Periapical radiolucencies in healthy human mandibular molars with fused roots
- 1. Texas A&M University Baylor College of Dentistry, Assistant Professor, Department of Endodontics
- 2. University of California at San Francisco School of Medicine, Assistant Professor, Department of Epidemiology & Biostatistics
- 3. Texas A&M Baylor College of Dentistry, Clinical Assistant Professor, Department of Biomedical Sciences
- 4. Columbia University College of Dental Medicine, Professor, Division of Endodontics
Abstract
Objective: To evaluate the possible prevalence of periapical radiolucencies related to healthy mandibular molars with fused roots.
Material and Methods: Full mouth series consisting of periapical films of 731 patients were evaluated. The following data was recorded for each patient: gender; total number of mandibular 1st and 2nd molars; number and location of molars with fused roots; and number and location of healthy fused-rooted molars with periapical radiolucency. Only the patients with radiographically healthy molars were included in the study (teeth with absence of radiographically visible deep caries or filling materials).
Results: Of all the 1st and 2nd molars (2924) in the study, 82 (2.8%) had complete radiographic display of root fusion. Adding fused-rooted third molars brought the number to 133. Of the 133 fused-rooted healthy molars (including 3rd molars) 44 manifested periapical radiolucency (33.08%), including 2 of 3 1st molars, 22 of 79 2nd molars, and 20 of 51 3rd molars (P > .05).
Conclusion: Periapical radiolucencies associated with human, healthy mandibular molars with fused roots exist, and they are not uncommon. Therefore, it is important to do a thorough clinical and radiographic assessment when evaluating pulpal and periapical status of lower molars with fused roots.
Keywords
- Mandibular molar
- Fused roots
- Periapical radiolucency
Citation
Jalali P, Mirzazadeh A, Tahmasbi M, Hasselgren G (2021) Periapical radiolucencies in healthy human mandibular molars with fused roots. JSM Dent 9(1): 1137.
INTRODUCTION
Endodontic-related inflammatory lesions, notably the periapical granuloma and cyst, are the most commonly found periapical radiolucencies (1). However, other pathological processes and anatomical variations can be misdiagnosed as periradicular lesions of endodontic origin leading to faulty diagnoses and resulting in unnecessary treatments. Aberrant anatomic variations may manifest as radiolucencies that can be interpreted in panoramic or periapical radiographs as endodontic lesions. Reported cases include the mental and incisive foramina, (2), maxillary sinus (3), salivary glands (4), Stafne’s bone defect (5), and canalis sinuosos (2). In addition, artifacts caused by film processing can also mimic endodontic lesions (6). There is anecdotal evidence that human, healthy, mandibular molars with fused roots occasionally show periapical radiolucencies (7). These radiolucencies have the appearance of endodontic-related inflammatory lesions, and can be misinterpreted and result in unjustified root canal treatment. To the best of our knowledge there is no study or case report relating such radiolucencies to fused-rooted mandibular molars with normal pulps. Therefore the purpose of this study was to evaluate the possible prevalence of periapical radiolucencies related to mandibular molars with fused roots.
MATERIALS AND METHODS
Study charts were randomly selected from charts of a patient pool that presented for triage at Columbia University College of Dental Medicine. Only patients who had radiographic full-mouth series taken with paralleling technique were included into the study. Inclusion criteria were as follows:
(i) Patients >18 years old,
(ii) Bilateral presence of mandibular 1st and 2nd molars,
(iii) Absence of radio graphically visible deep caries or filling materials (less than 1/3 of dentin thickness),
(iv) Teeth with fully developed roots.
Exclusion criteria included patients < 18 years old, absence of one or more of the mandibular 1st and 2nd molars on either side, teeth with deep caries, fillings and any evidence of root canal or vital pulp treatment, and teeth with immature roots. The protocol was approved by Columbia University Irving Medical Center Institutional Review Board. Two observers examined the periapical radiographs of mandibular molars, and the following data was recorded for each patient: gender; total number of mandibular 1st and 2nd molars; number and location of molars with fused roots; and number and location of fused-rooted molars with periapical radiolucency. The total number of first and second mandibular molars were counted and registered. The total number of third molars could not be registered as these teeth were not always fully depicted in the full mouth series. Therefore only 3rd molars with fused roots visible in radiographs were registered. Any discrepancy between the two evaluators was solved by a re-evaluation of the radiograph(s) and a discussion.
