverse torque simultaneous with ultrasonic vibrations , that will prevent the screw from twisting further into the implant and allow for its easy salvage. The procedure implemented in this case also has the advantage being painless and time saving and having a familiar armamentarium as well as completely abolishes the need for drilling on the top surface of the broken fragment to create a slot.
Bhandari et al., [9] used piezoelectric scaler on low, combined with reverse torque and concluded that screw being in an inclined plane, will unthread when subjected to continuous vibrations.
In a study, Joshi et al., [10] used fine round bur no. BR 49 to make groove on the occlusal surface of fractured screw across the diameter. Finally, ultrasonic scaler tip engaged and actuated
in the groove. The unconventional technique described in the current article developed simple armamentarium that is costeffective and can be universally used for any implant system.
CONCLUSION
Abutment screw fracture is a documented complication of implant placement. Adequate treatment planning, alertness of the occlusal scheme, tightening to the correct torque, and regular recall appointments will reduce the incidence of abutment screw loosening and fracture. The technique described in this article comprises the management of an implant abutment screw fracture using an unconventional technique and simple armamentarium. The piezoelectric ultrasonic scaler, which is a part of the routine dental armamentarium, is surely feasible for conservative retrieval of a fractured screw fragment, and the procedure’s non-invasive nature would also be satisfying to the patient.
REFERENCES
1. Reyhanian A, Parker S, Moshonov J, Fuhrman N. The use of Er: YAG in laser-assisted broken abutment screw treatment. case report _Er:YAG. 2010; 3: 6-11.
2. Balshi TJ. Preventing and resolving complications with osseointegrated implants. Dent Clin North Am. 1989; 33: 821-868.
3. Goodacre CJ, Bernal G, Rungcharassaeng K, Kan JY. Clinical complications with implants and implant prostheses. J Prosthet Dent. 2003; 90: 121-132.
4. Gooty JR, Palakuru SK, Guntakalla VR, Nera M. Noninvasive method for retrieval of broken dental implant abutment screw. Contemp Clin Dent. 2014; 5: 264-267.
5. Imam AY, Moshaverinia A, Chee WW, McGlumphy EA. A technique for retrieving fractured implant screws. J Prosthet Dent. 2014; 111: 81-83.
6. Mizumoto RM, Jamjoom FZ, Yilmaz B. A risk-based decision-making tree for managing fractured abutment and prosthetic screws: A systematic review. J Prosthet Dent. 2018; 119: 552-559.
7. Schwarz MS. Mechanical complications of dental implants. Clin Oral Implants Res. 2000; 11: 156-158.
8. Williamson RT, Robinson FG. Retrieval technique for fractured implant screws. J Prosthet Dent. 2001; 86: 549-550.
9. Satwalekar P, Chander KS, Reddy BA, Sandeep N, Sandeep N, Satwalekar T. A simple and cost effective method used for removal of a fractured implant abutment screw: a case report. J Int Oral Health. 2013; 5: 120-123.
10. Joshi A, Kale VT, Suragimath G, Zope SA. An unconventional approach for retrieval of fractured prosthetic screw: A case report. J. Osseointegration. 2018; 10: 75-78.








































































































































