Diagnosis of Temporo Mandibular Joint Disorders with Infectious Etiology
- 1. Residence program in TMJ, Catholic University of Salta, Argentina
- 2. Orthodontic Specialist of the Argentinian, Orthodontic Society of Corrientes, Argentina
Abstract
Aim: The occurrence of different types of bacteria in the temporomandibular joint (TMJ) is considered an etiological factor in TMJ pathologies. Chlamydia trachomatis (ChT) and Mycoplasma pneumonia (MP) can be present in different joint pathologies. The aim of this study is to introducediagnostic resources for patients with temporomandibular joint disorders of infectious etiology.
Method: Two male patients with temporomandibular joint disorders were evaluated. Diagnostic resources included the interpretation of mandibular condyle lesions in NMR, and immunofluorescence tests of specific Anti-IgG and IgM antibodies for ChT and MP.
Conclusions: NMR imaging interpretation and laboratory studies can reveal the presence of bacteria in the TMJ, thus facilitating correct differential diagnoses of TMJ pathologies
Keywords
• Temporomandibular disorders
• Nuclear magnetic resonance
• Serological tests
• Chlamydia trachomatis
• Mycoplasma pneumonia
• Temporomandibular joint
Citation
Learreta JA, Barrientos EE (2017) Diagnosis of Temporo Mandibular Joint Disorders with Infectious Etiology – Two Case Reports. JSM Oro Facial Surg 2(1): 1005.
INTRODUCTION
Knowledge of the anatomical structures of the temporomandibular joint (TMJ), is fundamental for diagnosing the pathologies that its tissues may undergo. Studies of sections in sagittal, frontal and horizontal planes of the temporomandibular joint allowed a three-dimensional analysis of the TMJ and the relation of the joint capsule with surrounding structures.
Sagittal section cuts of the posteromedial area of the mandibular condyle show the superior laminastrongly attached to the petrotympanic fissure, where some fibers extend through it, their insertion terminating in the anterior ligament of the hammer. The thinner inferior lamina is attached to the medial region of the pterygoid muscle fascia. Laterally, it inserts into the neck of the mandible and into the mandibular condyle.
The retrodiscal area presents loose connective tissue, with lobules of fatty tissue, and it contains a venous plexus and numerous nerve fibers [1]. It is vascularized by atrial, anterior tympanic and superficial temporal arteries, and innervated by the temporal auricular nerve [2]. It is the underlying posterior nutritional pole, given the existence of vascular plexuses that allow nutrition and hydration of the joint, where a large number of cells constituting synovial fluid elements are also found [3].
Hard and soft tissues may be altered by different etiological agents [4] such as traumatic [5] and autoimmune factors [6-8]. Although genetic factors are not direct causes of these pathologies, they create unfavorable conditions for clinical recovery and health restoration [9]. Different dental malocclusions, such as posterior tooth loss, may lead to condylar dislocations and soft tissue alterations [10-12]. Changes in the incisal guidance, such as retractions or inadequate torques, may alter the anteroposterior relationship of the mandible, generating posterior displacement of the mandibular condyle and compression of retrodiscal tissues [13,14].
Bacterial factors, different investigations [15-21] reveal a great diversity of bacteria in the TMJ, which can act as etiological agents of TMJ pathologies:
Henry [15] investigated whether the presence of bacteria associated with reactive arthritis could be identified in the TMJ. Posterior bi laminar tissue removed during TMJ surgery from 26 patients was evaluated for the presence of Chlamydia trachomatis, Mycoplasma fermentans, Mycoplasma orale and Mycoplasma genitalium, among others. The presence of Mycoplasma genitalium in the human TMJ had not been previously reported. He concluded that the presence of bacteria in the TMJ may serve as the pathogenetic mechanism of TMJ inflammation.
Sun W [17] identified a wide variety of bacteriain the synovial fluid from patients with TMJ disorders. Laboratory tests indicated that 67.86% of the samples were bacterial DNA-positive.
Wanyura H [18] established the presence of Borrelia burgdorferi spirochete in the histo pathological material obtained from the intra-articular space by arthroscopy from patients with advanced TMJ disorders.
