Overweight and Obesity in Pacific: A Systematic Review Study on Dietary Patterns of Pacific People
- 1. Department of Health Promotion, Fiji National University, Fiji
- 2. Department of Clinical Nutrition, Northern Borders University, Saudi Arabia
- 3. Department of Public health, Fiji National University, Fiji
Abstract
Introduction and aim: There are many adverse health effects that can arise from poor dietary habits or patterns such as overweight and obesity. Pacific countries are encountered with high prevalence of overweight and obesity while there has never been any study to consider the role of dietary patterns on it. This systematic review study is conducted to assess the available literature in regards to dietary patterns in the Pacific and determine the health impacts and factors contributing towards overweight and obesity.
Methods: Based on Cochrane library guideline of conducting systematic review, 6 most frequent used databases were searched using relevant key words to find the studies. All studies such as quantitative, qualitative and mixed methods were included in the search. Moreover studies used in this exercise were published between the 1st of January 2000 and the 1st of January 2017 in the English language was included in the search. Two independent coders reviewed were reviewed and finally the full text of the remaining studies were read to find relevant studies. A data extraction sheet was developed and the data were analyzed using descriptive analysis.
Results: Sixteen studies were analyzed and the South Pacific accounted for the most studies with 75% and most of the studies focused on individuals aged \20 and over (56%).The prevalence of overweight is ranged between 14.7% to 50.5%. And obesity prevalence is ranged between 6.1% to 73.9%.Consuming \sweet beverages was the most frequently reported dietary pattern (31.25%) which is followed by meals or breakfast skipping (25%).
Conclusion: The results of this study highlighted the role of dietary patterns in prevalence of overweight and obesity in Pacific countries. Promoting healthy policy along with developing interventional studies to change people health behavior are strategies which policy makers and health care decision makers
Keywords
Overweight; Obesity; Dietary patterns; Pacific
Citation
Mohammadnezhad M, Alqahtani NS, Salusalu MV, Konrote A (2017) Overweight and Obesity in Pacific: A Systematic Review Study on Dietary Patterns of Pacific People. JSM Health Educ Prim Health Care 2(2): 1031.
INTRODUCTION
Dietary patterns play an important part in the life of an individual and can have a large impact on their health and wellbeing [1]. Dietary requirements may vary from person to person depending on age, gender, lifestyle and degree of daily physical activity [1]. However, according to the World Health Organization (WHO) the principals of what constitute a healthy diet remain the same.
Despite the implementation of dietary recommendations millions continue to suffer from dietary related illness. Globally, 16 million Disability Adjusted Life Years (DALYs) and 1.7 million deaths are attributed to low fruit and vegetable consumption every year [2]. It is estimated that one in three persons is malnourished which is linked to a total of 3 million child deaths each year [3]. It was also determined by the Food and Agriculture Organization (FAO) that an estimated 2 billion people suffer from macronutrient deficiencies which is due to a low intake of macronutrients found in fresh meat, fruits and vegetables [4].
However a majority of these nutrient deficiencies are found to be prevalent in low to middle income countries [5]. FAO determined that 60% of the global caloric intake is met by rice, maize and wheat which are considered staples throughout the world, however this does not ensure that all nutrient requirements are satisfied [4].
Pacific countries are mostly characterized by geographical isolation, low income, limited natural resources, lack of sufficient managerial and technical expertise, as well as inappropriate management systems which can affect the prevalence of overweight and obesity. Moreover, Pacific people have similar socioeconomic indicators such as occupation, education and income [6]. Their traditional foods such as fresh fish, meat, and local fruits and vegetables have been substituted by rice, sugar, flour, canned meats, canned fruits and vegetables, soft drinks and beer [7]. Nowadays, majority of Pacific countries have come to depend on food imported from other countries so that they are encountering with lots of high-fat, energy-dense foods. As a result, purchasing these imported foods has reduced the importance of traditional foods among Pacific population [8]. In a report released by the WHO in 2010 it was found that as a result of abandoning traditional diets, Pacific islanders were becoming more susceptible to Non Communicable Disease (NCDs) and macronutrient deficiencies [8]. These diseases are on the rise due to Pacific islanders opting towards imported and processed foods rather than the fresh local grown goods which they are commonly known for including root crops (Taro, Cassava), fish, leafy greens and an array of seafood[8]. The same report released by the WHO found that 15 out of 16 countries observed had at least one fifth of their pregnant women and child population suffering from anemia. Anemia (Iron deficiency)and similar deficiencies are major problem in the Pacific due to the low consumption of fruits and vegetables by Pacific islanders [8]. This is backed by the report which found that only 20% of the surveyed population acknowledged that they consumed the required five servings of fruits and vegetables daily [8]. In addition to this Pacific islanders have been found to have high numbers of overweight and obese individuals as a result of poor diet and over consumption. This has been found to affect an estimated 50% to 90% of the populations of some island countries [8].
