Dental Anomalies in Opitz G or BBB Syndrome and Cleft Lip and Palate associated with Hypertelorism
- 1. Department of Dental Radiology and Imaging, University of São Paulo, Brazil
- 2. Department of Orthodontics, Sao Paulo State University, Brazil
- 3. Department of Pediatric Dentistry, University of São Paulo, Brazil
Abstract
G/BBB is a heterogeneous disorder, with variant X-linked inheritance associated with the chromosomal region Xp22. The aim of this cross-sectional study was to determine the prevalence of dental anomalies in individuals with Opitz G/BBB syndrome (G/BBB) and cleft lip and palate associated with hypertelorism (CLP/H) compared to two control groups. 22 individuals with G/BBB and 14 with CLP/H, above eight years of age, and two control groups paired for gender and age - non-syndromic cleft lip and palate (CLEFT), and without morphofunctional alterations (WMFA) composed the sample. Hypoplastic, hyperplastic and heterotopic anomalies were analyzed on panoramic radiographs, obtained before orthodontic treatment. The results were analyzed by descriptive statistics. Comparisons between groups was performed by the Dunn’s method, and the number of dental anomalies was evaluated by the Kruskal-Wallis test (p<0.05). All individuals with G/BBB syndrome and CLP/H presented at least one dental anomaly, with predominance of hypoplastic alterations, mainly anomalies of number as hypodontia and supernumerary teeth, followed by heterotopic alterations with predominance of rotation. The frequency of hypodontia and supernumerary teeth was significantly higher compared with WMFA group and without significant difference from the CLEFT group. Eight supernumerary teeth were identified in the mandibular midline and three mesiodens in the maxillary region. For diagnostic evaluation of individuals suspected to have these syndromes, it is suggested to investigate the occurrence of supernumerary teeth in the midline in both deciduous and permanent dentitions.
Citation
Rojas LV, de Oliveira Pinto R, de Carvalho IMM, da Silva Dalben G (2018) Dental Anomalies in Opitz G/BBB Syndrome and Cleft Lip and Palate associated with Hypertelorism. JSM Head Face Med 3(1): 1011.
Keywords
• Opitz syndrome
• Hypertelorism
• Tooth abnormalities
• Cleft lip
• Cleft palate
ABBREVIATIONS
CLP: Cleft Lip and Palate; H: Hipertelorism; WMFA: Without Morpho-Functional Alterations
INTRODUCTION
John Opitz first described the syndromes G [1] and BBB2 as two distinct disorders. G syndrome [1] received the name of a family whose surname began with letter G. Alike, the BBB [2] syndrome was described in three different families, all with last names beginning with letter B. Later, the author concluded that the two syndromes were actually part of the same condition with variable clinical features [3-6]. Since the initial description, this syndrome received different names according to the authors, including G/BBB syndrome, hypertelorism-hypospadias syndrome, hypertelorism-dysphagia syndrome, Opitz-Frias (OMIM, 2012) [6] and oculo-genito-laryngeal or Opitz syndrome [7].
G/BBB is a heterogeneous disorder, with variant X-linked inheritance associated with the chromosomal region Xp22 [2,7,8], causing specific mutation in the MID1 gene, and another variant with autosomal dominant inheritance located on chromosome 22 in region q11.2 [9], with male preference [3,8] yet still without gene identification [10-17]. Individuals with G/BBB syndrome present three main anomalies: hypertelorism, cleft lip and palate, and hypospadias, although they may have other defects in the body midline, especially in the craniofacial skeleton [18]. Manifestations may also include telecanthus, genitourinary anomalies (cryptorchidism in males), high arched palate, thin upper lip, laryngotracheal clefts, congenital heart disease [14,19] and gastrointestinal disorders (dysphagia, gastroesophageal reflux, imperforate anus). The face is typical with frontal bossing, flat filter, broad nasal bridge and nose, and small nostrils [14]. Individuals may also present low-set and malformed ears [6,20]. There may be agenesis or hypoplasia of corpus callosum and brain abnormalities, which can cause mild intellectual disability [21,22].
