Diagnosis of the Prevalence of Bruxism in HIV or AIDS Patients, Associated with Psychological Factors: Pilot Study
- 1. Department of Dentistry, Universidade Paulista, Brazil
Abstract
The Human immunodeficiency vírus (HIV) is a pathology that caused a global pandemic, developing a series of social and psycological problems on the population like conflicts, preconceptation, self discrimination, anguish, depression, rejection, abandonment, social isolation, fear to die, etc. Being those cofactors of stress it can influence directly making some conditions worse like bruxism. This study contains a sample of 14 patients with positive HIV, a clinic exam followed by 15 questions about stress factors, habits and the influence of HIV on the patients life’s. According to the research, 64,28% of the interviewed patients presented bruxism, a highest percentage comparing with the general population (8 to 21%), 9 patients (64,28%) with joint changes, joint blockage or dislocation was reported on 4 patients (28,57%) and only 2 were following the treatment. The bruxism patients, only 2 never had symptoms of HIV or medication, 2 reported thinking on the actual health condition and 7 think a lot, none of the patients that had never thought about their health condition had bruxism, 7 of 10 bruxist patients reported that think sometimes and 1 reported that think with frequency. It was conclude that the prevalence was higher on HIV patients when compared to the not HIV population. The psycological profile showed an influential factor, being worse on bruxist patients.
Citation
Juvino AC, Pereira CB, Tini GF, Noro Filho GA, Mesquita AM, et al. (2017) Diagnosis of the Prevalence of Bruxism in HIV/AIDS Patients, Associated with Psychological Factors: Pilot Study. JSM Head Face Med 2(1): 1004.
Keywords
• HIV
• Bruxism
• Psycological aspects
INTRODUCTION
Syndrome of Human immunodeficiency (AIDS) is caused by the Human Immunodeficiency Virus (HIV) that can be transmitted by sexual contact, blood and vertical contamination; affects mostly the immune system and nervous system making the clinic symptoms look like opportunistic infections; taking to the higher stage of AIDS desease [1,2].
The cure and vaccines to prevent AIDS hasn´t being developed, although antiretroviral were discovered acting on inhibition of HIV replication, so the viral load stays lower and improves the immune system, with great benefit in reducing mortality and morbidity [3-6]. It’s important to recognize the importance of multi professional treatment for those patients, with emphasis on dental and psychological treatment, since we know that there are sequela and psychological consequences.
It’s possible to see psychological changes on the HIV/AIDS patients during all the phases since the suspected contamination to the disease evaluation. Studies have shown that emotion changes happens because of the death possibility, fear, anxiety, uncertain prognosis, effects of medication, isolation and rejection; depression caused by lack of cure, self blame, and limits imposed by illness; anger and frustration, the inability to overcome the virus and the uncertainty of the future, guilt for the possibility and to have infected others involuntarily and obsessive problems due to concern about illness and death, and a tendency to avoid new infections [7].
Social unpreparedness often leads the HIV/AIDS sufferer to fell doomed to death, along with fear and distress, may contribute to increase stress. Stress can cause a change on the organism with the intention of adapting, causing degeneration of immune system, reaching even more the defense of those individuals [8- 10]. As symptoms of stress we have depression, discouragement, apathy, emotional hypersensitivity, irritability, anger, anxiety and, in addition, we have contributing stress of various diseases [11-13].
Among the diseases that have stress as one of its contributing factors to the cause is bruxism. Bruxism is tooth contact in movements that are different from normal functions, and may be static or dynamic, usually during sleep and unconsciously [14]. The etiology is complex and multifactorial, often associated with emotional stress and occlusal problems or both. The psychoemotional factor is related to a tendency of bruxist patients use their stomatognathic apparatus as a means of downloading aggressive feelings [15-16].
In the diagnosis of bruxism, we detected during the anamnesis an account of fatigue and muscular pain, the patient may report that it grinds the tooth at night and may complain of roughness or dental hypersensitivity. At the clinical exam, we can visualize dental wear, dental hypermobility without periodontal disease, dental or restorative fractures, hypertonicity of the masticatory muscles with pain in some points, headaches and may still have changes in the temporo-mandibular joint with pain and discomfort, Joint blockage, dislocation, subluxation, crepitation, noise, degenerative changes, limitation of opening and restriction of movement15.
This research is justified not only by the above, but also by the contribution in the studies on infectious diseases, and may help Dental Surgeons and institutions to include a psychological approach to patients with HIV/AIDS, as well as to diagnose the prevalence of bruxism early in this Population, relating to psychological factors.
METHODS
The present study was developed at the Center for the Study and Assistance to Special Patients (CEAPE) at the Clinic of Dentistry of the Paulista University, Campus Indianópolis - São Paulo, Brazil, that performs dental care for patients with infectious and contagious diseases.Data collection took place, after approval by CEPUNIP 642/99. The subjects of the research were individuals HIV/AIDS.
Inclusion criteria: HIV/AIDS patients without complications from their current state.
Exclusion criteria: patients on psychiatric treatment, those who administer muscle relaxants or corticosteroids.