With the importance of diet in mind there are many health effects that can arise from poor dietary habits or patterns. These include chronic diseases such as cardiovascular disease, cancer, overweight and diabetes[9]. In addition to NCDs poor dietary habits can lead to macronutrient deficiencies such as anemia, goiter, scurvy, and even osteomalacia. Another listed effect of under nutrition is that it increases the risk of death from common infections and increases their frequency and severity. Also it has been found that in children and infants, malnutrition can hinder growth, increase the risk of infection and impair cognitive ability [3].
Therefore it can be concluded that there is a need for research in relation to dietary patterns and nutrition in order to combat its effects not only in the Pacific but around the globe. Hence this systematic review is designed to assess the available literature in regards to dietary patterns in the Pacific and determine the health impacts and factors contributing towards it.
METHODS
This systematic review was conducted based on the Cochrane library guidelines. Eight data bases which were frequently used by other similar studies have been chosen to search the studies. They included Medline, PubMed, Web of Science, PsycInfo, CINAHL, Scopus, EMBASE and Google Scholar databases. The key terms used to search these databases included ‘obesity’, ‘‘overweight’, “dietary pattern*” OR “eating pattern*” OR “food* pattern*” OR “dietary habit*” OR diet OR “dietary”) AND (“factor” OR ”contributor”) AND Pacific. The search covered all the studies conducted in the Pacific without considering their region. All studies such as quantitative, qualitative and mixed methods were included in the search. Moreover studies were published between the 1st of January 2000 and the 1st of January 2017 in the English language were included in the search while studies with other languages and among non-Pacific countries were excluded.
Three steps were conducted to achieve the relevant studies after duplicated studies from selected databases had been removed Figure 1. At the first stage the title of all found studies were scanned by two independent researchers and all studies deemed irrelevant by the exclusion criteria were omitted. The remaining studies moved on to the second step were the abstracts were reviewed and all studies deemed irrelevant were again removed. Finally the full texts of the remaining studies were reviewed and those studies that met the inclusion criteria were chosen for further analysis (13 studies). The bibliography of the remaining studies was searched to include 3 additional studies that were not found within the searched databases Figure 1.
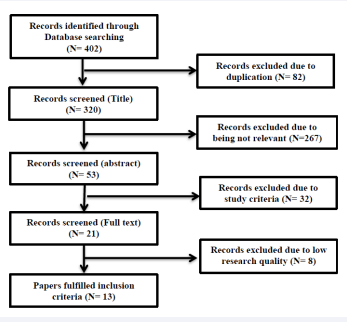
Figure 1: Article Selection Process.
A data extraction sheet was developed including four sections such as study information, compilation, methodology and results with relevant information being included in the sections. A descriptive analysis was used to analyse the data and the results were reported as percentages using tables and graphs.
RESULTS
Overall, 16 studies were analyzed. As Table 1 shows majority of the studies were conducted after 2010 (87.5%). The south Pacific accounted for the most studies with 75% and most of the studies focused on individuals aged 20 and over (56%). More than half of the studies (56%) were quantitative and 38% were mixed method design. In terms of place of study community based studies made up 56% of the studies while school based studies only made up 43.75% Table 1.
Among South Pacific countries, New Zealand had the highest number of studies (6 studies) which followed by Fiji, Vanuatu, Tonga (3 studies each) Samoa and Solomon Islands (2 studies each). Hawaii was the country in American Pacific which includes 4 studies. American Samoa and Northern Mariana had only one study.
All of the studies were quantitative study and in total 48064 total participants were engaged with these studies. 14 studies engaged both male and female participants and 2 studies engaged only female participants in the study.
