Reconstruction of Localized Horizontal Maxillary Ridge Defect with Subepethelial Connective Tissue Graft
- 1. Department of Periodontics, D.Y Patil School of Dentistry, India
- 2. Department of Prosthodontics, M.G.M Dental College & Hospital, India
Abstract
The goal of all prosthetic treatment is to obtain a satisfying functional and esthetical oral status. In a fixed bridge, the pontic frequently give the impression that they rest on the top of the ridge rather than emerge from within the alveolar process & lack marginal gingiva & interdental papillae. Black triangles, which almost always interfere with dentofacial esthetics, are present in the embrasure area between the pontics & between the abutments & the pontics. In other words, it may be difficult or impossible to produce a fixed prosthesis which truly restores the esthetics & function of the natural dentition. The localized alveolar ridge defect refers to the volumetric deficit of the limited extend of the bone & soft tissue within the alveolar process. Such type of ridge defect can be corrected by surgical ridge augmentation that can be accomplished by the addition of either soft or hard tissues. This case describes a procedure of surgical connective tissue augmentation of a localized deficient alveolar ridge in the maxilla, followed by fixed partial denture enhancing the esthetics, function & health.
Keywords
• Black triangles
• Connective tissue augmentation
• Localized alveolar ridge defect
Citation
Amberkar SC, Iyer JV (2017) Reconstruction of Localized Horizontal Maxillary Ridge Defect with Subepethelial Connective Tissue Graft. JSM Oro Facial Surg 2(1): 1006.
ABBREVIATIONS
SCTG: Sub-Epithelial Connective Tissue; PFM: PorcelainFused-Metal
INTRODUCTION
A beautiful smile can be crafted only against a backdrop of healthy gingiva. The relationship between periodontal health and the restoration of teeth is unique. For restorations to maintain long term, the periodontium must remain healthy so that the teeth are stable. To maintain or enhance the patient’s esthetics appearance, the tooth/tissue interface must present a healthy natural emergence profile, with gingival tissues framing the restored teeth in a harmonious manner [1].
Alveolar ridge defects have been classified into three general categories [2].
Class I: Buccolingual loss of tissue, with ridge height in an apicocoronal dimension.
Class II: Apicocoronal loss of tissue, with ridge width in a buccolingual dimension
Class III: Both Buccolingual and Apicocoronal loss of tissue resulting in loss of height and width of the ridge.
Abrams et al. [3], studied the prevalence of anterior ridge deformities in both arches of partially edentulous patients and reported the presence of alveolar ridge defects in 91% of the clinical cases. Class III clinical defects were the more prevalent (55.8%), followed by class I defects (32.8%) and class II defects (2.9%). Restoration with fixed partial dentures in these clinical cases is challenge, mainly because of the esthetic complications. Dark interdental spaces occur, and the pontic do not resemble natural teeth in terms of dimensions (shape, height, or size). Furthermore, these devices frequently cause difficulties phonetic, eating, and oral hygiene maintenance [4]. This case report describes, the unique technique of sub epithelial connective tissue graft for soft tissue ridge augmentation to correct horizontal alveolar ridge defect combined with ovate seat preparation followed with fixed prosthesis to achieve maximum esthetics and health.
CASE PRESENTATION
A 29 year- old female patient visited to the department of Prosthodontics for replacement of right central and lateral incisor and left central incisor. The dental history revealed that her teeth were extracted following trauma one year back. A through clinical and radiographic examination revealed a Siebert’s class I ridge defect in 11 and 12 region (Figure 1).

Figures 1: Pre-operative view of class I alveolar ridge defect in 12 & 11 area
In the presented case, the loss of buccolingual ridge width was more pronounced (Figure 2).

Figure 2: lateral pre-operative view of class I alveolar ridge defect in 12 & 11 area
The patient was scheduled for connective tissue autogenous graft ridge augmentation for the correction of ridge defect followed by ovate pontic seat preparation and restoration by porcelain-fused-metal (PFM) - fixed partial denture to attain maximum esthetics and health.
The maxillary right canine and left lateral incisor and canine were prepared for PFM (porcelain-fused-metal)-fixed partial denture. A provisional acrylic resin restoration was fabricated and placed over the abutment teeth. Surgical augmentation of loss of residual ridge of a horizontal nature was performed with sub epithelial connective tissue graft using envelope flap technique. This technique requires two sites preparation one is recipient site and second is donor site, which is as follow.
Recipient site preparation (Figure 3)

Figure 3: Recipient site preparation with a split –full- split thickness flap
Recipient site preparation is by envelope flap procedure. After local anesthesia with 1.8ml of 0.5% bupivacaine with epinephrine 1:100,000, a split –full- split thickness flap is first elevated on the buccal aspect of the deformed ridge, leaving the periosteum and a portion of the connective tissue overlying the alveolar ridge. The vertical incisions extend in an oblique fashion on either side of the deformed ridge and into the labial fold as high as is necessary to reposition the mucogingival junction. The horizontal incision is made slightly coronal to the palatal aspect of the ridge so as to increase the zone of masticatory mucosa available for repositioning.
Donor site preparation (Figure 4)

