Porcelain Veneers and Zircon-Porcelain Crowns for the Esthetic Treatment of Severely Discoloured Anterior Teeth
- 1. Department of Prosthodontics, University of Zagreb, Croatia
- 2. Department of Periodontology, University of Zagreb, Croatia
Abstract
A woman (38 years) with tetracycline-stained maxillary anterior teeth came to dental office to improve her appearance.
The porcelain veneers and zircon-porcelain crowns were selected as the best treatment option to mask the stained teeth. Medial line, occlusal line, level of gingival margin and frontal plane alignment of maxillary anterior teeth was analysed. Direct composite laminates were placed on the frontal surface of the teeth prior any treatment with intention to present the final result to the patient. Tooth structure was reduced from 0.5 to 1 mm for the porcelain veneers and 0.6-2 mm for the zircon-porcelain crowns. Double cord technique and two-step putty wash impression technique was obtained. The master dies (for veneers) were duplicated in the investment material. For veneers, the opaque porcelain was applied at first. The zirconiaporcelain crowns were made of the zircon with the ceramic veneering material.
Veneers and crowns were positioned to verify marginal adaptation, alignment, shape, size and color, as well as occlusal contacts. The patient was satisfied with the esthetics and the restorations were luted.
This case report shows clearly that the final result and high esthetical standards are result of a detailed plan of treatment. The OHIP-49 revealed significantly improved oral health related quality of life after the treatment. Porcelain veneers and zirconium-porcelain crowns offer a reliable and effective procedure for the esthetic treatment of anterior teeth.
Keywords
• Tetracycline-stained teeth
• Porcelain veneers
• Zircon-porcelain crowns
• OHIP
• Direct composite laminates
• Double cord technique
• Two-step putty wash impression technique
Citation
Petricevic N, Puhar I (2017) Porcelain Veneers and Zircon-Porcelain Crowns for the Esthetic Treatment of Severely Discoloured Anterior Teeth. JSM Oro Facial Surg 2(2): 1010.
INTRODUCTION
The great challenge in esthetic dentistry is the treatment of discolored healthy anterior teeth. For many years, the most predictable and durable esthetic correction has been achieved by full crowns. This approach requires a large amount of sound dental structure to be removed. The adhesive dentistry and new luting systems have enabled the development of porcelain veneers [1]. The contemporary dentistry proposes the porcelain veneers to be durable anterior restorations with superior esthetics [2]. The great improvement in the metal-free porcelain veneers and crowns result in good fracture resistance and marginal adaptation [3]. The reports of their successful clinical performance to mask tooth discolorations and/or to correct the unaesthetic tooth form and/or position have been steadily increasing their popularity among dental practitioners [4,5].
This paper will present a clinical case and discuss the advantages and difficulties when using the porcelain veneers for the restorative treatment.
CLINICAL CASE
A female subject (38 years) with a tetracycline stained frontal teeth had come to the dental office in order to improve her appearance (Figure 1,2),