The determination as to whether molar roots were fused was based on radiographic evaluation. The following criteria were used to define a fused-rooted molar (8). Any molar that had one root or roots fused in the apical-third (regardless of the occurrence of fusion in middle-third or coronal third) was considered a molar with fused roots. Therefore, only molars with one radiographic apex were included in the study.
Periapical radiolucency was defined as a unilocular radiolucency attached to the apex of a fused-rooted mandibular molar without any lamina dura between root and lucency (Figure 1).

Figure 1 Radiograph showing a mandibular second molar with a periapical radiolucency.
Radiographically these lesions looked similar to a periapical lesion of endodontic origin with Periapical Index Score 4 according to the scoring system devised by (9). Was used for data analysis. Study outcomes were reported as frequency/ percentage and compared between the groups using Pearson Chi Square test or Fisher’s exact test (where appropriate).
RESULTS
Based on the inclusion criteria, 731 full mouth series (341 from males and 390 from females) with 2924 mandibular 1st and 2nd molars were included into the study. Of all the 1st and 2nd molars in the study, 82 (2.8%) had complete radiographic display of root fusion. Roots of mandibular 2nd molars were fused more frequently than those of 1st molars with 0.21% of mandibular 1st molars exhibiting root fusion, compared to 5.4% of 2nd molars (P<0.05). In addition, among the 1st and 2nd molars in males (1364) and females (1560) the incidence of root fusion was significantly higher in females than males (P<0.05) (Table I).
Table 1: Number of fused-rooted 1st and 2nd mandibular molars.
| Male (341) | Female (390) | Female and Male (731) | ||||
| Fused-molar n(%) |
Total molar N |
Fused-molar n(%) |
Total molar N |
Fused-molar n(%) |
Total molar N |
|
| 1st Molar | 2 (0.29) | 682 | 1 (0.13) | 780 | 3 (0.21) | 1462 |
| 2nd Molar | 18 (2.64) | 682 | 61 (7.82) | 780 | 79 (5.4) | 1462 |
In the same population 51 fused-rooted 3rd molars were found. Hence, a total of 133 fused-rooted mandibular molars (Three 1st molars, seventy nine 2nd molars, and fifty one 3rd molars) were evaluated for the presence of periapicalradiolucency. Of the 133 fused-rooted molars, 44 manifested periapical radiolucency (33.08%), including 2 of 3 1st molars, 22 of 79 2nd molars, and 20 of 51 3rd molars (Table II).
Table 2: Number of fused-rooted mandibular molars with periodical radiolucency. The differences between the groups are not significant.
| Fused-rooted molars with periapical radiolucency n(%) |
Total molars n(%) |
95% confidence interval | |
| 1st | 2 (66.67) | 3 | .09 - .99 |
| 2nd | 22 (27.85) | 79 | .18 - .39 |
| 1st&2nd | 24 (29.27) | 82 | .19 - .4 |
| 3rd | 20 (39.22) | 51 | .25 - .53 |
| Total | 44 (33.08) | 133 | .25 - .41 |
There were no statistically significant differences found among the three groups.
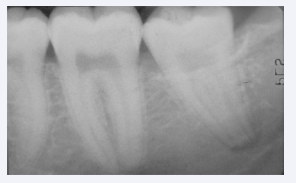
Figure 2 Radiograph showing a mandibular third molar with a periapical radiolucency.
