Insights into the Contemporary Neurosurgical Trainee: Personality Typing of Residents across the United States
- 1. Department of Neurosciences, Division of Neurosurgery, Medical University of South Carolina, Charleston SC
- 2. Department of Neurological Surgery, Cleveland Clinic, Cleveland OH
- 3. Department of Neurosurgery, University of Pennsylvania, Philadelphia, PA
ABSTRACT
Introduction: The purpose of this study was to investigate patterns of personality typing of current neurosurgical residents training in the United States.
Methods: Data was gathered on a volunteer basis through an online data collection website regarding Myers-Briggs personality instrument (MBPI) typing of present neurosurgical trainees.
Results: Data was obtained from one hundred and eight neurosurgery residents. Residents reported a slight preference for extraversion over introversion, although this was neither statistically significant nor different from the general population. However, compared to the general population, residents demonstrated a strong preference for gathering data from intuition (N) over sensing (S) (64.8% vs. 23.6%; p=0.02), thinking (T) over feeling (F) to guide the decision making process (75% vs. 40.4%; p <0.001), and a judging (J) rather than perceiving (P) lifestyle (94.4% vs. 54.3%; p<0.001). The three most common types among all respondents were INTJ (‘scientist’), ENTJ (‘executive’) and ISTJ (‘duty fulfiller’).
Conclusions: We have provided insights from contemporary neurosurgical residents by compiling MBPI responses across training programs. A strong preference for intuition, thinking and judging functions is apparent. This combination of preferences (NTJ) distinguishes neurosurgical residents from any other medical group that has been described in the literature.
KEYWORDS
Contemporary ; Neurosurgical,
CITATION
Spiotta AM, Mullin J, Weil RJ, Schlenk R, Sean GM, et al. (2014) Insights into the Contemporary Neurosurgical Trainee: Personality Typing of Residents across the United States. JSM Neurosurg Spine 2(3): 1022.
INTRODUCTION
The care of the neurosurgical patient can be challenging and presents a unique set of technical and cognitive demands on the neurosurgical trainee. Emergencies in neurosurgery create an unpredictable environment and daily schedule for the surgeon, including the neurosurgery resident. The field of neurosurgery requires a high degree of technical skills and neurosurgery residents routinely encounter critically ill patients and must evaluate them expeditiously to arrive at an intervention that could be life-saving. Thus, neurosurgical residents must be technically adept, decisive, organized, efficient, tough minded and conscientious individuals who are content with, at times, placing the needs of patients above self and family obligations. They must perform well under stress and be comfortable with making difficult life-or-death decisions. Finally, they must be confident regarding the decisions they make and regarding the procedures they perform.
The purpose of this study is to attempt to more accurately define the contemporary neurosurgical resident to provide insight into the physicians who currently choose to pursue the field. To do so, we investigate patterns of personality typing of neurosurgical residents throughout the United States (US). Since individuals can vary widely with respect to how they process both external and internal information and how they interact with the outside world including other people, an understanding of the common personality types entering the field could be beneficial to educators attempting to optimize training methodologies and improve the resident selection process.
METHODS
Current neurosurgical residents from all Accreditation Council for Graduate Medical Education accredited programs in the US were contacted via email and offered the opportunity to take an on-line survey to determine their Carl Jung and Isabel Briggs Myers personality types. It was stressed that participation was strictly on a volunteer basis. The survey results display personality typing based on four preferences (extraversion (E) and introversion (I), sensing (S) and intuition (N), thinking (T) and feeling (F), judging (J) and perceiving(P); refer to Table 1
Table 1: A description of some of the key defining characteristics of the four dichotomies which make up the sixteen Myers Briggs personality types.
|
Extraversion (E) vs Introversion (I) |
Sensing (S) vs Intuition (N) |
||
|
Prefer action over reflection |
Prefer reflection over action |
Prefer facts and details |
Prefer general concepts |
|
Learn best through doing or discussing |
Learn best through thorough mental practice |
Build card fully and thoroughly to conclusions |
Move quickly to conclusions, follows hunches |
|
Are sociable and expressive |
Are private and contained |
Trust experience |
Trust inspiration |
|
Thinking (T) vs Feeling (F) |
Judging (J) vs Perceiving (P) |
||
|
Strive for objective standard of truth |
Strive for harmony and positive interactions |
Are scheduled/organized |
Are spontaneuous/flexible |
|
Described as reasonable |
Described as compassionate |
Sees routines as effective |
Sees routines as limiting |
|
Want everyone treated equally |
Want everyone treated as an individual |
Try to avoid last minute stresses, finishes tasks well before deadlines |
Feel energized by last minute pressures, finishes tasks at the deadlin |
for an explanation of the dichotomies) to create a four letter type of which there are sixteen permutations (e.g., ENFJ, ISTP…etc). The distribution of these types in the general population is shown in Figure 1.
