Retrieval of Foreign Bodies by Surgical Approach: A Case Report
- 1. Aishwarya Roy, Department of Conservative Dentistry & Endodontics, Bareilly International University, India
- 2. Rashmi Bansal, Department of Conservative Dentistry & Endodontics, Bareilly International University, India
- 3. Saummya Singh, Department of Conservative Dentistry & Endodontics, Bareilly International University, India
Abstract
Fracture of endodontic instrument is an unfortunate mishap which may obstruct thorough cleaning and shaping of the root canals with potential impact on the endodontic prognosis and treatment outcome. When the fractured segment lies apical to canal curvature, overzealous removal of tooth structure is required to gain access to the separated segment which in turn increases the likelihood of root fracture. In infected cases, the stage at which instrument separation occurs is crucial as root canal disinfection is jeopardized. This case report describes the surgical retrieval of a fractured endodontic file and separated obturating material beyond the root apex.
Keywords
• Fractured instrument
• Silver point
• Mineral trioxide aggregate
• Platelet rich fibrin
• Periapical surgery
Citation
Aishwarya R, Rashmi B, Saummya S (2021) Retrieval of Foreign Bodies by Surgical Approach: A Case Report. JSM Dent Surg 4(1): 1032.
ABBREVIATIONS
MTA: Mineral Trioxide Aggregate, PRF: Platelet Rich Fibrin, NiTi: Nickel Titanium, H file: Hedstrom file
INTRODUCTION
The fracture of endodontic instruments is a procedural problem creating a major obstacle to normal routine therapy. The separation of instruments during endodontic therapy is a troublesome incident, and its incidence ranges from 2% - 6% of the cases investigated [1, 2]. Separated fragments may range from file, reamer, Gates-Glidden, Peeso drills, lentulospiral paste fillers, thermo mechanical gutta-percha compactors, the tips of hand instrument like explorers, gutta-percha, spreaders, gutta percha, silver point etc. which may block access to apical terminus [2]. Separation may occur due to improper usage of hand and rotary instruments, manufacturing defects, frailty in physical properties of endodontic instruments, inadequate access to root canal and unusual anatomy of root canal [3]. This separated fragment hinders the access and biomechanical preparation of root canal and affects the outcome of the endodontic therapy [4]. Therefore, it is necessary to bypass or retrieve the instrument before leaving it and obturating to the level of separation or undertake surgical procedure. If the fractured segment lies apical to canal curvature, overzealous removal of tooth structure is required to gain access to the separated segment which in turn increases the likelihood of root fracture. The present case report describes the successful retrieval of separated fragments by surgical approach as the separated fragments lies beyond canal apex. Mineral Trioxide Aggregate (MTA) apical plug and second generation platelet concentrate called Platelet Rich Fibrin (PRF) was placed to fill the surgical defect as the combination enhances the regenerative effect by exerting an osteoconductive effect in the bony defect area. The clinical and radiographic examination after six months revealed satisfactory periapical healing.
CASE PRESENTATION
A 38-year-old male patient with a chief complaint of pus discharge and dull aching pain in relation to his maxillary anterior tooth (# 21) was referred to Department of Endodontics. Brief history revealed that the patient had trauma in maxillary anterior region and had undergone root canal treatment 8 years back followed by retreatment 5 years back in same tooth but symptoms persisted again from last 1 month. Clinical examination revealed Ellis Class III fracture in relation to 21 and symptomatic with tender on percussion in relation to 21 & 22. Intraoral radiograph showed fractured instrument and separated obturating material extruding beyond the peri-apex with evident large periapical radiolucency involving 21 & 22, suggesting presence of periapical abscess. The treatment was planned was retreival of old obturating material followed by endodontic treatment by creating MTA apical plug in relation to 21 & 22 and surgical removal of periapically extruded fractured instrument and separated obturating material.[Figure 1A & B].

Figure 1: A) Pre-operative clinical photograph, B) Pre-operative radiographic image.
Orthograde retreatment of 21 was commenced with an attempt to retrieve the obturating material from the canal. After coronal flaring, NiTi (Nickel Titanium) Hedstrom File (H file) instruments (DENTSPLY Tulsa Dental Specialties) were used to retrieve the obturating material from the canal. With the use of Hedstrom File (H file) the obturating material was successfully retrieved from the canal. Access opening was performed for 22 and working length was determined using electronic apex locator (Coltene, Dentsply, USA) and confirmed using radiograph in relation to 21 & 22. [Figure-2 A & B]Canal was prepared using NiTi K file upto #70 in relation to 21 and upto #55 in relation to 22.

