Adenoid Hypertrophy in Adults
- 1. Department of ENT, KEM Hospital, India
Abstract
Adenoid tissue is one of the first line immunological defense mechanisms for the upper aero-digestive tract and reaches its maximum size between 3-7 years of age. Its atrophy starts from 10 years and is usually complete by 20 years of age. However, in the current clinical practice, we do encounter adenoid hypertrophy in adult patients. Persistence of adenoid tissue in adults is either due to chronic inflammation or reproliferation of regressed adenoid tissue. Important predisposing factors are pollution and smoking. Adenoid hypertrophy most commonly presents with snoring or bilateral nasal obstruction. Our case report describes a 31-year-old female with snoring and nasal obstruction who was diagnosed with adenoid hypertrophy by a flexible nasal endoscopy and confirmed with a CT scan. She underwent adenoidectomy as a two-step procedure, starting with the conventional curettage and removal of the bulk followed by removal of the remnant tissue with the help of a Coblation. The diagnosis was confirmed by histopathological examination of the tissue removed by curettage. Coblation adenoidectomy is becoming popular as an alternative technique for adenoidectomy, as it helps in complete removal with minimal blood loss. Adenoid hypertrophy should always be considered in the differential diagnosis of adults suffering from bilateral nasal obstruction.
Citation
Bidaye R, Desarda K, Thakkar J, William CS (2018) Adenoid Hypertrophy in Adults. JSM Head Face Med 3(1): 1007.
Keywords
• Adenoid
• Snoring
• Coblation
• Adenoidectomy
ABBREVIATIONS
CT: Computerised Tomography
INTRODUCTION
Santorini introduced the term ‘Nasopharyngeal Aggregate’ or ‘Luschka’s Tonsil’ in the 17th century, while the term ‘Adenoid’ was coined by Wilhelm in 1870 [1]. According to German literature incidence of adenoid hypertrophy is 2.5% in the adult population [2]. Adenoid hypertrophy is often underestimated in adults with nasal obstruction and is often misdiagnosed as a nasal or sinus pathology. Also, being prevalent in the pediatric age group is another reason for its underestimation [3]. we present to you a case of adenoid hypertrophy in an adult female who presented to us with nasal obstruction.
CASE PRESENTATION
A 31-year- old woman presented with complaints of bilateral nasal blockage, mouth breathing and snoring since the last 3 years. The complaints were continuous and affected her quality of sleep. There was no history of any allergies. Physical examination did reveal reduced nasal air blast bilaterally and a hypo nasal voice. The nasal septum and the turbinate examination were within normal limits. A trans-nasal Flexible Nasopharyngoscopy was performed under local anaesthesia which revealed a mass in the nasopharynx obstructing the choana. A CT scan was performed to confirm our diagnosis and to rule out any sinus pathology. The enlarged mass in the nasopharynx was suggestive of adenoid tissue hypertrophy on the CT scan. It was classified as grade 3 adenoid hypertrophy according to Clemens and Mcmurry classification (Table 1). The patient was counselled for an Adenoidectomy with histopathological examination of the tissue after the surgery. Preoperative investigations with the coagulation profile were within normal limits. Surgery was performed under general anesthesia with an oral endotracheal tube. Nasal decongestion was done with cotton pledgets soaked in 1:10000 adrenaline solution. An O° 4mm rigid endoscope was introduced in to the nasal cavity. Hypertrophied adenoids were visualized and documented. Figure 1
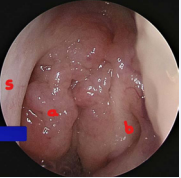
Figure 1 Nasopharynx seen through the Left nasal cavity a. Adenoid tissue, b. Eustachian tube opening, s. Nasal septum
With a Boyle-Davis mouth gag splinting the mouth open, the adenoids were removed using St.Claire Thompson Adenoid Curette. Homeostasis was achieved by using saline soaked gauze pack in the nasopharynx. After a few minutes the pack was removed, and the soft palate retracted with an 8F suction catheter which was introduced through the nostril. Remnants of adenoid tissue in the superior quadrant and near the Eustachian tube openings were removed using a Coblator wand which was introduced per orally. The Coblator wand Evac 70 was bent at an angle of 30°. This arrangement helps us to reach the remnant tissue at the edges with ease. Homeostasis was achieved using the coagulation mode on the wand (Figure 2).
