The Use of Piezo Surgery for Surgical Treatment in Patients with Craniosynostosis - Case Report
- 1. Department of Oral and Maxillofacial Surgery, Hospital Santa Paula, Brazil
- 2. Department of Pediatric Neurosurgery, Hospital Santa Cecilia, Brazil
- 3. Department of Oral and Maxillofacial Surgery, Hospital Santa Paula, Brazil
- 4. Coordinator of Center for Studies and Special Service for Patients, Postgraduate Dentistry Courses, Brazil
Abstract
Craniosynostosis (CS) is as congenital malformation occurring at an incidence of 1:2000 live births, characterized by premature closure of one or more cranial sutures, resulting in cranial and craniofacial deformities in varying degrees and volumetric disproportion between the skull and the brain. The diagnosis is made by clinical observation after child birth and it can be confirmed by imaging tests such as X-ray and CT scan.
The treatment of CS is usually surgical in order to correct cranial distortion, craniofacial deformity, and prevent any future cognitive disorders and progression. The goal of this study was to evaluate the effectiveness of the use of Piezo surgery on a syndromic patient of 11 months who underwent surgical treatment of CS.
The study concluded that the Piezo surgery’s benefits include: Selective cutting of bone structures while preserving the soft tissue, improved accuracy of osteotomies for front orbital development, and reduced post-operative swelling.
Keywords
• Craniosynostoses
• Piezosurgery
• Craniofacial abnormalities
• Syndromic patient
Citation
Ferreira SP, Aguiar U, Tarquinio Marinho KC, Giovani EM, Lobo LF (2016) The Use of Piezo Surgery for Surgical Treatment in Patients with Craniosynostosis - Case Report. JSM Head Face Med 1(1): 1002.
ABBREVIATIONS
CS: Craniosynostosis; CT: Computed Tomography
INTRODUCTION
Craniosynostosis (CS) is as congenital malformation occurring at an incidence of 1:2000 live births, characterized by premature closure of one or more cranial sutures, resulting in cranial and craniofacial deformities in varying degrees and volumetric disproportion between the skull and the brain [1,2]. It leads not only to secondary distortion of skull shape but to various complications including neurologic, ophthalmic and respiratory dysfunction [3].
The diagnosis is made by clinical observation after child birth and it can be confirmed by imaging tests such as X-ray and CT scan [4].
Craniosynostosis is divided into two groups, simple or complex craniosynostosis. Simple craniosynostosis has single suture synostosis and complex one has multiple synostoses which show more severe cranial deformity and stenosis. According to associated developmental lesions, isolated (nonsyndromic) craniosynostosis shows only cranial deformities caused by synostosis and may have secondary neurologic or ophthalmologic manifestations which are derived from early fusion of cranial sutures [4-6].
There have been reported numerous number sofdiseases belonging tosyndromic cranio synostosis. Crouzonsyndrome, Apertsyndrome, Pfeiffer syndrome and Saethre-Chotzensyndrome are relatively common in syndromiccraniosynostosis [6].
Craniosynostosis was first treated surgically in the late 1800s, using techniques such as fragmentation of the cranial vault and linear craniectomies. These early procedures were associated with high rates of reossification and poor esthetic outcomes, mandating many subsequent procedures. At present, however, simple craniectomy is used only in patients with transient cranial decompression. These early procedures have been supplanted by surgical remodeling of the affected area of the cranial vault and orbits. Surgery is generally performed at age 6–9 months to take full advantage of the regenerative capacity of the skull at this age [7].
Piezosurgery is mainly used in oral surgery; however, it has been used for osteotomies in cranial vault and orbital walls with minimal undermining of the dura mater and periorbital soft tissue, reducing the postoperative swelling. In particular, it is adequate in the case of osteotomies involving thin bone (eg, infant skull) [8].
Piezoelectric device has shown being a valid instrument for bone cutting in accurate procedures, because it allows performing a more precise and safer cutting, without the risk of harming surrounding tissues [9].
The goal of this study was to evaluate the effectiveness of the use of Piezosurgery on a syndromic patient of 11 months who underwent surgical treatment of CS.
CASE PRESENTATION
A 11- months old, female infant, attended accompanied by her parents to the Department of Maxillofacial Surgery headed by Dr Luiz Fernando Lobo, which serves a population that has medical private agreements, with coverage in the city of Sao Paulo. The parents said that her child was diagnosted with Craniosynostosis plagiocephalus (Crouzon Syndrome). Clinical examination revealed frontal recoil, more predominant in the supraorbital region, asymmetry of the skull and face, presenting a rise of the orbit on the affected side, and a frontal bulging contralateral to the compromised suture (Figure 1).

Figure 1 Asymmetry of the skull and face, preoperative.
Three-dimensional computed tomography was performed and it was decided to perform surgical treatment with the neurosurgery and maxillofacial surgery teams (Figure 2).
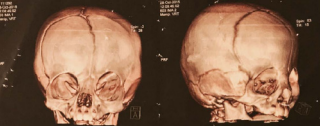
Figure 2 Three-dimensional computed tomography.
The parents were informed about the cosmetic aspect of the surgery and the progressive deformations and their informed consent was obtained.
Surgery was performed with the patient in a supine position. The coronal access was marked with a pen for skin marking (Codman®) and infiltrative anesthesia was performed with ropivacaine 7.5% on the subgaleal surface (Figures 3,4).