Figure 1: Pretreatment, facial view

Figure 2: Pretreatment, occlusal view
after the initial periodontal treatment. Treatment options were presented and discussed with the patient, and prosthodontic treatment was selected as the best choice for this case, as previous dental bleaching had given no satisfactory result. Advantages and disadvantages of the crowns and veneers were weighted. The porcelain veneers were selected as the best treatment option in order to save the dental structure and as the best alternative to mask the stained teeth. Since large resin composite restorations had been found on the maxillary right central incisor and on the maxillary left first premolar, the zircon-porcelain crowns were elected as a more suitable restorative strategy for those teeth.
The mandibular frontal teeth were not included in the restorative treatment, since only the incisal halves of the crowns were visible during speech or smile and had not been stained by tetracycline.
PREPARATIONS FOR TREATMENT
Irreversible hydrocolloid impression (Vival NF, Ivoclar Vivadent) of the maxillary teeth was made in order to save the information about the natural teeth dimensions. This was useful for the dental technician in order for him to produce the veneers and the crowns of the similar dimensions as those of the natural teeth.
Prior to the treatment, the problem analysis from the esthetic point of view was made in order to detect all disharmonies of the dental arches (Figure 3).
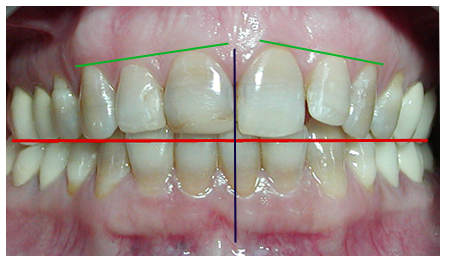
Figure 3: Problem analysis from the esthetic point of view; medial line, occlusal line and level of gingival margin.
The medial lines of the maxillary and mandibular dental arches were not in harmony, but it was of no importance to the patient. In order to achieve a perfect level of gingival margins, it was proposed to perform the clinical crown lengthening on the maxillary right lateral incisor, but the patient had disagreed. The analysis of the occlusal plane also showed some discrepancies that could be easily corrected by elongating the crown of the maxillary right central incisor and the maxillary left lateral incisor, and the patient had accepted the proposed option.
In order to achieve a perfect esthetics, the veneers had to be aligned in the frontal plane. The labial promenading and mesial side rotation of the maxillary left lateral incisor required more tooth reduction, and also served as a point of reference in the frontal plane alignment and enamel reduction (Figure 1,2). On the maxillary right first premolar the Class I composite restoration was not considered to be a contraindication for a veneer restoration, since the contact line between them would have been only on the occlusal surface of the tooth.
Since this therapy would have changed the appearance of the maxillary arch, it was decided to inform the patient about the final result. The best solution was to make the provisional veneers in dental laboratory (mock-up) and to bond them on the facial surface of the teeth, so that the final result could be presented to the patient. Since there had been a time and money consuming problem, direct composite veneers were made on the frontal surface of the maxillary frontal teeth (Figure 4).

Figure 4: Direct composite veneers were placed on the frontal surface of the teeth
They were held in place by a small area of etched enamel in order to demonstrate the final alignment and shape of the veneers and crowns [6]. Different composite shades were used for each provisional veneer, so that the patient herself would be actively participating in the decision making regarding the permanent porcelain (veneers and crowns) shade solution. This preparatory phase of the treatment had directed the therapy in a more predictable course and results with high level of patient’s satisfaction in the final stage. This was extremely important as the veneer restoration would have been luted in the next visit.
Second irreversible hydrocolloid impression of the maxillary teeth, provided with provisional veneer, and was made in order to save the information about the position of the direct composite laminates, which corrected the alignment of the maxillary frontal teeth. This was also useful to dental technician during laboratory procedures. Another polyvinyl siloxane impression (putty) (Express STD, 3M ESPE) was made to use it as silicon key for control of reduction of the tooth structure.
TOOTH PREPARATION
According to Shillingburg, the preparation of the tooth for veneer should be between 0.3 and 0.5 mm [7]. The reduction of the tooth structure also depends on the severity of the discoloration and the position of the tooth. Therefore, discolored teeth preparation should be extended between 0.5 and 1 mm [8,9].
In order to limit the preparation to the desired depth, the calibrated diamond bur (#200191AA, Diatech) was used to make 0.5 mm deep horizontal grooves in the facial side of the tooth (with the direct composite laminates in place) [5]. A 1 mm wide bur (#200691AA, Diatech) was used to make 1 mm deep grooves in the incisal half of the facial side. Next, the bottom of the grove was colored with a red marker in order to mark the level until which the tooth structure should be reduced (Figure 5).

Figure 5: The surface of the tooth was colored with a black marker and the bottom of the groove with a red marker
A roundend diamond bur (#200094AA, Diatech) was used to make a groove in the level of gingiva, parallel to its mesio-distal aperture. The tooth structure was reduced with a round-end taperedcylinder diamond bur (#200470AA, Diatech) until the red color marking was removed (Figure 6).

Figure 6: Reduction of the tooth structure of the maxillary left central incisor is controlled by the silicon key
The retraction cord (#00, Ultrapak, Ultradent) was placed in the sulcus and chamfer finish line was submerged 0.5 mm subgingivally. Facial reduction was extended on the proximal sides beyond the interdental contact. The same bur was used to make a 0.5 mm deep palatal overlap, terminating with a chamfer finish line and incisal notches (Figure 6). The overlap of the incisal edge provided a better control of the esthetics of the incisal part, and it also enhanced resistance of the restoration to incisal fracture [6,7]. Silicon key was used to control the reduction of the tooth structure (Figure 6). Finally, the preparation was finished with fine-grained diamond instruments.
Large composite restorations were present on the maxillary right central incisor (Class IV and complete palatal side) and on the left first premolar (Class II). Therefore, the zircon-porcelain crowns were indicated as a more suitable restorative strategy for those particular teeth. The tooth-substance reduction for the zircon-porcelain restoration is more necessarily; 0.6 mm is considered to be a minimum depth of preparation in the cervical region, the facial side reduction should be up to 1 mm and the occlusal side reduction up to 2 mm [3].
In order to achieve good and reproducible impressions, the double cord technique (Ultrapak ,Ultradent) was applied. The initial thin cord was placed in the sulcus (#00), and the second thicker cord (#1) was applied over the first one, and was then removed shortly before the impression was made. The two-step putty wash impression technique was applied with a polyvinyl siloxane material (putty and light-body viscosities) (Express, ESPE) (Figure 7).