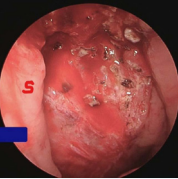
Figure 2 Complete adenoid tissue removal and haemostasis achieved, s. Nasal Septum.
The specimen caught in the adenoid curette was sent for Histopathological Examination. Antibiotics, antihistaminics, analgesics & steroids were administered as tablets for the next 6 days. Histopathological examination revealed adenoid tissue showing reactive changes with many lymphoid follicles with germinal centers are seen. Follow up of the patient after 4 weeks showed good recovery with significant reduction in symptoms.
Table 1: Clemen’s et al [13] classification of Adenoid grade.
| Grade | Adenoid tissue |
| 1 | Adenoid tissue filling one third of vertical portion of choana |
| 2 | Adenoid tissue filling one third to two third of choana |
| 3 | From two third to nearly complete obstruction of choana |
| 4 | Complete choanal obstruction |
DISCUSSION
Adenoid enlargement occurs most commonly between the age of three and seven years. Atrophy usually begins after 10 years of age and is complete before the age of 20 years [4]. In adults, adenoid hypertrophy causing nasal obstruction requires excision and a histopathological examination is required to rule out malignancy [5]. There is equal incidence of adenoid hypertrophy between male and females as per the study by Shetty et al., [6] However according to study done by Rout et al adenoid hypertrophy is more common in males as they are involved in outdoor activities and thus are exposed to more pollutants [1]. It frequently co exists with other nasal pathology like septal defect or turbinate hypertrophy in adults [7]. The persistence adenoid tissue in adults is due to chronic inflammation or re-proliferation of regressed adenoidal tissue in response to irritants or infection [8,9]. Finkelstein et al., has reported that obstructive adenoids in adults are more common in smokers [10]. Viral infection is also a causative factor in adults especially in an immune suppressed like organ transplants or a immune compromised state for example HIV/AIDS [11]. Benign lesions in nasopharynx in adults include cystic lesions like Brachial cleft cyst, Thornwaldt cyst and Mucus retention cyst [5]. Johnnsson et al., found that nasopharyngeal carcinoma was the most common malignant nasopharyngeal disease followed by Plasmacytoma, Lymphoma and Rhabdomyosarcoma.12 Mostafa et al., concluded that reactive lymphoid hyperplasia is the most common pathology encountered in nasopharynx of adult population followed by nasopharyngeal carcinoma and nasopharyngeal lymphoma. Nasopharyngeal cysts were the least diagnosed lesion [13].
Coblation technology is a non-heat driven process of soft tissue dissolution which makes use of bipolar radiofrequency energy [14]. Coblation is a form of controlled ablation. When current from radiofrequency probe pass through saline medium it breaks saline into sodium and chloride ions. These highly energized ions form a plasma field which breaks organic molecular bonds within the soft tissue causing its dissolution [15]. Surface temperature ranges from 40° to 70° Celsius and the ablation effect is primarily localized to contact area causing minimal damage to the adjacent tissue [16]. Coblation adenoidectomy technique has several advantages namely the reduced blood loss and reduction in pain intensity especially in children [17]. As it is combined with a direct endoscopic view of adenoid and the malleable wand has an ability to reach all areas of the nasopharynx, a complete removal of the adenoid tissue can be achieved. Another benefit of coblation adenoidectomy is the ability to use a single instrument to ablate and coagulate tissue. The only disadvantage would be the lack of tissue for Histopathological examination. Detection of mass in nasopharynx of an adult is usually associated with suspicious of nasopharyngeal malignancy. So we had to shave a part of the adenoids using a St. Clair Thomson adenoid curette to capture some tissue before using the Coblation wand. On histopathological examination in adults hypertrophied adenoid tissue usually has an intense chronic inflammatory cell infiltration and secondary changes like squamous metaplasia in surface epithelium and fibrosis. As compared to children who show the presence of lymph follicles with prominent germinal center as the main finding. An ENT surgeon should be aware of the incidence of adenoid hypertrophy in adults and should manage it appropriately with necessary investigations.









































































































































{kind=link}