Figure 3 Preparation for locating the coronal incision.

Figure 4 Demarcation of coronal access and infiltrative anesthesia with ropivacaine 7.5%.
A coronal incision was made and the scalp was dissected (Figure 5).
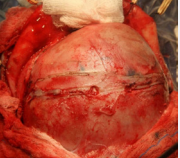
Figure 5 Coronal Access.
The dissection plane was extended subperiosteally to expose the frontal bone, the superior part of the orbit, the coronal suture, and the temporal fossa behind the zygomatic process. The coronal osteotomy with use of the piezoelectric surgical devices (Piezosurgery®- MECTRON, Italy) (Figures 6,7)
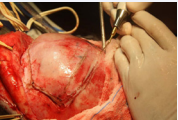
Figure 6 Osteotomy with use of the piezoelectric surgical devices (Piezosurgery®- MECTRON, Italy).
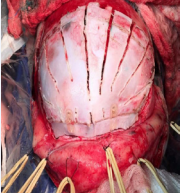
Figure 7 Osteotomy with use of the piezoelectric surgical devices (Piezosurgery®- MECTRON, Italy).
for the forward orbital advancement was realizaded to release of intracranial pressure (Figure 8).

Figure 8 Frontalorbital advancement to release of intra-cranial pressure
The osteotomies were fixated with resorbable fixation system (Lactosorb®- BIOMET, USA) (Figures 9-11).
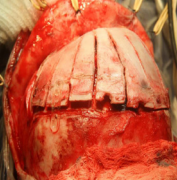
Figure 9 Osteotomy fixation with resorbable fixation system (Lactosorb®- BIOMET, USA).

Figure 10 Osteotomy fixation with resorbable fixation system (Lactosorb®- BIOMET, USA).
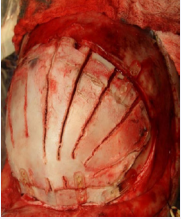
Figure 11 Osteotomy fixation with resorbable fixation system (Lactosorb®- BIOMET, USA.
The procedure occurred without intercurrences.
The patient presented on the first day of the postoperative, a satisfactory response, with minimal edema and absence of hematoma (Figure 12).

Figure 12 First day of the postoperative, a satisfactory response, with minimal edema and absence of hematoma.
She remained hospitalized for 5 days, evolving with clinical and physical improvement (Figure 13).

Figure 13 Fifth postoperative day evolving with clinical and physical improvement.
DISCUSSION
Craniosynostosis is a congenital anomaly of cranial deformity and stenosis due to early fusion of the cranial sutures. The classification probably more used, based on the compromised suture (the one that closed early), and may present 4 main types: escafocephaly or dolicocephaly (early closure of the sagittal suture), trigonocephaly (early closure of the metopic suture), plagiocephaly Brachycephaly or turricephaly (early closure of the coronal and / or lambdoid sutures). These cranial deformities, when left untreated, can bring psychological damage to these children, causing them to avoid social interaction due to their unusual appearance [4].
The sagittal suture (40–55%) is the most commonly affected, followed by the coronal (20–25%) [3]. Neurocognitive impairments have been reported in 35–50% of school-aged children with isolated single suture craniosynostosis [10].
The treatment is usually surgical, and has as main scope to correct the cranial distortion and prevent progression and craniofacial deformity, preventing any future impairment and an increase in intracranial pressure (ICP). Intraoperative bleeding is the main complication. In addition to trained neurosurgical staff, a multidisciplinary team is enabled to manage these children, and intraoperative bleeding in cases of cranial reconstruction is the main complication [11].
Frontoorbital advancement has become a standard method both to increase intracranial volume and to improve facial appearance in patients with syndromal or nonsyndromal craniosynostosis. Relevant complications of this procedure include severe hemorrhage and trauma to intracranial, orbital, or facial soft tissues, which mostly arise during the process of bone exposure or osteotomy [12]. The piezoelectric device in the present study showed an easy handling with a reduced amount of trauma, being an instrument indicated in osteotomies because it allowed a safe cut without damaging the adjacent tissues.
Furthermore, with piezoelectric surgery, it has been possible to perform precise osteotomy in close proximity of vessels, nerves, and other important structures, such as dura mater, with minimal bleeding. To minimize the risk of soft tissue injury and to increase the precision of the osteotomy, the authors applied a piezoelectric osteotomy for frontoorbital advancement in 15 patients with craniosynostosis seen consecutively (mean age 11.3 months), they demonstrated that this new device can cut cranial bones using ultrasonic micro vibrations created by piezoelectric effects [12].
The surgical treatment of CS with the use of the piezo surgery has proved to be effective, because it allows a precise osteotomy, minimal bleeding and without injury to adjacent tissues. The patient evolved without complications, with minimal edema and a shorter hospital stay.
REFERENCES
1. Renier D, Arnaud E, Marchac D. Craniostenoses: Introduction. Neurochirurgie. 2006; 52:149-150.
4. Renier D, Arnaud E, Marchac D. Classification des craniostenoses. Neurochirurgie. 2006; 52: 200-227.
11. Tude Melo JR. Atualizaçãoemneurocirurgiapediátrica. Rev Bras NeurolPsiquiatr. 2014; 18: 110-112.









































































































































{kind=link}