Table 1: General characteristic of the studies.
| Factors | Frequency | Percentage |
|
Year of the studies 2000-2004 2005-2009 ≥ 2010 |
0 2 14 |
0 12.5 87.5 |
|
Region South Pacific American Pacific |
12 4 |
75 25 |
|
Age group Less than 10 11-20 years 0ver 20 years old Not reported |
2 4 9 1 |
13 25 56 6 |
|
Study design Quantitative Qualitative Mixed Method |
9 1 6 |
56 6 38 |
|
Place of the study Community based School based |
9 7 |
56.25 43.75 |
Table 2: Frequency dietary patterns in Pacific Islanders.
| Factors | Frequency | Percentage |
| Meal/breakfast skipping | 4 | 25 |
| SSB | 5 | 31.25 |
| Purchased school lunch | 1 | 6.25 |
| Consume less fruit | 1 | 6.25 |
| Carbonate drink | 1 | 6.25 |
| Processed foods | 3 | 18.75 |
| No family meals | 1 | 6.25 |
| Rice or Carbohydrates | 1 | 6.25 |
| Fast food | 1 | 6.25 |
| Meat | 2 | 12.5 |
PREVALENCE OF OVERWEIGHT AND OBESITY DESCRIPTION
From the 16 studies identified, 10 of them (62.5%) reported the prevalence of obesity and overweight. However, overall, the prevalence of overweight is ranged between 14.7% to 50.5%. And obesity prevalence is ranged between 6.1% to 73.9%. The study from Vanuatu conducted among adults reported the highest prevalence of obesity. The lowest prevalence of obesity was reported from the study conducted among adolescents in six Pacific islands in Oceania (Fiji, Kiribati, Samoa, Solomon, Tonga and Vanuatu). Comparing prevalence in terms of Gender, the highest prevalence of obesity reported was among women or female 93.9% and the highest prevalence of obesity for males was 49.5%
Ten dietary factors have been identified in this research. Consuming sweet beverages was the most frequently reported dietary pattern and its role in overweight and obesity was documented five times in five studies (31.25%). Sweet Beverages is followed by meals or breakfast skipping which appeared 4 times in the studies (25%). Consuming of western foods/ processed foods was the third most reported dietary factor with a frequency of three (18.75%); then followed by high intake of meat with a frequency of two (12.5%). All the remaining dietary factors (purchased school lunch, low intake of fruit and vegetables, carbonate drinks, family meals, rice and fast foods high consumption) reported once in the studies. Most importantly, all of these dietary factors identified are positively associated with increase weight and obesity Table 2.
DIETARY PATTERNS BASED ON ETHNICITY
In terms of ethnicity and fruits and vegetable consumption two studies were found with one based in Fiji while the other was conducted in New Zealand. The result showed that 77% indo-Fijian and 69% Indigenous Fijian consumes less fruit and vegetables fall short of the WHO fruit and vegetables consumption requirement. In addition, the study conducted on adolescents dietary pattern in New Zealand reported more than half (50%) of the Pacific islander’s adolescents (specific countries not reported) consume less fruit and vegetables.
Breakfast and lunch skipping were common dietary practices among adolescents Table 3. Overall there were no community based studies focusing of breakfast and meal skipping however four school based studies (25%) reported breakfast and lunch skipping. The prevalence of breakfast skipping is ranged from 23% to 68% among adolescents. Among the sixteen dietary studies, seven community based studies (43.75%) were conducted and the most common dietary patterns reported from those studies, sugar sweetened beverage consumption reported by two studies (13%), the other two studies (13%) reported high meat consumption, and one study (7%) reported high consumption of sugar sweetened beverage and carbonic drinks Table 3.
DISCUSSION
The results of this study highlighted high prevalence of overweight and obesity in Pacific countries. Environmental factors play main role in the rapid increase of population obesity rather than physical factors like evolutionary genetic changes. Sociocultural changes due to immigration, westernization and acculturation can affect people overweight and obesity status [10]. For example in a study conducted by Lassetter (2011), native Hawaiian people who migrated to Las Vegas were believed that food played an important role in well-being and to support cultural connectedness; migrants were encouraged to expend calories [11].
However there was difference in age group of participants were reviewed in this study, in Pacific countries due to traditional Pacific cultural milieu, values about food and diet and body image of children may be influenced by the parents and adults [12]. The present demographical features of Pacific peoples such as high fertility, fast intermarriage, a high population growth rate, and a young population designate that there are potential risks for the future [13].
Through the duration of this study much insight into the dietary patterns of Pacific islanders has been brought to light. The first major dietary finding of this study was that of sweet sugary beverage consumption. Out of the sixteen articles reviewed in this study a total of 5 made reference to a high consumption of sweet sugary beverages Table 4. Consumption of these beverages has been linked to CVD, high cholesterol, weight gain and Type 2 Diabetes [14]. In a study by Ebling CB et al. (2006), it was found that by reducing the consumption of sweet sugary beverages beneficial effects can be seen on body weight [15]. These studies provide evidence that there is indeed a risk on the health of Pacific islanders if they continue to consume SSBs in high quantities.
