Prenatal Diagnosis and Elective Cesarean Management of a Giant Placental Chorioangioma: A Case Report
- 1. Department of Obstetrics and Gynecology, Vithas Hospital Las Palmas, Atlántico Medio University, Spain
Abstract
Background: Placental chorioangioma is a rare benign vascular tumour. Large lesions can be associated with significant maternal and fetal morbidity. Early prenatal diagnosis is critical for risk stratification and optimized perinatal care.
Case Presentation: We report a case of a giant placental chorioangioma diagnosed at 18 weeks’ gestation in a 33-year-old primigravida. Serial ultrasound and Doppler evaluations showed stable lesion size and normal fetal hemodynamics. At 38 weeks, elective cesarean delivery resulted in the birth of a healthy neonate.
Conclusion: This case highlights the importance of accurate prenatal diagnosis and multidisciplinary management. Conservative surveillance can be effective in the absence of fetal compromise, and elective cesarean delivery represents a safe option for large vascular placental tumours.
Keywords
• Placental chorioangioma
• Prenatal diagnosis
• Doppler ultrasound
• Elective cesarean section
• Fetal surveillance
Citation
De la Torre D, Marrero MAB, Cros EC. (2026) Prenatal Diagnosis and Elective Cesarean Management of a Giant Placental Chorioangioma: A Case Report. JSM Med Case Rep 7(1): 1016.
INTRODUCTION
Placental chorioangioma is the most common benign non-trophoblastic tumour of the placenta, originally described in 1798 [1]. It consists of a vascular hamartoma composed of proliferating capillaries within the placental stroma [2]. The incidence is approximately 0.5–1% in histopathological series, but clinically significant lesions are rare [2,3]. Lesions smaller than 5 cm are typically asymptomatic. However, giant chorioangiomas (≥5 cm) may act as arteriovenous shunts and lead to high-output cardiac failure, hydrops fetalis, polyhydramnios, fetal anaemia, and preterm delivery [4,5]. Advances in high resolution ultrasound and Doppler imaging have facilitated early prenatal diagnosis and enhanced fetal surveillance. We present a case of a giant placental chorioangioma managed conservatively until term with a favourable outcome.
CASE PRESENTATION
A 33-year-old primigravida was referred to our maternal–fetal medicine unit at 18 weeks’ gestation due to a suspected placental mass. The pregnancy had been uncomplicated, with no relevant medical or obstetric history. Ultrasound examination revealed a well-defined, hypoechoic, vascular placental mass measuring 5.9 × 6.5 cm, located near the umbilical cord insertion on the fetal surface (Figure 1).
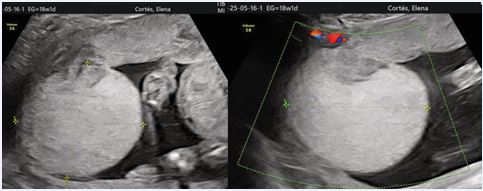
Figure 1: Prenatal ultrasound image demonstrating a well-defined, hypoechoic placental mass located on the fetal surface near the umbilical cord insertion. Colour Doppler imaging shows abundant low-resistance arterial blood flow within the lesion, consistent with a giant placental chorioangioma.
Colour Doppler imaging demonstrated abundant low-resistance arterial flow, consistent with a diagnosis of placental chorioangioma. Fetal biometry, Doppler studies—including middle cerebral artery peak systolic velocity (MCA-PSV)—and amniotic fluid volume were within normal limits. Serial ultrasound examinations were performed every two weeks. The lesion remained stable in size, and no evidence of fetal anaemia, hydrops fetalis, or growth restriction was observed. Maternal condition remained stable throughout pregnancy. At 38 weeks’ gestation, an elective cesarean section was performed due to breech presentation and the vascular nature of the tumour, with concern for potential intrapartum complications. A healthy female neonate weighing 3070 g was delivered, with Apgar scores of 9 and 10 at 1 and 5 minutes, respectively. Gross examination of the placenta revealed an 8.0 × 6.8 cm vascular mass on the fetal surface (Figure 2).
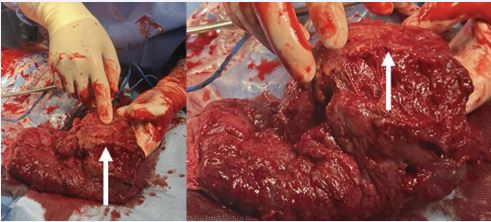
Figure 2: Gross and histopathological findings of the placental chorioangioma. Macroscopic examination reveals a large, well-circumscribed vascular mass on the fetal surface of the placenta. Histological analysis shows numerous capillary-sized vessels lined by benign endothelial cells within the placental stroma, confirming the diagnosis of placental chorioangioma.