Individuals with non-syndromic cleft lip and palate may also have associated anomalies. Among these, the occurrence of cleft lip and palate associated with hypertelorism (CLP/H) is relatively common, not classified as G/BBB syndrome due to the absence of other characteristic signs of the syndrome. Cleft lip and palate is a congenital anomaly that can cause esthetic, emotional, and functional alterations [23]. Several dental anomalies are common in the deciduous or permanent dentition, with higher prevalence in the maxilla [24]. These anomalies appear to be determined embryologically and may occur at different stages of dental development [25].
CLP/H is a classification used by the Clinical Genetics team of HRAC/USP for a group of individuals who present as striking characteristic hypertelorism associated with cleft lip and palate, without other syndromes or disorders, which encouraged the present study to evaluate whether this group could represent an emerging sub-phenotype of the G/BBB syndrome.It might be argued that such combination of malformations could represent a milder form of the syndrome, not described in theliterature so far.
Fewreports are available on the oral characteristics of individuals with G/BBB syndrome. There are reports of cleft lip and palate, short lingual frenulum and large tongue [19,26] hypoplastic alterations with high frequency of microdontia and hypodontia, as well as supernumerary teeth in the mandibular midline and ankyloglossia [27], maxillary and mandibular hypoplasia [20,28-30], and micrognathia [19,31,32]. Conversely, no reports were found describing the dental findings in individuals with CLP/H.
Based on these aspects, this study determined the prevalence of dental anomalies in individuals with G/BBB syndrome and CLP/H, compared with control groups of individuals with non-syndromic cleft (CLEFT) and without morphofunctional alterations (WMFA). Such control groups were also included to differentiate which anomalies could be assigned to the presence of the cleft itself, regardless of its combination with syndrome (G/BBB) or with associated anomalies (CLP/H).
MATERIALS AND METHODS
The study was approved by the Institutional Review Board of the Hospital for Rehabilitation of Craniofacial Anomalies, University of São Paulo (HRAC⁄USP) and was conducted at the Oral Radiology Sector of HRAC/USP.
The inclusion criteria comprised panoramic radiographs of individuals with diagnosis of G/BBB and CLP/H from the database of HRAC/USP, registered since the hospital was established in June 1967 until November 2013, above eight years of age, with complete unilateral or bilateral cleft lip and palate, regardless of ethnicity or gender, and not submitted orthodontic treatment.
The prevalence of dental anomalies was compared with two control groups, the first composed of panoramic radiographs of 99 individuals with isolated, non-syndromic cleft lip and palate (CLEFT) registered in the database of the Oral Radiology Sector, HRAC/USP, and the second by 38 individuals without morphofunctional alterations (WMFA) obtained from analysis of pretreatment panoramic radiographs from the files of a private orthodontic clinic, paired for gender and age.
At baseline, there were 94 individuals registered with a clinical diagnosis of G/BBB syndrome. Some were excluded because they had no panoramic radiographs (24), had incomplete clefts (17), age younger than 8 years at the time of radiography (26), previous orthodontic treatment and tooth extraction (four) and poor-quality radiography (one). This led to a final sample of 22 individuals with 24 panoramic radiographs.
Regarding CLP/H, there were 64 individuals with clinical diagnosis. All these individuals had been diagnosed after thorough screening by the Genetics team of HRAC/USP, based on the clinical observation of cleft and hypertelorism, without other malformations. Among these, some were excluded because they had no panoramic radiographs (17), had incomplete clefts (15), age below 8 years (13), and previous orthodontic treatment and tooth extraction (five). This led to a final sample of 14 individuals with 14 panoramic radiographs.
The dental anomalies were assessed on panoramic radiographs obtained both by conventional system (Panoramic Apparatus Rotograph Plus - Vila SistemiMedicali, Buccinasco, MI, Italy) and digital system (Panoramic Kodak 8000, Eastman Kodak Company, Rochester, NY, USA). Conventional panoramic radiographs were selected on a light box in the Oral Radiology sector, then they were digitized (Hp 4554 scanner, Brazil) to enable the same standard of review as digital radiographs.