Adachi [20] related myco bacterial infection with TMJ pathologies, as findings suggest that some cases of TMJ disorders are concerned with the synovial IgG against the EF-Tu of M. tuberculosis. The existence of the antibody is a clinical indication of TMJ disorders.
The aim of the present study is to present diagnostic resources for patients with temporomandibular joint disorders of infectious etiology.
METHOD
Two male patients were evaluated: Patient1, aged 37, and patient 2, aged 47, who attended private consultation due to temporomandibular disorders and symptoms such as TMJ pain, difficulty in chewing, limitation to mouth opening, headaches and neck pain. In both cases, the TMJ diagnosis was performed through standardized questionnaires, imaging studies, including NMR (in sagittal and frontal sections) and protocol of Prof. Dr. Jorge A. Learreta. In Patient 2, with a NMR obtained 2 years ago, new studies were performed with the same resonator.
Immuno fluorescence tests of Anti-IgG and IgM specific antibodies for ChT and MP were requested, as mandibular condyle lesions were observed in NMR (Figures 1c,3c). Patients received detailed information about the aim and procedures of the studies to be performed.
RESULTS
In patient 1, mandibular condyle lesions observed in NMR were described as hypo intense images located in the upper pole, triangular in shape, with one of their vertices towards the condylar depth. (Figure 1 a,b).
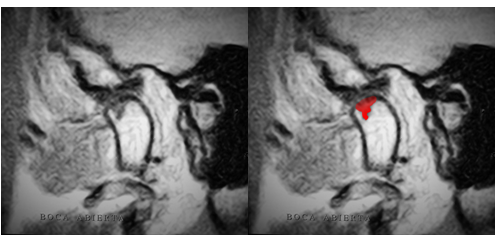
Figure 1a Figure 1b
Figure 1a: RNM T1.Sagittal cut of TMJ with mouth open shows characteristic lesions on the condylar head for ChT, and a triangular, hypointense image in the upper pole, one of its vertices towards the condylar depth.
Figure 1b: Characteristic lesion of ChT highlighted in color.

Figure 1c: Positive laboratory tests. Anti-IgG antibody was 1/16 and Anti-IgM antibody was 1/16, for ChT.
Anti IgG and Anti IgM laboratory tests for ChT were both 1/16 positive, the negative reference value being lower than 1/16.
On the first study in patient 2, the lesions observed in the mandibular condyle were described as hypo intense images of irregular shape, from the cortical to the medullary areas of the mandibular condyle, in the anterior, superior and posterior pole (Figure 2 a,b).
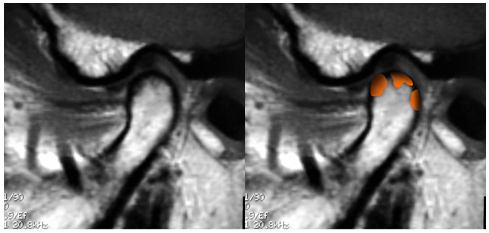
Figure 2a Figure 2b
Figure 2a: RNM T1.Sagittal cut of the TMJ with mouth closed shows characteristic lesions on the condylar head for MP, and an irregular hypo intense image from the cortical to the medullary area of the mandibular condyle, in the anterior, superior and posterior pole.
Figure 2b: Characteristic lesion of MP highlighted in color.
The new study shows loss of bone tissue in the anterior pole due to progression of the lesion, and hypo intense images in the superior and posterior poles (Figure 3 a-b).
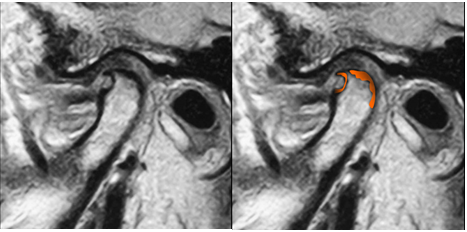
Figure 3a Figure 3b
(2 years after the first NMR)
Figure 3a: RNM T1. Sagittal cut of the TMJ with mouth closed shows progression of lesions with bone loss in the anterior pole of the condyle. Hypo intense images of irregular shape in the superior and posterior pole.
Figure 3b: Characteristic lesion of MP highlighted in color.

Figure 3c
Figure 3c: Laboratory test: Anti-IgG antibody was 1/320 positive for MP.
The Anti-IgG antibody test was 1/320 positive for MP, the negative reference value being lower than 1/10.