DISCUSSION
The prevalence of fused-rooted mandibular molars varies in previous studies between 0.4% and 32.1% (8, 10, 11). The wide spread may be due to differences in fused root determination criteria and often extracted teeth were used. We evaluated root fusion only by periapical radiographic observation so our criteria for root fusion were different from earlier studies. We defined root fusion as a complete fusion of the roots only if a single apex could be visualized radiographically. The full mouth series used in this study did not always completely depict the mandibular third molars and it is therefore likely that the true number of fused root molars was higher. Still, as the intention was to evaluate a possible prevalence of periapical radiolucencies related to fused mandibular molar roots, we used the images that were available. Since the present study was a cross sectional radiographic study, we were not aware of the pulpal status of the fused-rooted molars. The fused-rooted molars that were included into the study were either virgin or affected by shallow caries or had small restorationsand it would seem unlikely that the periapical radiolucencies originated from endodontic infection. Although pulp necrosis, in the absence of deep caries or restorations, can be caused by longitudinal cracks (12), trauma or orthodontic treatment it is inconceivable that the incidence of pulp necrosis should be as high as the number of periapical radiolucencies found in the study. The question is what is the nature of the tissue, which is manifested as periapical radiolucency? Unfortunately, the answer to this question is unclear. It has been shown that widened PDL space could be visualized in teeth with normal pulps and Regardless, in the present study, the periapical radiolucencies were larger than a merely widened PDL space. Hypothetically, could this be the result of failure of epithelial diaphragm resorption? Normally, the epithelial diaphragm disappears after root maturation (13), to the best of our knowledge, there is no published evidence showing remnants of epithelial diaphragm after closure of the apices. Around a third (33.08%) of fused-rooted mandibular molars showed periapical radiolucencies. All of the teeth included in the study were mature with radiographically closed apices, therefore the possibility that the radiolucencies visualized in the present study were apical papilla tissues could be ruled out. In addition, it is very unlikely that theradiolucencies were the result of mental foramen superimposition since the mental foramen is usually not located below or posterior to the first molars (14) The inferior alveolar nerve canal can be superimposed radiographically on the apices of mandibular molars, but it appears as a radiolucent band, which can seldom mimic a lesion of endodontic origin. Stafne’s bone cavities can also mimic a lesion of endodontic origin (15), but the prevalence of these cavities is very low (0.009%) (16). Marrow spaces in the mandible may coalesce and create large radiolucent areas, in which if they are superimposed on the apices, they might be misinterpreted as endodontic pathosis (17). Mostly these can be distinguished from endodontic pathosis by tracing of the intact lamina dura and periodontal ligament space. Still, could it be possible that the concentration of forces from a large conic root shape encourages the formation of larger marrow spaces? Presently, the true explanation for the presence of the periapical radiolucencies is unknown, but it must be emphasized that this is not a pathological process rather a variation of normal anatomy. As mentioned earlier the numbers obtained in this study are not absolute as the radiographic full mouth series did not constantly depict third molars. Still, the results show that periapical radiolucencies at human, healthy mandibular molars with fused roots exist, and that they are not uncommon. Therefore, it is important to do a thorough clinical and radiographic assessment when evaluating pulpal and periapical status of lower molars with fused roots. The true nature of the radiolucent areas associated with fused molar roots is unknown. Further studies may benefit from studies integrating histology and computed tomography.
CONCLUSION
Periapical radiolucencies associated with human, healthy mandibular molars with fused roots exist, and they are not uncommon. Therefore, it is important to do a thorough clinical and radiographic assessment when evaluating pulpal and periapical status of lower molars with fused roots.
ACKNOWLEDGEMENT
The authors want to acknowledge the work of the late Dr. Neill Serman who enthusiastically participated in the beginning of this study.
REFERENCES
6. Horner K. Film fault artefact mimicking a periapical radiolucency. Br Dent J 1988; 165: 21–22.
7. Strindberg LZ, Kompendium i Endodonti, Kungliga Tandläkarhögskolan, Stockholm, Sweden. (Compendium in Endodontics. Royal School of Dentistry). 1968.








































































































