Tooth abnormalities of shape, position and number were classified as hyperplastic, hypoplastic and heterotopic alterations, following the methodology described by Dalben et al. (2008) [27]. Their occurrence was compared between the two study groups and the two control groups. The evaluations were performed by a single examiner using a computer (PC Hp Omni200, Brazil) in a darkened room in the Oral Sector, with 15-minute intervals between each group of five radiographs.
Method error
Intraexaminer agreement for the presence of tooth anomalies was determined by re-evaluation of 10 randomly selected panoramic radiographs for each group, including the control groups, after an interval of 15 days. The kappa coefficient was calculated separately for each tooth anomaly, showing perfect agreement, with Kappa values of 0.655 to 1.000 (minimum to maximum), p<0.001.
Analysis of results
The prevalence of tooth anomalies was determined by descriptive statistics. Multiple comparisons between study and control groups were assessed by the Dunn’s method. The mean number of tooth anomalies was assessed by the Kruskal-Wallis test. All statistical tests were applied at a significance level of p <0.05.
RESULTS AND DISCUSSION
The 22 individuals with G/BBB syndrome, all males, presented mean age 10.41 years (range 8.00 - 25.00). Among the individuals, two had complete right cleft lip and palate, four complete left cleft lip and palate, and 16 had complete bilateral cleft lip and palate. All individuals exhibited at least one type of tooth anomaly, ranging from one to six per individual, adding up to 56 anomalies, being 48.21% hypoplastic, 16.07% hyperplastic and 35.71% heterotopic. The CLP/Hgroup comprised 14 individuals, being six males and eight females, with mean age 11.43 years (range 8.00- 25.00), among which two individuals showed complete right cleft lip and palate, 5 complete left cleft lip and palate, and seven had complete bilateral cleft lip and palate. All individuals had at least one type of tooth anomaly, ranging from one to 5 per individual, adding up to 31 anomalies, being 48.38% hypoplastic, 12.90% hyperplastic and 38.70% heterotopic. Distribution of the types of tooth anomalies per individual in the study and control groups is presented in detail in Table 1 (alterations of shape, position and number).
|
Table 1: Distribution of type tooth anomalies in the study and control groups
|
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Nine types of tooth anomalies were observed in the study and control groups, with higher prevalence of alterations of number as hypodontia in 17 individuals and 9 individuals with supernumerary teeth primarily in the inter-incisor anterior region in the study groups (Figure 1,2).
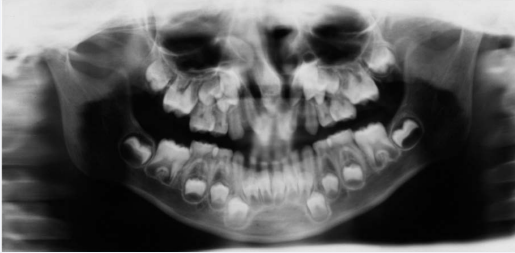
Figure 1 Supernumerary tooth in the lower anterior region, in an individual with G/BBB syndrome
In both control groups, alteration of position (mainly rotation) was the most prevalent tooth anomaly.
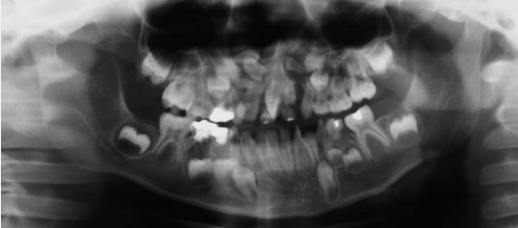
Figure 2 Supernumerary teeth in the upper anterior region, in an individual with CLP/H.
The mean number of tooth anomalies for all groups evaluated were 2.54 for G/BBB, 2.21 for CLP/H, 2.75 for CLEFT and 1.05 for WMFA, with statistically significant difference between groups according to the Kruskal-Wallis test (H=56.62, p = 0.001).
Hypodontia was observed in 36.36% and 32.26% of individuals with G/BBB and CLP/H respectively, and 29.29% and 2.63% of individuals in the control groups CLEFT and WMFA respectively, without statistically significant difference between G/BBB, CLP/H and CLEFT groups, yet these presented statistically significant difference compared with the second control group WMFA (Dunn method, p=0.001). Concerning the presence of supernumerary teeth and microdontia per individual in all analyzed groups, the multiple comparisons method revealed statistically significant difference between all study groups and the control group WMFA (Dunn’s method, p=0.021; p=0.030 respectively).