DISCUSSION
In the present study, NMR was used to diagnose lesions of the mandibular condyle, as it is one of the main imaging methods employed for the diagnosis of TMJ pathologies [22,23]. Being a noninvasive test that allowsto obtain images on different planes, magnetic resonance has become a first-line study for diagnosing TMJ pathologies [24]. Anatomical structures of the TMJ and their relationships can be clearly observed [25], and it facilitates discovery of alterations that cannot be visualized by any other imaging method. In addition, clinical symptoms of temporomandibular disorders can be correlated with findings in NMR [26,27].
Lesions in the mandibular condyle were described according to bacterial genera. ChT cases how a hypo intense image in the upper pole, triangular in shape, with one of its vertices towards the condylar depth. MP cases show a hypo intense image of irregular shape on the cortical area towards the medullary section of the mandibular condyle, in the anterior, superior and posterior pole. In patient 2, comparing a present study with that obtained two years ago, progression of the lesion located in the anterior pole can be observed, along with a cavity and loss of bone tissue.
Bone marrow lesions of the mandibular condyle can be diagnosed through NMR [28,29]. Emshoff R, 2003 [29] found a relationship between bone marrow edema and disc displacement, osteoarthritis, and effusion in NMRs of 120 TMJs in 73 consecutive patients with symptoms of joint pathology. Although there is a relationship, these alterations may not be regarded as the unique and dominant factors in TMJ bone marrow edema instances. Images along with serological tests of Anti-IgG and IgM antibodies for ChT and MP confirmed the diagnosis. In patient 1, both AntiIgG and Anti-IgM antibody results were 1/16, positive for ChT. In patient 2, Anti-IgG antibody was 1/320 positive for MP.
Henry, 1999 [30] investigated the correlation between degenerative changes of the TMJ and the presence of ChT in the joint. A total of 31 tissue samples from the bilaminar area were analyzed through PCR. Results showed that 39% was DNA positive for ChT, concluding that the presence of this microorganism can serve as an etiological mechanism for TMJ dysfunctions, as likewise demonstrated in other joints. In a subsequent study [31], antibody increase was found in patients with internal TMJ disorders.
Paegle Dl, 2004 [32] investigated the occurrence of serum antibodies to Chlamydia trachomatis, Chlamydia pneumonia, and Chlamydia psittaci in patients with temporomandibular joint (TMJ) monoarthritis, chronic closed lock, and in control subjects. The occurrence of serum antibodies to C. trachomatis was significantly higher in patients than in control subjects, but this occurrence did not correlate with the severity of observed tissue changes. Nevertheless, an association may exist between the presence of C. trachomatis and TMJ disease.
Watanabe, 1998 [19] detected the presence of Mycoplasma salivarium and Mycoplasma fermentans in the synovial fluid of patients with pain and anterior disc displacement. The presence of these mycoplasmas in TMJs may damage the synovial membrane and cartilage with their enzymatic activities and metabolites. They will certainly affect the balance between cytokines and their inhibitors in TMJs by their cytokine-inducing activities, and could thus be a cause of pathological changes. In previous research, pathognomonic NMR images and laboratory tests allowed correlation between TMJ pathologies and MP [33].
CONCLUSIONS
The TMJ, as other joints of the human body, is not exempt from disorders due to various etiological causes, among them, infections. The combination of specific laboratory studies and the interpretation of NMR images allow differential diagnoses of TMJ pathologies.
REFERENCES
3. Learreta JA. Anatomía de la Articulación Temporomandibular. Actualización de la misma. Revista de la Sociedad Odontológica de la Plata. Año X. 1997; 19: 17 -26.
17. Kim SJ, Park YH, Hong SP, Cho BO, Park JW, Kim SG. The presence of bacteria in the synovial fluid of the temporomandibular joint and clinical significance: preliminary study. J Oral Maxillofac Surg. 2003; 61: 1156-1161.








































































































