Histopathological analysis demonstrated numerous capillary-sized vessels lined by benign endothelial cells, confirming the diagnosis of placental chorioangioma. Postoperative recovery was uneventful, and both mother and infant were discharged on the third postpartum day.
DISCUSSION
Placental chorioangioma represents a benign vascular malformation rather than a true neoplasm [2]. Lesion size and vascularity largely determine clinical impact. While small chorioangiomas are usually asymptomatic, giant lesions can act as arteriovenous shunts, diverting significant fetal cardiac output and predisposing to complications such as fetal anaemia, hydrops fetalis, and high-output cardiac failure [3-6].
Large chorioangiomas can cause fetal and maternal complications via several mechanisms:
- Arteriovenous shunting, increasing cardiac preload and leading to high-output cardiac failure.
- Sequestration of red cells and platelets within the tumour, contributing to anaemia and thrombocytopenia.
- Increased transudation across the tumour surface, producing polyhydramnios.
- Altered placental perfusion leading to placental insufficiency and growth restriction [4,5].
Maternal complications, including preeclampsia and preterm labour, justify close monitoring. Prenatal ultrasound and Doppler are the main diagnostic tools. Typical findings include a hypoechoic mass with internal vascularity, often near the cord insertion. Differential diagnoses include placental teratoma, intervillous thrombus, subchorionic hematoma, and partial hydatidiform mole [7]. Management depends on lesion size, vascularity, and fetal condition. Expectant management with close monitoring is appropriate for stable cases [4]. Interventional options such as fetoscopic laser coagulation, embolization, intrauterine transfusion, or amnioreduction may be considered in complicated cases [8,9]. In our case, conservative surveillance was appropriate due to stable fetal parameters. Elective cesarean delivery was selected to reduce risks associated with labour in the presence of a large vascular tumour [10]. The mode of delivery is individualized based on tumour characteristics and fetal condition. Cesarean delivery is recommended for large vascular lesions, particularly near the umbilical cord insertion, to minimize intrapartum haemorrhage and cord compression [5]. With timely diagnosis and management, outcomes are favourable.
CONCLUSION
Prenatal detection of placental chorioangioma through detailed ultrasound and Doppler evaluation is essential for risk stratification. Conservative management can be successful in the absence of fetal compromise. Elective cesarean section is a safe delivery route for large vascular lesions. This case highlights the value of multidisciplinary care in rare placental tumours.
REFERENCES
- Fox H. Pathology of the placenta. Clin Obstet Gynaecol. 1986; 13: 501-519.
- Guschmann M, Henrich W, Entezami M, Dudenhausen JW. Chorioangioma--new insights into a well-known problem. I. Results of a clinical and morphological study of 136 cases. J Perinat Med. 2003; 31:163-169.
- Jauniaux E, Ogle R, Burton GJ. Pathophysiology of vascular changes in chorioangioma of the placenta. Placenta. 2018; 69: 63-70.
- Zalel Y, Weisz B, Gamzu R, Schiff E, Shalmon B, Achiron R. Chorioangiomas of the placenta: sonographic and Doppler flow characteristics. J Ultrasound Med. 2002; 21: 909-913.
- Tawa N, Kusanovic JP, Romero R. Giant placental chorioangioma: prenatal diagnosis, complications, and management. Obstet Gynecol Clin North Am. 2017; 44: 93-108.
- Wong HS, Cheung YK, Sin WC. Prenatal diagnosis and outcome of placental chorioangioma. Ultrasound Obstet Gynecol. 2013; 42: 420-426.
- Sepulveda W, Alcalde JL, Schnapp C, Bravo M. Perinatal outcome after prenatal diagnosis of placental chorioangioma. Obstet Gynecol. 2003; 102: 1028-1033.
- Quintero RA, Reich H, Romero R, Johnson MP, Gonçalves L, Evans MI. In utero endoscopic devascularization of a large chorioangioma. Ultrasound Obstet Gynecol. 1996; 8: 48-52.
- Tanaka M, Ichizuka K, Matsuoka R. Successful intrauterine treatment of fetal anaemia due to placental chorioangioma. Prenat Diagn. 2001; 21: 794-797.
- Wong HS, Cheung YK, Sin WC. Prenatal diagnosis and outcome of placental chorioangioma. Ultrasound Obstet Gynecol. 2013; 42:420- 426.








































































































