Figure 7: Two-step putty wash impression technique made with a polyvinyl siloxane material
The impression of the opposing arch was made with irreversible hydrocolloid (Vival NF, Ivoclar Vivadent). Temporary restorations were made of the composite material (System pc & b, Ivoclar Vivadent) and cemented with temporary cement (Systemp cem, Ivoclar Vivadent). The impressions were sent to the dental laboratory.
DENTAL LABORATORY PROCEDURE
The master dies (for veneers) were duplicated (Adisil blau 9:1, Siladent) and refractory dies were poured in the investment material (Ducera Lay Super Fit, Degudent) [3]. At first, the opaque porcelain was applied, and then the veneer was built up to full contour (Duceram Kiss, Degudent).
The zircon-porcelain crowns were made of zirconium oxide ceramics (Cercon, Degudent) with the ceramic veneering material specifically developed for zirconia frameworks (Cercon ceram kiss, Degudent) [3].
The luting surfaces of the veneers were air-abraded before insertion.
TESTING AND LUTING
Veneers and crowns were positioned to verify marginal adaptation, alignment, shape, size and color, as well as occlusal contacts. As the patient was satisfied with the esthetics, the restorations were luted.
Prior to luting, the inner surface was etched with 5% hydrofluoric acid (IPS Ceramic Etching Gel, Ivoclar Vivadent) for 60 seconds, rinsed and dried. A silane-coupling agent was applied on the inner surface of the porcelain veneers (Monobond-S, Ivoclar Vivadent) and the zircon-porcelain crowns (Metal/Zirconia Primer, Ivoclar Vivadent) left for 3 minutes and air-dried.
Since the rubber dam does not offer the most suitable solution for preventing the sulcus fluid to wet the luting surface, retraction cords were placed in the sulcus [10].
The surface of the teeth was etched for 15 seconds with 37% phosphoric acid gel (Total Etch, Ivoclar Vivadent), rinsed and dried. Dual-curing adhesive was applied (Excite DSC, Ivoclar Vivadent) and air-dried.
Dual-curing resin cement (Variolink II, Ivoclar Vivadent) was applied to the internal surface of the restorations. The restorations were positioned and light-cured for 10 seconds (Bluephase 8, Ivoclar Vivadent). The resin cement residues were removed with a dental probe and light-curing was continued for another 40 seconds at the lingual sides of the veneers (Figure 8-10).

Figure 8: Posttreatment, occlusal view, 4 weeks later. The contact of the maxillary right first premolar and the antagonistic tooth is located on the new resin composite restoration.

Figure 9: Post treatment, labial view, 4 weeks later.