The G/BBB syndrome is agenetic disorder characterized by the presence of hypertelorism, cleft lip and palate and hypospadia. All individuals with G/BBB were males, agreeing with the literature [3,8], which reported higher prevalence in this gender.
All individuals with G/BBB and CLP/H had at least one type of tooth disorder, with predominance of hypoplastic alterations for both groups, agreeing with previous reports on the G/ BBB syndrome [27,29,30]. This occurrence is explained by the presence of complete unilateral and bilateral cleft lip and palate, associated with both disorders. Among the hypoplastic anomalies there was greater prevalence of hypodontia, in agreement with the presence of cleft lip and palate in these individuals [33].
This study revealed significant presence of supernumerary teeth in the study groups of individuals with G/BBB syndrome (16.07%) (Figure 1) and CLP/H (12.9%) (Figure 2), with greater frequency than observed in the control groups CLEFT (4.04%) and WMFA (2.63%). Supernumerary teeth were observed in 15 individuals in the G/BBB group, being nine between the lower incisors, five mesiodens between the upper incisors, and one between lower canine and premolar. With respect to the LP/H group, there were four supernumerary teeth, being one in the lower anterior region and three maxillary mesiodens.
The occurrence of supernumerary teeth in the cleft region is expected in a proportion of individuals [33], being rarely observed in individuals without morphofunctional alterations [23,34].However, the presence of supernumerary teeth near the midline in the upper and lower arches was a fairly consistent observation and could hardly be interpreted as an incidental finding, especially considering that the G/BBB syndrome is characterized as a midline developmental field disorder [20]. The literature reported the presence of supernumerary teeth in the anterior mandible in 33.33% of a sample of individuals with G/BBB syndrome [27], which was corroborated by the present results. Furthermore, the presence of supernumerary mesiodens in individuals with cleft lip and palate associated with hypertelorism was also significant, suggesting that the association of these anomalies can also represent midline developmental field disorders.
Several mechanisms of formation of supernumerary teeth have been suggested, including atavism, division of tooth buds, localized hyperactivity of dental lamina, or a combination of genetic and environmental factors [32]. Considering the present findings and previous reports in the literature, it would be possible to suggest that the same etiologic factors causing the disorders addressed in this study could also affect the dental lamina in the midline, with most pronounced effects in the mandibular region for G/BBB syndrome and in the maxillafor cleft lip and palate associated with hypertelorism.
CONCLUSION
In conclusion, the Opitz G/BBB syndrome and CLP/H presented at least one tooth anomaly, with predominance of hypoplastic alterations, mainly hypodontia, and high frequency of supernumerary teeth in the midline with predominance of mandibular alterations for G/BBB syndrome and in the maxilla for CLP/H, which were significantly higher compared with WMFA group and without significant difference compared to the CLEFT group.
According to the present findings, CLP/H could be considered an intermediate disorder between individuals with G/BBB syndrome and CLEFT, taking into account the presence of supernumerary teeth and alterations in the body midline, observed in the maxilla and mandible respectively, which may facilitate the diagnosis in individuals suspected to have these syndromes.
REFERENCES
6. University JH. Online Mendelian Inheritance in Man. OMIM(TM). 2012.
10. Kimmelman CP, Denneny JC. Opitz (G) syndrome. Int J Pediatr Otorhinolaryngol. 1982; 4: 343-347.
13. Lacassie Y, Arriaza MI. Opitz GBBB syndrome and the 22q11.2 deletion. Am J Med Genet. 1996; 62: 318.
17. Allanson JE1. G syndrome: an unusual family. Am J Med Genet. 1988; 31: 637-642.









































































































































{kind=link}