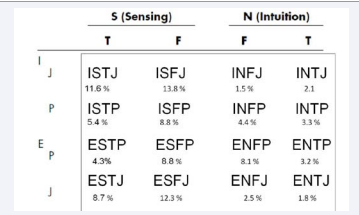
Figure 1 The distribution of the sixteen Myers Briggs personality types in the general population. Personality typing is based on four preferences (extraversion (E) and introversion (I), sensing (S) and intuition (N), thinking (T) and feeling (F), judging (J) and perceiving(P)) to create a four letter type. The estimated frequency table was compiled from data from 1972 through 2002, including data banks at the Center for Applications of Psychological Type, Inc and Stanford Research Institute and is available at www.myersbriggs.org.
Using an online survey for data collection the results were then sorted by result and postgraduate year. Additionally, participants were given the option of reporting their training institution.
Statistics were performed on commercially available software. For comparison of proportions between groups a Fisher test was performed. A p value of 0.05 was predetermined to be significant. For the sample size of the general population available from www.myersbriggs.org a sample size of 1,000 was assumed as a conservative estimate so as not to overstate our findings.
RESULTS
A total of 108 resident responses were received (~15% response rate). The distribution of responses by postgraduate year (PGY) was as follows: PGY 1 (n=7), PGY 2 (n=7), PGY3 (n=31), PGY 4 (n=15), PGY 5 (n=10), PGY 6 (n=15), PGY 7 (n=15).
48 (44.4%) respondents listed their training program. From these responses, residents represent at least twelve programs. While the Midwest region was the most common location, programs covered all areas of the country. Table 2
Table 2: Relative proportions of the four Myers Briggs personality type dichotomies among all neurosurgical residents compared to the general population. Data is listed as ratio of each dichotomy as a percentage for the general population and for the resident responses as (n:n) and percentage of the total (%). Significance values are listed as a comparison to the general population (sample size of 1,000 source Myersbriggs.org). Abbreviations: extraverted (E), introverted (I), intuitive (N), sensing (S), thinking (T), feeling (F), judging (J), perceiving (P).
|
Dichotomy |
Population (%) (n=1000) |
All Neurosurgery Resident Respondents (n=108) |
|
E:I |
49.1:50.9 |
49:59 (43.5%) p=0.48 |
|
S:N |
73.7:23.6 |
38:70 (35.2%) p=0.02 |
|
T:F |
40.4:59.6 |
81:21(75%) p<0.001 |
|
J:P |
54.3:45.7 |
102:6 (94.4%) p<0.001 |
summarizes the differences between the distributions of the four dichotomies in the general population compared to resident responses.
Extraversion vs. Introversion
Overall, residents reported a slight preference forextraversion (54.6%) over introversion (45.3%), which is not unlike the distribution among the general population (p=0.48).
Intuition vs. Sensing
Neurosurgical residents were more likely to gather data from intuition over sensing compared to the general population (64.8% vs. 23.6%; p=0.02)
Thinking vs. Feeling
Residents demonstrated a very strong preference for thinking rather than feeling in the decision making process, compared to the general population (75% vs. 40.4%; p<0.001).
Judging vs. Perceiving
Residents demonstrated a strong preference for a judging rather than perceiving lifestyle compared to the general population (94.4% vs. 54.3%; p<0.001).
