Extraction of a 30-Year-Old Pacemaker Lead Implanted Through the Right Femoral Vein Using a Combination of Sheaths and a Femoral Work Station: A Case Report
- 1. Department of Cardiovascular Surgery, Sanatorio de la Trinidad San Isidro, Buenos Aires, Argentina
- 2. Department of Cardiovascular Surgery, Hospital Italiano de La Plata, Buenos Aires, Argentina
Abstract
Pacemaker lead extraction is a challenging and potentially risky procedure, especially when dealing with leads that have been implanted for a long period of time [1]. In this case report, we present a 45-year-old patient who required the extraction of a 30-year-old pacemaker lead implanted through the right femoral vein. We used a combination of sheaths and a femoral work station to safely extract the lead.
Keywords
• Lead Extraction
• Pocket Infection
• Femoral Approach
CITATION
Mazzetti HA, Rios A, Koladynski D, Marenchino R, Zgrablich C, et al. (2023) Extraction of a 30-Year-Old Pacemaker Lead Implanted Through the Right Femoral Vein Using a Combination of Sheaths and a Femoral Work Station: A Case Report. JSM Heart Surg Case Images 3(1): 1011.
INTRODUCTION
Pacemaker lead extraction is a complex procedure that requires careful planning and execution. The procedure becomes even more challenging when dealing with leads that have been implanted for an extended period of time. In this case report, we present a patient who required the extraction of an old pacemaker lead implanted through the right femoral vein.
CASE REPORT
A 45 year old male with a history congenital Complete AV Block, with a first trans venous pacemaker implant at 7 years old, then a pocket infection with the removal of the pacemaker and lead, remaining the tip. Then a new transvenous implant on the contralateral side, with a new infection and bacterial endocarditis, which need open heart surgery when he was 15 years old [Figure 1].
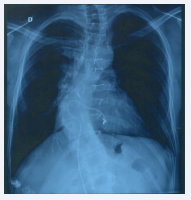
Figure 1: Preoperatory X-ray. Black arrows: abandoned tips.
Through a right femoral approach a pacemaker was implanted 30 years ago. A genograms showed the obstruction of both subclavian veins and the superior vena cava. After a third pacemaker change, he presented with a pocket infection. An echocardiogram showed no vegetation. Positive blood cultures for coagulase negative staphylococcus. After discussion with the patient and his family, it was decided that the lead would need to be extracted [2].
The lead was implanted through the right femoral vein (Unknown model), which posed a challenge for lead extraction. We used a combination of sheaths and a femoral work station to safely extract the lead. A locking style (Spectranetics/Philips) was used to lock the lead in place. We then used a series of sheaths, including metal sheaths (medium) (Cook Medical) to enter into de Femoral and Iliac vein, polypropylene sheaths (10 and 11.5 Fr) (Cook Medical) through the iliac vein, and a Tight Rail (11 Fr) (Spectranetics/Philips) along the inferior vena cava for along 45 cm from the entrance, and then a Byrd Femoral Work Station (Cook Medical) to remove the lead, (Figure 2).

Figure 2: Femoral work station. The sheath entering the right ventricle.
Calcium rings were found along the lead. There was scar tissue all along the lead in the femoral, iliac and the inferior vena cava (Figure 3 Computed tomography).
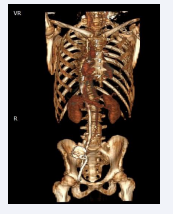
Figure 3: TAC showing scar tissue along the lead.
Tools used, were for the superior approach, and the only sheath that reached the heart was the femoral work station. Sheaths were change due to the tortuosity of veins. The tip was left inside the heart, with a procedure clinical success [Figure 4].

Figure 4: Post-operative X-ray Black arrows: abandoned tips
During the procedure, heart rhythm was maintained with temporary epicedial lead. A dual chamber epicedial pacemaker was implanted in the same procedure, with two screws in bipolar leads, with steroids. Nine months later, uneventful post-operative.
DISCUSSION
The extraction of a pacemaker lead implanted through the right femoral vein is a challenging procedure. In this case, we used a combination of sheaths and a femoral work station to safely extract the lead. The use of a locking style and various sheaths allowed us to navigate the lead through the patient’s venous system and safely remove it.
CONCLUSION
The extraction of a 30-year-old pacemaker lead implanted through the right femoral vein using a combination of sheaths and a femoral work station is a challenging but achievable procedure. Careful planning and execution, along with close monitoring of the patient’s vital signs can lead to a successful outcome.






































































































