Figure 10: Post treatment view, 8 weeks later.
OHIP
The concept of oral health –related quality of life (OHRQoL) attempts to characterize the patients’ perception of oral health. Therefore, in order to measure the social and psychological impact of oral condition and treatment procedure on the patient’s OHRQoL, the OHIP questionnaire was completed [11]. Responses were given on a Likert-type scale (0=never, 1=hardly ever, 2=occasionally, 3=fairly often, 4=very often). 0 indicates absence of any problem and each higher score represents more impaired oral health. Addition was made for all 49 items, as well as for seven domains, in order to represent a change in the score results and the impact of treatment on the patient’s OHRQoL (Table 1). As expected, the OHIP score was lower after the treatment, which confirms the impact of treatment procedure on the patient’s OHRQoL. Since the treatment improved the patient’s appearance, the most impaired item was the “Psychological discomfort”. Cultural adaptation of the OHIP instrument is a great advantage that enables the international comparability of this measurement with similar ones [12].
Table l: OHIP score results.
| Prior treatment | After treatment | |
| OHIP 49 | 46 | 8 |
| Functional limitations | 10 | 1 |
| Physical pain | 8 | 3 |
| Psychological discomfort | 14 | 1 |
| Physical disability | 10 | 3 |
| Psychological disability | 4 | 0 |
| Social disability | 0 | 0 |
| Handicap | 0 | 0 |
DISCUSSION
Masking the extremely discolored teeth (by endodontic treatment or tetracycline) is difficult to predict and frequently it results with an unpleasant color [13,14]. Great improvement in porcelain veneers has led to the more satisfying results in the treatment of unaesthetic anterior teeth. Therefore, porcelain veneers have become a desirable treatment option [2-5].
The clinical success of porcelain veneers, built up with alternating layers, depends on the accurate selection of cases and correct execution of clinical and laboratory procedures. The rehabilitation involved maxillary anterior teeth with feldspathic porcelain veneers made on refractory dies. The advantage is color control, what is crucial in aesthetic improvement of stained teeth, but strength is a weak side of layering technique. On the other side, strength of crowns made of zirconium oxide ceramic is superior, but low color control and need for more reduction of the tooth volume makes it less desirable solution.
Many studies were focused on the effects of the opaque luting cement or ceramic materials to mask a discolored background. According to Chen et al., the extreme discolorations could be corrected by using opaque porcelain for veneer build up, and by luting them with the opaque composite resin [15]. According to Heffernan et al., zirconia framework has the best opaque effect in comparison to other all-ceramic systems [16]. On the contrary, Vichi et al., demonstrated that the thickness of the ceramic material is critical in order to achieve a desirable color and the preparations should not be limited to the enamel [17]. The dark substrate can also be masked with the heat-pressed ceramic of a desirable thickness, and without any opaque material [18]. The property of the opaque porcelain and zircon-porcelain to mask the tetracycline discoloration is their great advantage, especially if the tooth reduction has to be more radical, in order to achieve a proper veneer alignment in the frontal plane. Since tetracycline color is more visible in dentin, the deeper the preparation is, the darker the teeth will be [9].
Among the most common esthetic problems associated with the porcelain veneer is the impact of the luting cement on the final shade of the veneer [1]. Since the opaque porcelain and zircon-porcelain do mask the sub structure, and also the luting cement, the shade of the luting cement is of no concern. Therefore, unpleasant esthetic surprises would occur.
The depth of the preparation is important for the satisfactory bonding strength between a tooth and the veneer. The newgeneration dentin adhesive-systems enables satisfactory bond-strength of the porcelain bonded to dentin, but the bond strength of the porcelain bonded to enamel is still superior [19]. If a part of dentin is exposed it should not impact the strength of the adhesive system, but the problem occurs if a great part of the preparation does penetrate into dentin [19]. According to Friedman, debonding will occur if 80% or more of the preparation penetrates the dentin [4]. This could be a problem if the tooth reduction has to be more necessarily, in order to achieve a proper veneer alignment in the frontal plane. Therefore, whenever possible, at least 50% of the preparation should be end in the enamel [20].
SUMMARY-CONCLUSION
This case-study clearly shows that the final result and high esthetic standards are the result of a detailed plan of treatment. Porcelain veneers and zircon-porcelain crowns offer a reliable and effective procedure for the conservative and esthetic treatments of the anterior teeth.
ACKNOWLEDGMENTS
This study was supported by the grant number No. 065- 0650446-0420 of the Ministry if Science, Education and Sports of Croatia. The authors thank Dr. Hrvoje Starcevic and dental technician Zdravko Tometic for their contribution to the article.
REFERENCES
3. Blanckenburg H, Wüstefeld F. Interdisziplinäre Behandlungsplanung und komplexe Versorgung einer Patientin mit Kronen und Brücken aus der Zirkonoxidkeramik Cercon. Berlin:Quintessenz. 2004.
5. Gürel, G: The Science and Art of Porcelain Laminate Veneers. Quintessenz. 2003.
8. Fortin DJ. Porcelain veneers: a challenging case. J Can Dent Assoc. 1999; 65: 110-112.
9. Gürel G. Keramikveneers bei Tetracyclinverfärbungen. Quintessenz Zahntech. 2004; 30: 152-168.
18. Cornell DF. Ceramic veneers: Understanding their benefits and limitations. Quintessence Dent Technol. 1998; 21:121-132.
20. Garber DA, Goldstein RE, Feinmann RA. Keramische Verblendschalen (Veneers). Berlin: Quintessenz. 1989.








































































































