Moreover the second most prominent dietary trend found by this study was that of meal skipping. According to research meal skipping has been associated with CVD, increased prevalence of obesity and has even been found to affect appetite [16]. In a study conducted in Australia it was found that meal skippers tend to snack more than individuals who eat three meals a day [17]. In addition to this a similar study also found that despite the frequent snacking individuals who skipped meals had a lower overall nutrient intake than those who ate three full meals a day. The study also went on to state that meal skipping was more common among smokers, females, lesser educated individuals and individuals with lower self-rated quality of wellbeing[18].
n a study set out by J Vanden Bulck and S Eggermont (2006) attempting to establish reasons behind meal skipping in secondary school students a positive association was made between high media usage and meal skipping[19]. The study found that a high usage of media often resulted in meal times being sacrificed. In a similar study by Tasileta Teevale et al. (2010), it was found that another reason common among parents relating to meal skipping was lack of time [20]. With the rapid modernization of the Pacific islands issues such as meal skipping will continue to rise if not kept in check. Hence more needs to be done to spread the word about the health implications of meal skipping.
The next dietary pattern found to be common among Pacific islanders by this study was the high intake of imported and processed foods. Pacific islands are known around the world for the availability of fresh and nutritious fruits, vegetables and in certain countries dairy and livestock. However due to modernization and trade links to outside countries, the importation of canned and processed goods is currently on the rise [8]. In the Pacific consumption of foods such as tinned fish and tinned meats are a common occurrence along with instant foods such as noodles [21]. According to a study by Kelsey Dancause et al. (2013), tinned fish is likely to have a much higher fat content than fresh fish which can have negative impacts on the health of an individual [21]. However the public continues to consume processed and nutritionally lacking goods [8].
In a bulletin report released by WHO it was stated that a major issue regarding diet was the high consumption of imported foods from countries such as China, Malaysia and the Philippines [8]. In addition to this it was found that the nutrition labels of these imported goods are often inconsistent and at times not even in English [8]. This can lead to confusion and even prevent the public from assessing the nutritional quality of the foods being consumed. In order to combat this, a study by Anne Marie Thow et al. (2011), concluded that by promoting healthier imports and reverting back to traditional foods the potential would be present to improve diets and health [22]. Hence more needs to be done to encourage local consumption and reduced intake of processed and imported foods.
In addition to this the next most prevalent dietary trend was high meat and animal protein consumption. A study conducted in Vanuatu to assess the behavioural risk factors of obesity in relation to health transition concluded that the population’s reliance on red meat is significant enough to contribute to an increased risk of obesity [21]. In addition to this a similar study which investigated the frequency of meat consumption in Koreans and found that an increased frequency was positively associated with Colorectal Cancer [23]. This is further backed by another study conducted by An Pan et al. 2012, [24].This is evident as meat consumption is a common event in the Pacific with a majority of the meats being provided through imports [25]. Therefore more needs to be done in order to spread awareness on the effects of over consuming meat.
Aside from the factors mentioned above the following dietary trends were also observed, low fruit and vegetable intake, fast food consumption, high rice intake, and the frequent purchasing of schooled lunches. In terms of fruit consumption the Pacific is a hub for fresh produce however consumption of said fruits is constantly decreasing not just in the Pacific but world-wide [25]. In a study conducted by Karen Lock and her team it was found that by increasing fruit and vegetable consumption the risks of NCDs could be reduced greatly [26]. Similarly a study published by the International Journal of Obesity found that fruit consumption can be linked to reduced risks of obesity and weight gain which backs up the conclusions of the article by Karen Lock [27].
Dietary patterns are present in everyday life and a key factor is that they are indeed modifiable. In order to protect the people of the Pacific from dietary related illness, work needs to be done both on the ground level and on that of the policy level [22]. Countries such as Fiji have taken the first steps towards achieving this by banning the entry of foods deemed unhealthy into the country. In the case of Fiji the importation of mutton flaps from Pacific neighbour New Zealand were banned in an attempt to prevent the consumption of the fatty meat. However after the 2000 coup the ban was lifted and importation is now legal again [28]. Therefore the governments and relevant authorities need to ensure that the policies put in place are enforced strictly to ensure the safety and health of the public.
