Management of an Esthetic Dental Implant Complication: A Case Report
- 1. Nova Southeastern University College of Dental Medicine, USA
Abstract
The 3-dimensional positioning of a dental implant is a key factor in achieving an adequate esthetic result. If a dental implant is placed too far facially, especially in the maxillary anterior sextant, gingival recession can be expected, which eventually may lead to a compromised esthetic result. This clinical case report represents the surgical and prosthetic management of a 5 mm gingival recession over implant #8 due to an inadequate buccal-lingual position of the dental implant as well as an overcountoured provisional crown. Numerous techniques for addressing dental implants esthetic complications have been described in the literature; however the predictability and long term success of such procedures is yet to be determined. Surgical management and treatment consisted on the debridement of the granulomatous tissue and encapsulated previous xenograft bone particles, air abrasion of the implant with aluminum oxide particles, and application of tetracycline paste over the implant surface. FDBA (RegenerOss Allograft, Biomet 3i, Palm Beach Gardens, FL, USA), rhPDGF-BB (GEM 21s, Osteohealth, Shirley, NY, USA), a resorbable cross-linked collagen membrane (OsseoGuard Flex, Biomet 3i, Palm Beach Gardens, FL, USA) and a palatal pedicle graft were chosen and used.
Keywords
• Esthetic complication
• Implants
Citation
Espona J, Hernandez MA (2013) Management of an Esthetic Dental Implant Complication: A Case Report. JSM Dent 1(3): 1018.
INTRODUCTION
Over the past decade there has been a steady increase in the number of dental implants placed in the United States and growth in the field of implant dentistry is projected to continue at approximately 12% annually [1].
Implant esthetic complications are very demanding for the clinical practitioners. These complications can be caused by many factors including but not limited to, malposition implants and overcontour restorations. Reproduction of the form and function of a single tooth, including the papilla and the facial gingiva, is paramount when it comes to restoring aesthetics. If the initial scenario is ideal, esthetic results are based on more controllable factors involving the 3-dimensional position of the implant within the surrounding hard and soft tissue [2].
Proper implant placement is vital for a satisfactory and esthetic result [2]. If an implant is placed too far facially, recession can be expected [3,4,5,6], leading to an esthetic implant failure. Similarly, an over-contoured abutment or restoration can worsen this recession by displacing the soft tissues more apically [7].
The literature describes numerous techniques to be used in addressing dental implant esthetic complications [8,9,10,11], however the predictability and long term success of such techniques and procedures are yet to be determined, especially in the anterior region.
METHODS
A healthy 40-year-old presented to the Postgraduate Periodontics dental clinic at Nova Southeastern University, College of Dental Medicine, Fort Lauderdale, Florida. His chief complaint was the uneven gingival margins between teeth #8,9 and a dark shadow underneath the gingiva in tooth #8. The past dental history revealed an implant-supported restoration on site #8 with a 5mm facial gingival recession. Also, tooth #7 presented with loss of periodontal attachment as well as scar tissue from previous surgeries (Figure 1).

Figure 1 Pretreatment view showing gingival recession, scar tissue and provisional restoration of implant #8.
Radiographic examination revealed normal bone levels (Figure 2).

Figure 2 Periapical radiograph of implant #8 showing adequate bone.
Alternative treatment plan options were presented and discussed with the patient, including removing implant #8, grafting and replacing at a later time. However, treatment option of soft tissue and hard tissue grafting over implant #8 was chosen.
The temporary crown and healing abutment were removed and a cover screw was placed over implant #8. A tooth supported provisional restoration was placed (Figure 3).

Figure 3 New provisional restoration and placement of a cover screw on implant #8.
After 6 weeks soft tissue grew over the cover screw and patient was ready for the corrective soft and hard tissue surgery.
Topical and local anesthetic were applied. Crestal incision was performed from palatal line angle to line angle of teeth #7,9. Two vertical apically divergent incisions were performed at the mesial line angles of #7 and #9 to ensure a broad blood supply to the flap, which was reflected full thickness. Upon flap reflection, the implant showed a significant loss of buccal bone plate (Figure 4).

Figure 4 Surgical flap showing implant #8 with facial bone loss and granulomatous tissue and encapsulated bone graft particles.
Granulomatous tissue and encapsulated xenograft particles were removed by mechanical debridement, using titanium curettes and aided by ultrasonic instruments. Air abrasion of the implant was then performed with aluminum oxide particles to remove any remaining granulomatous tissue and to resurface the implant. Thorough irrigation was performed with saline solution and Chlorhexidine 0’12%. Tetracycline paste was then applied for 2 minutes and then a second irrigation was conducted (Figure 5).