Figure 2
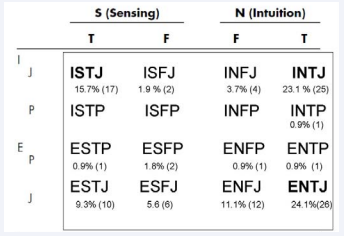
Figure 2 Distribution of the sixteen Myers Briggs personality types among neurosurgical residents. Each type is depicted by the number (n) and percentage (%). The three most common types are highlighted in bold lettering. Personality typing is based on four preferences (extraversion (E) and introversion (I), sensing (S) and intuition (N), thinking (T) and feeling (F), judging (J) and perceiving(P)) to create a four letter type.
illustrates the distribution of the sixteen Myers Briggs personality types among all residents. Thirteen of the possible sixteen MBPT were observed; those not represented include ISFP (‘artist’), ISTP (‘mechanic’) and INFP (‘idealist’). Overall, the most common types among neurosurgical residents were the four Thinking-Judging types (INTJ –‘scientist’, ENTJ – ‘executive’, ISTJ – ‘duty fulfiller’, ESTJ – ‘administrator’) and ENFJ (‘teacher’). Cumulatively, these five types are present in 83.3% of residents as compared to 26.7% of the general population (p<0.001). The four TJ types are present in 72.2% of residents compared to 24.2% in the general population (p<0.001). Of these, the most disproportionately represented types compared to the normal distribution are INTJ (25% vs. 2.1%; p<0.001) and ENTJ (26% vs. 1.8%; p<0.001) (Figure 3).
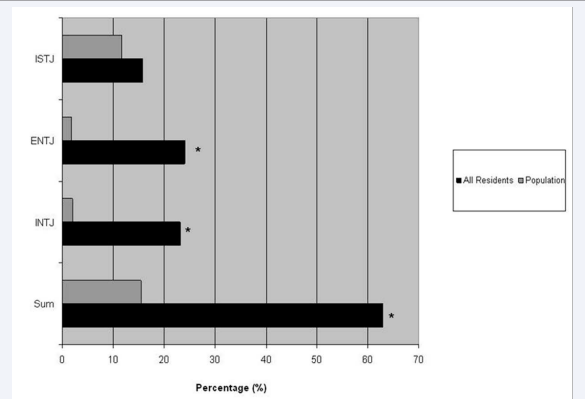
Figure 3 Frequency of the three most common types among neurosurgical residents compared to the general population. Two of the Thinking-Judging types (INTJ and ENJT) are disproportionately represented compared to the general population. Statistical significance (p<0.001) is denoted by (*).
These two types alone, while cumulatively present in only 3.9% of the general population, accounted for 51% of resident responses.
DISCUSSION
Personality typing in medicine
The Myers-Briggs personality typing instrument (MBPI) is the most widely adopted instrument used to assess a person’s innate preferences and is commonly employed for job interviews,team building exercises and for increasing self-awareness. The MBPI has been utilized in medicine most extensively in the study of medical students and their eventual career paths. Of the four preference functions, a feeling tendency has been most correlated with entering a primary care field as opposed to a specialty care field [1-5] and an extraverted and thinking type is most correlated with a surgical field [6]. While there are limitations to MBPI, we chose to employ this assessment tool to provide insights into the current neurosurgical trainee across the country.
The MBPI and other personality instruments have been used in the assessment of members of a variety of healthcare groups [4,7-14]. In all instances, the group composition has varied significantly from the normal (i.e. population) distribution of types, reflecting that specialized groups can become quite different from the general population through self-selection processes (Table 4).
Table 4: Summary of the available literature regarding Myers Briggs Personality Typing in the various medical groups that have been sampled. Results are clustered by similar types to demonstrate similarities and differences between the different specialties. Extraversion (E) and introversion (I), sensing (S) and intuition (N), thinking (T) and feeling (F), judging (J) and perceiving(P). Registered nurse (RN), respiratory therapist (RT).