The research was carried out in three stages:
- Presentation of the research, clarifications and agreement with the Term of Free and Informed Consent.
- Delivery of a questionnaire related to psychological factors, which the patient answered in a quiet and alone environment. This questionnaire was composed of 15 questions that included: demographic data (age, sex, skin color, family income and education level); Uncovered reaction to HIV diagnosis; Impact of medication; How much HIV prevents daily activities; Opinion about the health service in relation to the treatment; Count your current health condition; Symptoms; How much do you think about your health condition; Satisfaction with current health; Stress or sadness for health; preconception; quality of life; Satisfaction with sleep; Frequency of negative feelings, and situations that cause you stress.
- Execution of a clinical examination directed to the diagnosis of bruxism and joint alterations, evaluating: custom of grinding or grinding of teeth; Chewing muscles; Jaw locking episode; click; Ladder of pain; Crackling; Mandibular mobility index; Tooth wear; Use of a device for bruxism and need for treatment.
Subsequently the data were analyzed and tabulated
RESULTS
The total sample consisted of 14 patients, 5 (35, 71%) of the female gender and 9 (64, 28%) of the male gender. Of this sample, as for race, 8 being considered as white, 5 as mulattos and 1 black. The mean age was 44.07 years old, being aged between 42 and 62 years of age.
The general and oral pathologies found in these patients were: Pneumonia; Candidiasis esophagus; Toxoplasmosis; Oral candidiasis; Cytomegalovirus; Herpes zoster; schizophrenia; Pulmonary metastasis and syphilis.
As for the CD4 count, only 1 interviewee had below 300 and for viral load, the majority (64, 28%) had undetectable load regarding the psychological aspects (Table 1)
|
Table 1: Data obtained from the psychological questionnaire applied to HIV/Aids patients. |
||||||||||||||
|
Patients |
Reaction to discovery
|
Impact of medication
|
How much HIV prevents daily activitys
|
Health Service
|
For those who tell about their health
|
Symptoms |
How much do you think about your health?
|
Satisfaction with health
|
Stress or sadness by the condition |
Preconception
|
Quality of life
|
Sleep quality
|
Frequency of negative feelings
|
Factorsthat cause stress |
|
1 |
Surprised
|
medium
|
Nothing |
Good |
Family and doctor
|
Already had
|
Verymuch |
Satisfied
|
----------- |
Few Times |
Good |
Satisfied
|
Sometimes |
Transit and Financial Problems
|
|
2 |
Took time toaccept |
High |
medium
|
Great |
Family and doctor
|
Already had
|
Verymuch |
-------------- |
----------- |
----------- |
--------- |
------------- |
------------- |
Health condition
|
|
3 |
surprised
|
No impact
|
Nothing |
Great |
Family |
Never |
Verymuch |
Satisfied
|
----------- |
Few Times |
Good |
Satisfied
|
Sometimes |
Financial Problems |
|
4 |
surprised
|
No impact
|
Extremely
|
Good |
Doctor |
Never |
Verymuch |
Satisfied
|
Many times |
Many times |
Good |
Medium
|
Never |
Transit and health condition
|
|
5 |
Took time toaccept |
medium
|
Very few
|
Good |
Family |
Frequently
|
Verymuch |
Partially Satisfied
|
Few Times |
----------- |
Good |
Satisfied
|
Sometimes |
Transit and health condition
|
|
6 |
Took time toaccept |
medium
|
Very few
|
Good |
Nobody |
Already had
|
Notmuch |
Satisfied
|
Many times |
Many times |
Medium
|
Satisfied
|
Sometimes |
Family sickness
|
|
7 |
Took time toaccept |
Low |
Very few
|
Good |
Family |
Frequently
|
Verymuch |
Satisfied
|
Few Times |
Many times |
Good |
Satisfied
|
Sometimes |
Health condition
|
|
8 |
Took time toaccept |
medium
|
Very few
|
Good |
Nobody |
Already had
|
Notmuch |
Satisfied
|
Few Times |
----------- |
Good |
Insatisfeito
|
Frequently |
Traffic, Family Illness, Home and Financial Problem
|
|
9 |
Took time toaccept |
High |
Nothing |
Good |
Everyone |
Eventually
|
Verymuch |
Partially Satisfied
|
Few Times |
Many times |
Verygood |
Partially Satisfied
|
Sometimes |
Financial Problems and socializing with people
|
|
10 |
Normal |
medium
|
Very few
|
Good |
Nobody |
Eventually
|
Eventually
|
Satisfied
|
Few Times |
Few Times |
Good |
Partially Satisfied
|
Sometimes |
------------------------ |
|
11 |
surprised
|
No impact
|
Nothing |
Great |
Everyone |
Never |
Verymuch |
Satisfied
|
Never |
Never |
Good |
Partially Satisfied
|
Sometimes |
Financial Problems |
|
12 |
Normal |
No impact
|
Nothing |
Great |
Everyone |
Never |
Eventually
|
Satisfied
|
Never |
Many times |
Verygood |
VerySatisfied |
Never |
------------------------ |
|
13 |
Took time toaccept |
medium
|
Nothing |
Great |
Family and doctor
|
Already had
|
Notmuch |
Satisfied
|
One Time |
Few Times |
Good |
Satisfied
|
Sometimes |
Transit and Financial Problems
|
|
14 |
surprised
|
No impact
|
medium
|
Good |
Family |
Eventually
|
Eventually
|
Partially Satisfied
|
Few Times |
Few Times |
Good |
Satisfied
|
Sometimes |
Health condition
|
we obtained significant data: only 2 (14.28%) reported the finding as normal; 3 (21.42%) said they did not tell that they have AIDS for anyone, not even doctors and relatives; 10 (71.42%) have or already had symptoms; 8 (57.14%) reported thinking too much about their health condition; Only 1 (7.14%) never suffered prejudice; And 2 (14,28) reported never feeling negative feelings.