Figure 4: Palatal donor site preparation for harvesting sub epithelial connective tissue graft
The Sub-epithelial connective tissue graft (SCTG) was harvested from the palate by single incision technique, described by Hurzeler and Weng [5]. After local anesthesia with1.8ml of 0.5% bupivacaine with epinephrine 1:100,000, an envelope flap was designed depending upon the recipient site deformity and the amount of tissue needed. First incision was made with the blade 90º to the bone. After the first incision, the blade was angled to approximately 135º and an undermining preparation towards the median was started within the first incision. The epithelium and connective tissue are not removed, however, but are left attached along the midline. The underlying connective tissue is then removed down to the palatal osseous, and this donor tissue (Figure 5)
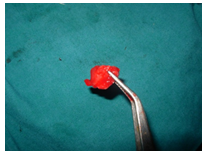
Figure 5: Sub epithelial connective tissue graft harvested from the palate
is placed on saline- soaked gauze. The donor site is sutured (Figure 6)

Figure 6: Donor site sutured
The connective tissue from donor site is placed on the recipient site base and sutured with absorbable suture (Figure 7).

Figure 7: The connective tissue from donor site is placed on the recipient site base and sutured with absorbable suture
The elevated split thickness flap is then sutured down over the connective tissue to immobilize it in the desired position and realign the mucogingival junction. The sutures remain in situ for 2 weeks.
Post-surgical instructions: Systemic antibiotics & antiinflammatory were prescribed for 5 days post-surgically. The patient was prescribed 0.2% chlorhexidine gluconate antimicrobial mouth rinse and recalled after 2 week followed by suture removal and the surgical area was irrigated with saline. The patient was recalled after 15 days for re-evaluation (Figure 8).

Figure 8: Post-operative view after 15days
After 15 days, there was substantial gain in the labial contour of the alveolar ridge. After 2 months of recall, the alveolar ridge form was evaluated & considered acceptable for the permanent prosthesis. Five unit metal ceramic prosthesis was fabricated. The aesthetic & function of the prosthesis were adequately restored. On subsequent appointments, it was noticed that, there was no relapse of the augmented ridge.
Prosthetic phase
Before the provisional fixed partial denture is cemented, the pontic must be shaped and allowed to come into contact with the soft tissue passively (Figure 9).

Figure 9: Provisional Prosthesis is given with passive soft tissue contact
This favors the formation of gingival contours adapted to the shape of the pontic. Two months post-surgery; the soft tissues have healed completely and adequately. A significant gain in tissue volume with respect to width has been achieved in bucco-lingual direction. Ovate seat preparation was carried out with flame shaped diamond bur, in relation to 12, 11, & 21(Figure 10),

Figure 10: Ovate seat preparation in relation to 12&11 for better emergence profile
the provisional restoration was modified to make a passive contact with tissue. Final restoration was given after 14 days of ovate seat preparation (Figure 11).

Figure 11: Final restoration
DISCUSSION
There are various other prosthetic and surgical options for improving aesthetics in the patient with alveolar ridge deformities, like long pontic design or gingival (pink) ceramic in the cervical region can enhance aesthetic in selected cases. Various Surgical procedures using sub-epithelial connective tissue graft, various alloplastic materials, autogenous bone grafting and guided tissue regeneration procedures can correct such type of alveolar ridge defects [6].
The case presented refers to the treatment of a class I alveolar bone defect that involved the area of two teeth i.e 12 & 11, with satisfactory results in context to dimensional stability and color match with adjacent tissue over a recall period of 2 years. The technique employed to harvest connective tissue graft by Hurzeler and Weng [5], involves a single incision for access and release of underlying connective tissue, there is maintenance of adequate blood supply to the palatal graft, no need for stents or haemostatic agents at the palatal region, and healing by first intention at the donor site, which provides adequate comfort to the patient in the post-operative stage. The main drawback lies in the gain in volume depends on the size of the graft, which is usually limited. At the same time, the techniques that involve large grafts, such as full- thickness on lay graft, are more prone to cause necrosis [7]. However, the inter positional technique implicated in this case, has an advantage of dual blood supply, i.e, provided by both the recipient site and pedicle. Within this context, the risk of necrosis is very low. Disadvantages are it is technically demanding and because of graft thickness gingivoplasty may be necessary postoperatively
Overall, it is accepted that ridges that have been augmented with sub-epithelial connective graft undergo shrinkage over the first 6 week postoperative. From 2 months post-surgery, the ridge dimensions remain stable (Figure 12).

Figure 12: Bucco-lingual palatal view showing increased ridge dimensions.
No clinical controlled studies have been performed to examine the long term stability of localized alveolar ridge augmentation with sub-epithelial connective graft. However, many authors report stability over periods of 2 to 10 years following the use of highly collagenized connective tissue.
CONCLUSION
This clinical case report suggests that soft tissue augmentation with sub-epithelial connective tissue graft harvested from the palate, in combination with a metal ceramic restoration, is a promising treatment to provide aesthetically acceptable contour to the alveolar ridge with an effective restoration.








































































































