|
Health Care Provider |
Prototype (E/I) (S/N) (T/F) (P/J) |
Source |
|
Surgical specialty |
_ _ T _ |
Friedman et al., 1988 |
|
Primary care |
_ _ F _ |
Friedman et al., 1988, Harris et al., 1985; Stilwell et al., 2000, Taylor et al., 1990 |
|
|
|
|
|
Health care executives |
_ _ T J |
O’Connor et al., 1992 |
|
Obstetrics gynecology |
_ S T J |
McCaulley et al., 1978, Friedman et al., 1988 |
|
General surgery |
_ S T J |
Swanson et al., 2010, McCaulley et al., 1978 |
|
Orthopedics |
_ S T J |
McCaulley et al., 1978 |
|
Endodontists and dentists |
_ S T J |
O’Neill et al., 2007, Westerman et al., 1991, Wu et al., 2007 |
|
Otorhinolaryngology |
_ S T J |
Zardouz et al., 2011
|
|
|
|
|
|
Family medicine |
_ S F J |
Taylor et al., 1990, Friedman et al., 1988 |
|
Pediatrics |
_ S F J |
Myers et al., 1976, |
|
Dental hygienists |
_ S F J |
Saline et al. ,1991, McDonald et al., 1998 |
|
Occupational therapist |
I S F J |
Radonsky et al., 1980 |
|
Registered nurses |
I S F J |
Bean et al., 1993, Jain et al., 1996 |
|
|
|
|
|
Anesthesiology |
I S _ P |
Myers et al., 1976 |
|
Physical medicine and rehabilitation |
E _ _ P |
Sliwa et al, 1994 |
|
Flight crew members (RNs, RT and pilots) |
E _ _ P |
Gabram et al., 1994 |
|
Pathology |
I N T _ |
Myers et al., 1976 |
|
Psychiatry |
_ N F P |
Friedman et al., 1988 |
For example, family medicine (_SFJ), obstetrics-gynecology (_STJ), general surgery (_STJ) and psychiatry (_NFP) have unique tendencies [1,15,16]. In addition, peer selection can also be astrong driving force towards the specialization of a group by personality composition and personality bias (like favoring the like) has also been observed during resident selection in surgical subspecialties [17].
Personality typing in neurosurgery
To date, no studies have studied the neurosurgical personality exclusively. Likely due to its relatively small size, this specialty has been either excluded or lumped together with other surgical specialties in broad terms as “surgeons”. Very strong preferences for thinking and judging over feeling and perceiving are evident among current trainees. In addition, gathering data through an intuition rather than sensing function has also been observed. Thus, a prototype of a contemporary neurosurgical resident has emerged (_NTJ followed by _STJ). This distribution of types among neurosurgical trainees varies significantly from the normal distribution, as well as from other medical specialties. Of this set of preferences, __TJ is shared most in common with other surgical specialties and health care executives, while health care providers such as family medicine and pediatrics and support staff such as nurses and occupational therapists share a strong _SFJ preference which is not common among neurosurgical residents.
NTJ prototype: Of these preferences, the most strongly prevalent among neurosurgical residents is a judging over perceiving lifestyle. It may come as no surprise since peoplewith a preference for J over P strive to maintain an organized and structured schedule with clear deadlines and expectations. The lifestyle of a neurosurgery resident is highly hierarchical and structured, consisting of morning rounds, operative cases during the day and overnight call. The second strongest preference is thinking over feeling as a means to make decisions. This preference coincides well with the requirement of a resident to remain objective and calm during a critical event, not allowing emotions to interfere with reaching the most rationale decision. A strong preference for intuition over sensing is also evident. Striking a balance between gathering sufficient detail (S) to guide one’s clinical decision making without losing sight of the big picture (N) can be challenging and both are required. In contradistinction to contemporary neurosurgical residents, there is a clear preference for S over N in other surgical fields like general surgery [7], otorhinolaryngology [10] and gynecology [13]. The field of neurological surgery requires an assessment ofthe nervous system and may be less concrete than other fields, with a stronger requirement for an intuitive sense.
Implications of personality typing
There is evidence that different personality types favor certain learning strategies and tend to score differently on subjective evaluations. These differences may have implications for likelihood of success in academic settings, including residency training. Among medical students, the _S_ J followed course objectives most closely while the _N_P was more prone to independent learning [18]. Among dental students, the _S_J earned the highest grades overall, introverts scored highest on the board examination and perceivers were most likely to be on probation [19]. While introverted medical students scored highest on objective examinations, extroverts scored more favorably on subjective evaluations [20], which ultimately placed them higher on class rank [19], which takes into account both subjective and objective measures. Among naval academy midshipmen, the ESTJ was most likely to graduate while the _F_P was the highest risk to drop out [21]. Given these differences, some graduate schools have begun tailoring teaching methodologies to certain personality types [22,23]. Additionally, knowledge of a groups’ MBPT composition can be utilized to improve teamwork, productivity, moral and efficiency, a strategy which has proven effective when applied by nurse managers in their units [24,25] and which the business world has utilized for decades.