According to the survey, 64.28% of the interviewees presented bruxism (Figure1,2),
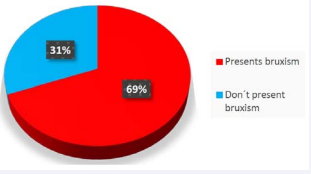
Figure 1 Prevalence of bruxism
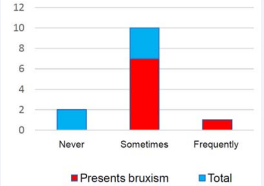
Figure 2 Evaluation of the health conditions for patients with bruxism in front of their thinking.
with the patients: 1, 2, 3, 5, 8, 9, 10, 11 and 14. Of the bruxist patients, 8 had noise or crackling articular, in addition to 1 patients who presented these signs and did not have bruxism, in a total of 9 patients (64.28%) with joint alterations. A blockage or dislocation episode was reported in 4 patients (28.57%), 3 of them had bruxism and 1didn´t . On the bruxist patients, 5 reported pain, 8 had dental wear and only 5 received some type of treatment for bruxism, and only 2 were still on treatment, thus 7 needed treatment.
Relating the bruxist patients to the psychological aspects we had: Only 2 never had symptoms resulting from HIV/AIDS or medication; 2 reported thinking eventually about their health condition and 7 think a lot; Only 1 suffered prejudice more than once, the other 8 suffered a few times or never suffered; Regarding the quantity that thinks about their health condition (Chart 2) we have that none of the patients who never think has bruxism, 7 in 10 patients with bruxism reported that they think sometimes and 1 reported that they think often.
DISCUSSION
According to the results, the prevalence in HIV/AIDS patients is higher than in the general population. 64.28 % in the HIV/AIDS population and 8-21% in the general population, according to Brown and Hong [17,18].
Considering also that 8 had joint changes and 8 had dental wear. Also, 7 needed treatment.
Knowing that the main damages caused by bruxism are: changes in the dentition, periodontium, masticatory muscles, temporo-mandibular joint, headache, behavioral and psychological effects [15,19,20-23], a different approach is required for The early diagnosis in patients with HIV/AIDS, before presenting the effects of the diseases, requiring more complex treatment.
In view of the psychological results, the importance of an intervention to this point is emphasized, since it is a population that has great emotional sequels, being important the motivation, valorization, bonding and humanization in all the treatment, also making it clear the necessity of amultiprofessional treatment, which is paramount to offer an integral service to these patients.
CONCLUSION
The prevalence of bruxism in HIV/AIDS patients is about 3 times higher than in the general population, which according to Brown and Hong is 8 to 21% and in HIV/AIDS patients is 64.28%. And the psychological pattern proved to be an influential and even more aggravating factor in patients with bruxism.
It is suggested that the Dental Surgeon, considering the high prevalence, can detect these contributing factors to bruxism during the treatment of HIV/AIDS patients and that makes the diagnosis early and immediate treatment. And that still, can offer a multi professional treatment to aid in the psychological aspect of these individuals.
It is necessary to study larger samples to increase the results.
REFERENCES
5. Johnson D. Therapeutic management of HIV. Oral Dis. 2002; 8: 17-20.
8. Hirata CHW. Oral manifestations in Aids. Braz J Otorhinolaryngol. São Paulo Mar./Apr. 2015; 81: 2.
16. Ramfjord SP, ASH MM. Oclusão. 3. ed., Rio de Janeiro: Guanabara, 1987.
21. Bahils A, Rodrigues NL, Ferrari E. Bruxismo. Revista Odonto Ciência. 1999; 27: 7-20.
22. Uetanabara R, Mazzetto MO. Bruxismo: Uma visão atual. Rev Odontol UNICID. 2000; 12: 163-169.









































































































































{kind=link}