The strengths of this study include the range of studies from the year 2000 to the year 2017 however there were some limitations to the study. The first limitation was the exclusion of article written in languages other than English which limited the scope of the study and the second limitation was the omission of grey literature.
In conclusion, the high prevalence of overweigh and obesity is alarming that the health care providers and policy makers need to consider it as the health priority. Knowing the fact that the Pacific countries exporting their healthy foods and products such as fish and fruits to other countries and also importing the cheap foods along with difficulty is buying healthy foods for majority of the population increase the risk of overweight and obesity. Promoting healthy policy along with developing interventional studies to change people health behaviour are strategies which policy makers and health care decision makers need to consider.
At the end of this study the available literature was able to provide a glimpse into the dietary patterns and habits of the people of the Pacific islands. Considering the results of this study and dietary patterns of Pacific people, developing public health strategies to address health risk conditions such as obesity is very important. Pacific Island countries need to implement innovative policy interventions in both health and outside of health sectors. Their high rates of overweight and obesity make them likely settings for further policy-based actions in the global level. It is essential to develop preventive strategies for health issues such as obesity which involve collaborations among the peoples, the communities and the governments they represent and also international health organizations. Strategies need to focus on modifying human behaviour, promoting health systems, educating the stakeholders and changing the policies for the aim of meaningfully improving the well-being of Pacific Islanders and their future generations. It is notable that more research needs to be conducted regarding the dietary patterns and habits of Pacific islanders as they are currently at risk of diet related illness.
Table 3: Distribution of school based studies based on breakfast and meal skipping.
| School-based | Breakfast skipping | Lunch skipping |
| 1 | 68% | - |
| 1 | - | 40% |
| 1 | 23% | - |
| 1 | 45.4% | 55.6% |
Table 4: Data extraction sheet- Dietary Descriptive studies.
| Article | Participants | Methods | Results | |
| 1 |
Wate et al., [29] Year: 2013 Country: Fiji Type of Study: Descriptive study |
Number: 6,871 Gender: Male 3395 Female 3476 Age: 12-17 years |
Sampling. -Purposive sampling Data Collection tools. Questionnaires Place: School |
Prevalence -24% overweight or obese -Indigenous Fijian 34% Dietary pattern -Infrequent breakfast & lunch consumers, consumed SSB, low intake fruit & vegetables |
| 2 |
Thompson-McCormick et al., [30] Year: 2010 Country: Fiji Type of Study: Descriptive study |
Number: 523 Gender: Female Age: 15–20 years |
Sampling. -Purposive sampling Data collection tool. Questionnaires Place: Schools |
Prevalence -40.7% overweight, 14.7% obese Dietary pattern - breakfast skipping - skipping breakfast |
| 3 |
Teevale et al., [31] Year: 2012 Country: NZ Type of Study: Descriptive study |
Number: 4284 Gender: Male 2116 Female 2168 Age: 12 and 17 years |
Sampling. -Purposive sampling Data collection tools. Questionnaires and interview Place: School |
Prevalence -31% obese , 36% overweight Dietary pattern -purchased lunches; |
| 4 |
Grant et al., [32] Year:2004 Country: NZ Type of Study: Descriptive study |
Number: 60 Age 2-5 years Gender: Male, Female |
Sampling -Purposive sampling Data collection tools Interview & questionnaires Place: School |
Prevalence obese 64%-75%, overweight 45%-60% Dietary pattern -Sugar intake excess WHO standard |
| 5 |
Utteret al., [33] Year:2006 Country:NZ Type of study: Descriptive study |
Number: 2989 students Age: 5-14 years Gender: Male 1504 Female: 1485 |
Sampling -Purposive sampling Data collection tools Questionnaires, interviews, Place: School |
Dietary pattern 40% Pacific, 23% Mäori students skipped breakfast -High takeaway consumption - low fruit, vegetable intake. Physical activity -children do more active game |
| 5 |
Utteret al., [33] Year:2006 Country:NZ Type of study: Descriptive study |
Number: 2989 students Age: 5-14 years Gender: Male 1504 Female: 1485 |