For these reasons, it is imperative to collect data on personality types of all neurosurgical residents prospectively. This knowledge may aid in customizing teaching methods both in the operating room and in didactic sessions. It may also help to optimize the performance of the resident team managing a busy inpatient service. This is increasingly important in the era of resident duty hour regulations when teaching exposures must become higher yield. In addition, it may be of value to understand each individual’s preferences, potential strengths and weaknesses under different stressors. Such understanding could enhance the group’s performance as it strives to deliver the best possible patient care. There are certain personality types that are very likely to misunderstand each other and could result in team conflict (J vs. P and T vs. F, for example). This is of special importance in an era of work hour reform and increased bureaucratic demands (i.e., more work to be done in less time). In addition, as programs assess the progress of residents achieving milestones by incorporating subjective data from faculty evaluations, directors must be cognizant of the fact that extroverts tend to score higher on these measures [19,20]. Lastly, among faculty a type bias exists that favors their own type, which can impact the assessment of trainees [26].
Importantly, it should be stressed that there is no evidence that a single type is “best suited” for a career in neurosurgery. Rather, the relative strengths and weakness of each should be recognized to maximize patient care and the satisfaction and success of each trainee.
Study limitations
While the study attempted to survey all current neurosurgery residents the response rate achieved was lower than expected (15%). This yield could potentially bias the data towardspersonality types who are more likely to respond to survey requests. Additionally, our institution made up a disproportionate amount of the sample size (25%) which could also bias the data if our program self- and peer-selects for a certain personality type. However, we found no major differences between the results from our institution compared to those around the country.
Table 3: Description of the three most common Myers Briggs personality types among neurosurgical residents. Adapted from descriptions available at www.myersbriggs.org. Extraversion (E) and introversion (I), sensing (S) and intuition (N), thinking (T) and feeling (F), judging (J) and perceiving(P)
|
Myers Briggs Personality Type |
Description |
|
INTJ – the Scientist Mastermind |
Have original minds and great drive for implementing their ideas and achieving their goals. Quickly see patterns in external events and develop long-range explanatory perspectives. When committed, organize a job and carry it through. Skeptical and independent, have high standards of competence and performance. |
|
ENTJ – the Executive Leader |
Frank, decisive, assume leadership readily. Quickly see illogical and inefficient procedures and policies, develop and implement comprehensive systems to solve organizational problems. Enjoy long-term planning and goal setting. Usually well informed, well read; enjoy expanding their knowledge and passing it on to others. Forceful in presenting their ideas. |
|
ISTJ – the Duty Fulfiller |
Quiet, serious, painstaking, systematic, hard-working and careful with detail, earn success by thoroughness and dependability. Practical, matter-of-fact, realistic, and responsible. Decide logically what should be done and work toward it steadily, regardless of distractions. Hold a tremendous amount of facts. Take pleasure in making everything orderly and organized. Value traditions and loyalty. |
CONCLUSIONS
We have provided insights from contemporary neurosurgical residents by compiling MBPI responses from a survey offered to all current neurosurgical residents in the US. A strong preference for thinking, judging and intuition functions is apparent. This combination of preferences (NTJ) distinguishes neurosurgical residents from any other medical group that has been described in the literature. Further study including larger sample size, longitudinal studies of residents, career paths, job satisfaction and success will determine how to apply this data to allow for the most beneficial impact on resident selection and education.
REFERENCES
- Friedman CP, Slatt LM. New results relating the Myers-Briggs Type Indicator and medical specialty choice. J Med Educ. 1988; 63: 325-327.
- Nieman LZ, Holbert D, Bremer CC. Career preferences, career decision-making, and orientation toward medicine among third-year students. J Med Educ. 1988; 63: 474-476.
- Burkett GL, Gelula MH. Characteristics of students preferring family practice/primary care careers. J Fam Pract. 1982; 15: 505-512.
- Taylor AD, Clark C, Sinclair AE. Personality types of family practice residents in the 1980s. Acad Med. 1990; 65: 216-218.
- Wallick MM, Cambre KM, Randall HM. Personality type and medical specialty choice. J La State Med Soc. 1999; 151: 463-469.