Figure 5 Surface conditioning of the implant with tetracycline
The defect was grafted with FDBA (RegenerOss Allograft, Biomet 3i, Palm Beach Gardens, FL, USA), rhPDGF-BB (GEM 21s, Osteohealth, Shirley, NY, USA) and covered with a resorbable cross-linked collagen membrane (OsseoGuard Flex, Biomet 3i, Palm Beach Gardens, FL, USA) (Figure 6).
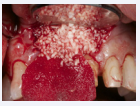
Figure 6 Freeze dried bone allograft placed in conjunction with rh-PDGF BB and covered by a cross-linked collagen membrane.
A split thickness incision was performed in the palate from distal line angle of tooth #7 extending to tooth #3 at about 2mm from the gingival margins. Tissue was undermined with a 15 blade 5 mm away from the incision to obtain sub epithelial connective tissue. Connective tissue was harvested, but it remained attached at the most anterior region to preserve its blood supply. The palatal pedicle flap was rolled over the collagen membrane to increase the blood support and to thicken the gingival complex, and to cover a 3x3mm soft tissue dehiscence that was present in origin (Figure 7,8)

Figure 7 A palatal pedicle graft was rolled over the membrane to provide adequate tissue thickness and increase the blood supply.

Figure 8 Buccal view of the bone and soft tissue graft prior suturing.
Flaps were sutured with 6/0 PGA sutures and the tooth supported provisional restoration was recemented (Figure 9,10)

Figure 9 Flaps were sutured with 6/0 poliglactin multifilament sutures.

Figure 10 Immediate postoperative with the acrylic bonded provisional in place
RESULTS
At one week postoperative visit, the surgical site appeared to be healing within normal limits with slight swelling, but no signs of infection could be detected. The palatal donor site presented with sloughing, however the patient reported no pain (Figure 11, 12).
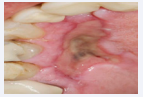
Figure 11 One week post-operative palatal donor site.

Figure 12 One week postoperative view of the buccal site.
At four weeks postoperative visit healing normally progressed, and the palatal tissue, which sloughed, was epithelialized (Figure 13).

Figure 13 Healing at 4 weeks. Epithelization of the palatal donor site and adequate buccal contours.
At six weeks postoperative visit soft tissue healing appeared to be complete and individual composite temporary crowns were placed (Figure 14).

Figure 14 Individual composite temporary crowns.
The emergence profile of #8 was carefully developed. Critical contour followed the shape of #9 and subcritical contour was undersized, especially on the buccal, to prevent future recession.
At six weeks postoperative visit soft tissue healing appeared to be complete and individual composite temporary crowns were placed (Figure 14). The emergence profile of #8 was carefully developed. Critical contour followed the shape of #9 and subcritical contour was undersized, especially on the buccal, to prevent future recession.
At six weeks postoperative visit soft tissue healing appeared to be complete and individual composite temporary crowns were placed (Figure 14). The emergence profile of #8 was carefully developed. Critical contour followed the shape of #9 and subcritical contour was undersized, especially on the buccal, to prevent future recession.
At three months, the gingival margins of the two central incisors were in harmony. Probing depths around #8 were 3,3,3 with no bleeding or suppuration. Although, there was an improvement in soft tissue thickness and attached gingiva, there is a 2 mm recession at the mesiobuccal line angle of tooth #7, probably due to the number of surgeries perform on this patient. (Figure 15)

Figure 15 Individual composite temporary crowns.
Patient is currently undergoing orthodontic and restorative treatments.
DISCUSSION
This clinical case report represents the importance of preoperative planning and clinical assessment before placing dental implants in the esthetic zone. It also shows the importance of proper 3- dimensional implant placement and how challenging and demanding malposition complications can be.
The successful treatment of an implant esthetic complication due to a malposition of the dental implant is often to be determined by the degree of the malposition, the diameter and the design of the implant [8].
The treatment goal for this patient was to improve the gingival recession over implant #8 as well as to provide a more adequate gingival tissue thickness over implant #8. By using a combination of soft and hard tissue grafting as well as a surface treatment, a more coronal position of the gingival margin was accomplished, giving better harmony with the adjacent dentition, and improving the thickness and quality of the tissues.
Corrective soft and hard tissue surgeries are challenging, especially around implants, as they lack the vasculature that the periodontal ligament provides. After each surgical procedure, tissues become weaker and more rigid, as the scar tissue increases and there is less vascular support [12,13,14] When the patient presented to the clinic, he had already undergo 3 surgical procedures, consisting in extraction and socket preservation, implant placement and second stage surgery. This gave us a more challenging environment. The use of biologic modifiers improves the initial cell recruitment and vascularity [15], which in this case were paramount. In addition, the use of a pedicle palatal connective tissue graft allowed us with more blood supply to the grafted area.
However, despite all our efforts, we ended up with some recession in the mesial line angle of #7. If we attempted another surgery in this same region, we could severely compromise the results already achieved. Therefore, decision was made to have the patient undergo orthodontic treatment (slow force eruption #7) hoping that this will allow a more coronal displacement of the hard and soft tissues as the tooth erupts.
CONCLUSIONS
3-dimensional position of dental implants and proper abutment and restoration contours are vital for achieving a successful esthetic outcome. Various authors have proposed different techniques for addressing esthetic failures. Here we propose another treatment alternative to compensate hard and soft tissue deficiencies around an implant supported restoration.








































































































































