Sinus of Valsalva Aneurysm of the Non-Coronary Cusp with Intraluminal Thrombus: A Multimodality Imaging Case Report
- 1. Assistant professor, Department of Cardiology, Nizam’s Institute of Medical Sciences, Hyderabad, Telangana, India
- 2. Assistant professor, Department of Cardiology, Nizam’s Institute of Medical Sciences, Hyderabad, Telangana, India
- 3. Assistant professor, Department of Cardiology, Nizam’s Institute of Medical Sciences, Hyderabad, Telangana, India
- 4. HOD -Professor, Department of Cardiology, Nizam’s Institute of Medical Sciences, Hyderabad, Telangana, India
Abstract
Sinus of Valsalva Aneurysm (SOVA) is a rare cardiac anomaly that can present incidentally or with life-threatening complications such as rupture or thromboembolism. We report a case of a 49-year-old male evaluated for palpitations, in whom multimodality imaging revealed an aneurysm arising from the non-coronary cusp of the aortic sinus containing an eccentric mural thrombus. Transthoracic Echocardiography (TTE), Transesophageal Echocardiography (TEE), Cardiac Magnetic Resonance Imaging (MRI), and Computed Tomography Coronary Angiography (CTCA) provided complementary diagnostic information. This case highlights the role of multimodality imaging in characterizing sinus of Valsalva aneurysms and guiding individualized management.
INTRODUCTION
Sinus of Valsalva Aneurysm (SOVA) is a rare cardiac anomaly that may be congenital or acquired. It accounts for less than 1% of all congenital cardiac defects [1]. The aneurysm most commonly involves the right coronary sinus, while involvement of the non-coronary sinus is uncommon [2]. SOVAs are often asymptomatic but may present with arrhythmia, heart failure, or complications such as rupture or thromboembolism. We present a case of non-coronary cusp SOVA with mural thrombus identified incidentally through multimodality cardiac imaging.
CASE PRESENTATION
A 49-year-old male presented with complaints of intermittent palpitations for three years, increasing on exertion and associated with sweating. Clinical evaluation revealed atrial fibrillation with a controlled ventricular rate. Baseline echocardiography demonstrated a large mass in the interatrial septum measuring approximately 5.2 × 3.0 cm, suggestive of a cystic lesion with internal septations. Transesophageal Echocardiography (TEE) confirmed a large mass arising near the non-coronary sinus of Valsalva, raising suspicion of aneurysm with internal thrombus. Coronary angiography showed mild coronary artery disease. Cardiac MRI demonstrated an aneurysmal dilatation of the non-coronary cusp of the aortic sinus measuring 4.3 × 3.1 cm with eccentric mural thrombus, causing compression on the left atrium. No myocardial edema, perfusion defect, or late gadolinium enhancement was noted. CT coronary angiography further delineated a saccular aneurysm from the non-coronary sinus measuring 3.8 × 3.8 × 5.6 cm with non-enhancing thrombus, indenting the left atrium and right pulmonary vein. Calcified plaques causing mild luminal narrowing were noted in the left main coronary artery and left anterior descending artery. The total calcium score was 420. The cardiothoracic surgeon had assessed the operative risk to be significantly high in view of the patient’s very low body weight (40 kg), raising concerns regarding perioperative morbidity, hemodynamic instability, and postoperative recovery. These factors were clearly explained, and although surgery was advised, the patient declined the procedure after understanding the associated risks. In view of the high surgical risk and the patient’s informed refusal, we adopted a conservative management strategy. The patient was managed with rate control for atrial fibrillation and remains stable on follow-up (Figures 1-3).
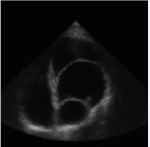
Figure 1 Transthoracic Echocardiography showing large mass occupying the LA.
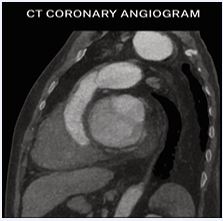
Figure 2 CT Coronary Angiogram depicting saccular aneurysm from non-coronary sinus compressing left atrium and right pulmonary vein with peripheral thrombus.
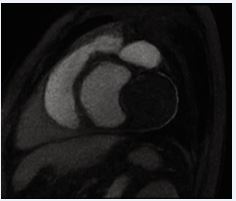
Figure 3 Cardiac MRI demonstrating aneurysmal dilation of non coronary cusp with eccentric thrombus, no myocardial edema, and preserved LV systolic function.
DISCUSSION
Sinus of Valsalva Aneurysms (SOVAs) can be congenital, resulting from deficiency in the elastic and muscular tissues of the aortic wall, or acquired, secondary to trauma, infection, or degenerative aortopathy [3]. Non-coronary cusp involvement, as in our patient, is the least common type and may remain asymptomatic until complications develop [4]. Thrombus formation within the aneurysm is a rare occurrence but carries risk of systemic embolization [5]. Multimodality imaging is crucial for diagnosis: echocardiography defines morphology and hemodynamics, CT angiography delineates anatomic detail and calcification, while MRI assesses tissue composition and thrombus characterization [6]. Management depends on aneurysm size, symptoms, and associated lesions. Surgical repair is recommended for large or symptomatic aneurysms or those with risk of rupture [7]. Our patient, with moderate aneurysm size, mural thrombus, and no rupture or hemodynamic compromise, even though we advised surgery in view of life-threatening complications, patient refused surgery. Hence, he was managed conservatively with imaging follow-up.
CONCLUSION
Non-coronary sinus of Valsalva aneurysm with mural thrombus is an uncommon clinical entity. Multimodality imaging combining echocardiography, CT, and MRI provides comprehensive evaluation for diagnosis, risk assessment, and management planning. Early recognition and appropriate imaging surveillance are essential to prevent catastrophic complications.
AUTHOR CONTRIBUTION AND PATIENT CONSENT
All authors contributed to the conception, drafting, and revision of this manuscript and approved the final version for publication. Informed written consent was obtained from the patient for publication of this case and accompanying images.
REFERENCES
- Feldman DN, Roman MJ. Aneurysms of the sinuses of Valsalva. Cardiol. 2006; 106: 73-81.
- Takach TJ, Reul GJ, Duncan JM, Cooley DA, Livesay JJ, Ott DA, et al. Sinus of Valsalva aneurysm or fistula: management and outcome. Ann Thorac Surg. 1999; 68: 1573-1577.
- Moustafa S, Mookadam F, Cooper L, Adam G, Zehr K, Stulak J, et al. Sinus ofValsalva aneurysms--47 years of a single center experience and systematic overview of published reports. Am J Cardiol. 2007; 99: 1159-1164.
- Weinreich M, Yu PJ, Trost B. Sinus of valsalva aneurysms: review of the literature and an update on management. Clin Cardiol. 2015; 38: 185-189.
- Tandon V, Goel PK, Mehta V. Thrombus formation in unruptured sinus of Valsalva aneurysm: a rare cause of embolic stroke. Indian Heart J. 2023; 75: 76-79.
- Saremi F, Channual S, Gurudevan SV. Imaging of the sinuses of Valsalva: normal anatomy and pathologic entities. Radiographics. 2020; 40: 829-855.
- Zhao B, Zhang H, Hu S. Surgical management of unruptured sinus of Valsalva aneurysm: experience from a tertiary center. Eur J Cardiothorac Surg. 2024; 65: e12-e18.








































































































