- Stilwell NA, Wallick MM, Thal SE, Burleson JA. Myers-Briggs type and medical specialty choice: a new look at an old question. Teach Learn Med. 2000; 12: 14-20.
- Swanson JA, Antonoff MB, D'Cunha J, Maddaus MA. Personality profiling of the modern surgical trainee: insights into generation X. J Surg Educ. 2010; 67: 417-420.
- Gabram SG, Hodges J, Allen PT, Allen LW, Schwartz RJ, Jacobs LM. Personality types of flight crew members in a hospital-based helicopter program. Air Med J. 1994; 13: 13-17.
- Warschkow R, Steffen T, Spillmann M, Kolb W, Lange J, Tarantino I. A comparative cross-sectional study of personality traits in internists and surgeons. Surgery. 2010; 148: 901-907.
- Zardouz S, German MA, Wu EC, Djalilian HR. Personality types of otolaryngology resident applicants as described by the Myers-Briggs Type Indicator. Otolaryngol Head Neck Surg. 2011; 144: 714-718.
- Eng MK, Macneily AE, Alden L. The urological personality: is it unique? Can J Urol. 2004; 11: 2401-2406.
- Boyd R, Brown T. Pilot study of Myers Briggs Type Indicator personality profiling in emergency department senior medical staff. Emerg Med Australas. 2005; 17: 200-203.
- Neral SM, Collins J, Gandy MJ, Hampton HL, Morrison JC. Non-cognitive variables and residency choice. J Miss State Med Assoc. 2008; 49: 327-329.
- Needleman HL, Bang S, Zhou J, Johnson JR, McPeek B, Graham D. Personality types of pediatric dentists: comparative analysis and associated factors. Pediatr Dent. 2011; 33: 37-45.
- McCaulley MH. Application of the myers briggs type indicator to medicine and other professions. Washington, DC. US Department of Health, Education and Welfare, 1978.
- McCaulley MH. The myers-briggs type indicator in career planning. Gainesvile, Florida: Center for Applications of Psychological Type. 1981.
- Quintero AJ, Segal LS, King TS, Black KP. The personal interview: assessing the potential for personality similarity to bias the selection of orthopaedic residents. Acad Med. 2009; 84: 1364-1372.
- Harasym PH, Leong EJ, Lucier GE, Lorscheider FL. Relationship between Myers-Briggs psychological traits and use of course objectives in anatomy and physiology. Eval Health Prof. 1996; 19: 243-252.
- Jones AC, Courts FJ, Sandow PL, Watson RE. Myers-Briggs Type Indicator and dental school performance. J Dent Educ. 1997; 61: 928-933.
- Davis KR, Banken JA. Personality type and clinical evaluations in an obstetrics/gynecology medical student clerkship. Am J Obstet Gynecol. 2005; 193: 1807-1810.
- Murray KM, Johnson WB. Personality type and success among female naval academy midshipmen. Mil Med. 2001; 166: 889-893.
- Jessee SA, O'Neill PN, Dosch RO. Matching student personality types and learning preferences to teaching methodologies. J Dent Educ. 2006; 70: 644-651.
- McNulty JA, Espiritu B, Halsey M, Mendez M. Personality preference influences medical student use of specific computer-aided instruction (CAI). BMC Med Educ. 2006; 6: 7.
- Schoessler M, Conedera F, Bell LF, Marshall D, Gilson M. Use of the Myers-Briggs Type Indicator to develop a continuing education department. J Nurs Staff Dev. 1993; 9: 8-13.
- Costello K. The Myers-Briggs type indicator--a management tool. Nurs Manage. 1993; 24: 46-47, 50-1.
- Bell MA, Wales PS, Torbeck LJ, Kunzer JM, Thurston VC, Brokaw JJ. Do personality differences between teachers and learners impact students' evaluations of a surgery clerkship? J Surg Educ. 2011; 68: 190-193.









































































































