Sampling -Purposive sampling Data collection tools Questionnaires, interviews, Place: School |
Dietary pattern 40% Pacific, 23% Mäori students skipped breakfast -High takeaway consumption - low fruit, vegetable intake. Physical activity -children do more active game |
| 6 |
Teevale et al., [20] Year: 2010 Country: New Zealand Type of Study: Mixed methods study |
Number: 1586 students Gender: Male, 789 female 807 Age: 12-17 years |
Sampling. -Purposive sampling Data collection tool. Questionnaires, interviews Place: High schools |
Prevalence Obesity-49.4 boys, 50.6% girls, Overweight-49.5 boys, 50.5% girls Dietary pattern Breakfast and lunch skipping Physical activity: obese children less active |
| 7 |
Pengpid and Peltzer [34] Year:2015 Country: South Pacific islands Type of Study: Descriptive study |
Number: 10,238 Age:13–16 years Gender Male 4566 Female 5672 |
Sampling -Purposive Data collection tools. Questionnaires &interview Place: School |
Prevalence overweight 24.3% obesity 6.1% Dietary pattern consumed carbonated soft drink, fast foods, Low fruit and vegetable, physically inactive |
| 8 |
Dancause et al., [21] Year: 2013 Country: Vanuatu Type of Study: Descriptive |
Number: 534 Gender: Male, 282 Female 252 Age: 18 years and above |
Sampling. -Purposive sampling Data collection -Questionnaire & interview Place: Community |
Prevalence -obesity 73.9% female 22.5% male Dietary pattern -Heavier reliance on animal protein, -Western processed foods (tinned fish and instant noodles) |
| 9 |
Utter et al., [35] Year:2013 Type of Study: Descriptive Country: NZ |
Number: 8734 Age: 13-17 Gender: Male 4691 Female 4043 |
Sampling -Purposive sampling Data collection tools Questionnaires Place: High schools |
Dietary pattern -frequent family meals high fruits and vegetables intake. |
| 10 | Smith et al., [36] Year:2007 Country: Tonga Type of study: Descriptive study |
Number: 443 school students Age: aged 11–16 years Gender: Male, 199 Female 244 |
Sampling -Purposive sampling Data collection tools questionnaire Place: School |
Prevalence Overweight or obese 36.0% of boys, 53.8% girls Dietary pattern eat Tinned mutton or beef , not eat taro physical activity - active, watched television |
| 11 |
Novotny et al., [37] Year:2009 Country: US Type of study: Cross sectional study |
Number: 4,530 hotel workers from 30 hotels Age:-18+ years Gender: Male, 1947 Female 2583 |
Sampling -Purposive sampling Data collection tools questionnaires Place: Community |
Prevalence -57% overweight -Greater acculturation result in greater BMI Dietary pattern -sweet drinks and meat |
| 12 | Estimé et al., [38] Year:2014 Country: South Pacific islands |
Number: Not reported Age: 18 years and above Gender: Male, female |
Sampling -Purposive sampling Data collection tools -questionnaires Place: Community |
-Expenditure on imported foods Kiribati, Tonga, Solomon Islands and Vanuatu Dietary pattern High imported foods high unhealthy foods |
| 13 |
Sluyter et al., [39] Year:2013 Country: NZ Type of Study: Descriptive study |
Number: N=5714 Age:12-22 years Gender: Male, 2885 Female 2829 |
Sampling -Purposive Data collection tools questionnaires, Place: Community |
Risk factors TV viewing related to fatness Dietary -soft drink consumption related fatness |
| 14 |
Braun et al., [40] Year: 2014 Country: American Pacific Type of study: Descriptive study |
Number: Not reported Age: 2–8 years Gender: Male, Female |
Sampling -Purposive sampling Data collection tools Community meetings, literature review Place: Community |
Prevalence 40% overweight or obese Dietary pattern -engaged children in growing and eating local healthy foods change attitudes and behaviors |
| 15 |
Novotny et al., [41] Country: Hawaii Year:2012 Type of Study: Descriptive |
Number 1612 Age: 18+ years Gender: Male, 774 Female 838 |
Sampling -Purposive Data collection tools questionnaires Place: Community |
Dietary pattern –Acculturation related high intake SSB BMI outcome -no significant change in BMI across intervention |
| 16 |
Braginsky et al., [42] Country: Hawaii Year:2016 Type of Study: Descriptive study |
Number: 6 women Age:39 to 56 years Gender: Female |
Sampling -Purposive study Data collection tools Questionnaires, interviews Place: Community |
Dietary High intake rice, fast food, parties related overweight, obesity |










































































































































{kind=link}