Figure 2: A: Radiograph showing retrieval of obturating material i.e. silver point, B: Working length determination.
Normal saline and metrogyl (Novo dental products pvt., ltd, India) was used to irrigate the canals during canal preparation. After canal preparation, calcium hydroxide based intracanal medicament (RC Cal, Prime dental products pvt ltd, India) was placed and temporized with Cavit (3M ESPE Dental, India) for one week. However, on follow up after one week, the tooth was still symptomatic but pus discharge was not present. Canal was irrigated and calcium hydroxide based intracanal medicament was repeated. Patient was recalled again after one week. After a week, when the acute msymptoms had resolved, canals were irrigated with final rinse of 17% EDTA (Canalarge, Ammdent, Chandigarh, India) and normal saline. After copious saline irrigation, the canals were dried with paper points. MTA apical plug was made and cavit was placed. [Figure-3].
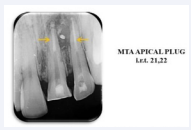
Figure 3: Radiograph showing orthograde MTA apical plug.
Following MTA apical plug, Dentascan was performed to evaluate the location of fractured instrument and separated silver point and to determine the extent of lesion and bone defect. [Figure 4 A, B, C, D, E & F].
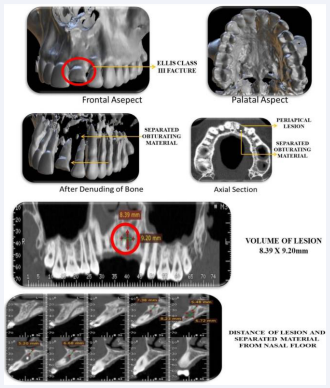
Figure 4: A-F: Detailed images of Dentascan showing presence of separated instrument and obturating material and extent of lesion.
After detailed study of Dentascan report, blood investigation was carried and periapical surgery was initiated. Complete intraoral disinfection was done with betadine rinse before surgery. After administration of local anaesthesia (1:80000 adrenaline, Lignocaine, Warren pharmaceuticals pvt., ltd, India), crevicular incision was given extending from distal aspect of lateral incisor to mesial aspect of canine with subsequent vertical releasing incisions. [Figure-5A].
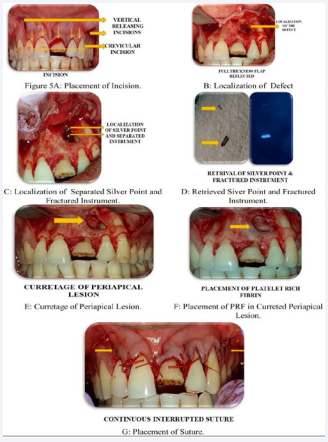
Figure 5: A: Placement of Incision, B: Localization of defect, C: Localization of separated silver point and fractured instrument, D: Retrieved siver point and fractured instrument , E: Curretage of periapical lesion, F: Placement of PRF in currated periapical lesion, G: Placement of Suture.
A full thickness mucoperiosteal flap was reflected on the buccal aspect and defect was localized. A buccal window of approximately 4 mm diameter was created by osteotomy to locate the root end. Apex of root along with the extruded instrument and silver point could be well visualised [Figure- 5B & C]. A deep cut was made using a round bur with copious irrigation using sterile saline, parallel to the long axis, nearly located in the centre of the root through the mesial aspect. The fractured file and separated silver point was retrieved and all pathological tissue was thoroughly debrided with curettage [Figure-5D & E]. The osseous defect was filled with PRF produced by Choukron’s technique and a synthetic nano crystalline hydroxyapatite. [Figure-5F] Mucoperiosteal flap was approximated with continuous interrupted sutures. [Figure-5G] An immediate postoperative radiograph was taken to confirm complete retrieval of the fractured segments. [Figure-6] antibiotics (Amoxycillin and clavulanate potassium 625 mg) and Non-Steroidal Analgesics (Diclofenac) were prescribed along with 0.2% chlorohexidine digluconate mouthwash for five days postsurgery.

Figure 6: Post-operative radiograph showing complete retrieval.
On recall after surgery days, patient was asymptomatic and sutures were removed. Postoperatively, clinical and MTA, has many unique characteristics that are consistent with an ideal material for various endodontic applications, including its use as root-end filling during apical surgery [8].MTA has been considered in this case as it is effective as an apical barrier and its application results in predictable apical closing, periapical healing and hard tissue formation at apex [9].
PRF, a second generation platelet rich concentrate, has diversified applications in dentistry such as extraction socket radiographic examinations were done in three months interval for a period of six months. The radiograph and clinical picture demonstrated satisfactory healing of the periapical radiolucency with no clinical signs or symptoms. [Figure-7 A & B]

Figure 7: A: Clinical Photograph showing no sinus and proper gingival adaptation, B: Radiograph reveals satisfactory periapical healing.
DISCUSSION
Instrument fracture obstructs optimal cleaning and shaping of the root canals thereby compromising the final outcome because of pulp remnants and bacteria persisting in the canals. In this case report, RVG and Dentascan was used for precise location of the fractured segments similar to the case report of Gandevivala A et al., for retrieval using a surgical approach [5]. A combination of MTA apical plug and PRF was placed to fill the bone defect to accelerate the healing process by acting as a scaffold as done by Jayalakshmi KB et al [6]. Other newer modalities of retrieval of a fractured instrument reported include atraumatic extraction and removal of the fractured instrument extraorally followed by replantation [7].
preservation, reconstruction of osseous defect, sinus lift procedures, alveolar ridge augmentation etc [7, 10]. PRF has been considered in this case as it protects the surgical site, promotes soft tissue healing and when used in combination with hydroxyapatite, an osteoconductive material, it enhances bone regeneration [11].
REFERENCES
10. Porrini M, Rossi M, Bosotti M, Landi M, Bossi E, Marino S, Spadari F. Plasma cell chronic gingivitis: a case report. In Congresso Nazionale del Collegio dei Docenti Universitari di discipline Odontostomatologiche (CDUO). 2019; 11: 260-261.








































































































































