Identifying Trends in Patient Satisfaction in Cleft Lip Repair Using CLEFT-Q Survey Scores: A Case Series
- 1. SUNY Upstate Alan & Marlene Norton College of Medicine, USA
- 2. Department of Otolaryngology, Head and Neck Surgery SUNY Upstate Medical Center, USA
- 3. SUNY Upstate Medical University, Department of Public Health & Preventative Medicine, USA
Abstract
Orofacial clefts, including incomplete/complete cleft lip and primary vs. secondary cleft palate, are congenital abnormalities which can drastically interfere with speech, hearing, nutrition and typical infant and childhood development.
Citation
Mansour FM, Pillai A, Kavoosi T, Danning H, Wang D, Obayemi A (2026) Identifying Trends in Patient Satisfaction in Cleft Lip Repair Using CLEFT-Q Survey Scores: A Case Series. JSM Oro Facial Surg 8(1): 1019.
BACKGROUND
Orofacial clefts, including incomplete/complete cleft lip and primary vs. secondary cleft palate, are congenital abnormalities which can drastically interfere with speech, hearing, nutrition and typical infant and childhood development. With the advent of interdisciplinary treatment teams and coordinated care programs, both clinical and surgical teams co-manage care for these patients from primary repair through secondary cleft care,orthodontic care, orthognathic surgery, and definitive cleft rhinoplasty to help propel proper childhood development.
The CLEFT-Q survey has been developed with the goal of providing a more holistic assessment of patient satisfaction following orofacial cleft repair surgeries. This case series examined demographic variability in patient-reported CLEFT-Q satisfaction scores among 26 patients with non-syndromic cleft lip and palate who underwent primary lip repair and subsequent lip revision from 2014-2024.
METHODS
Approval for this study was obtained from the SUNY Upstate Medical University Institutional Review Board.
An electronic medical record mediated search of was completed using CPT and ICD-10 codes for identification of patients >10 years of age with non-syndromic cleft lip and palate who underwent primary and secondary lip repair from 2014 – 2024. Anthropometric values measured were as follows: nasal height, nasal length, right and left columellar height, columellar width, infratip height, nasal projection, interalar width, right and left cutaneous lip height, left and right upper vermillion height, midline upper and lower vermillion height, middle facial third length, and lower facial third length were obtained from profile, basal, and frontal images taken during the interdisciplinary Cleft and Craniofacial Clinic (Figure 1). These values were obtained by two independent raters using ImageJ analysis software.
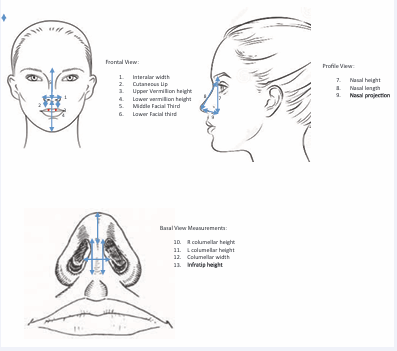
Figure 1: A schematic representation of the anthropometric values obtained from patient images.
Statistical Analysis
Inter-rater reliability for anthropometric values was calculated by means of a Bland-Altman analysis of agreement. Anthropometric values were analyzed according to demographic information through two sample t-tests and p-values were obtained using the Wilcox nonparametric test. Correlation analyses were completed to examine trends in anthropometric values and CLEFT-Q scores by patient age.
RESULTS
26 patients participated in this case series, 15 males and 11 females. 20 patients were Caucasian, 3 Hispanic, and 3 Asian. 16 patients had unilateral cleft lip with/ without palate. 7 patients had bilateral cleft lip with/ without palate. 3 patients had isolated cleft palate. The average age at secondary cleft lip revision was 7.92 +/- 6.22 years. Demographic information of study participants is summarized in Table 1.
Table 1: A Summary of the demographic information of the case series participants.
|
Demographic |
Number of Participants (%) |
|
Females |
11 (42) |
|
Males |
15 (58) |
|
Caucasian |
20 (77) |
|
Hispanic |
3 (12) |
|
Asian |
3 (12) |
|
Unilateral Cleft Lip with/without Palate |
16 (62) |
|
Bilateral Cleft Lip with/without Palate |
7 (27) |
|
Isolated Cleft Palate |
3 (12) |
|
Average age at Secondary Cleft Lip Revision |
7.92 years (+/- 6.22) |
Inter-rater reliability demonstrated consistent facial anthropometric measurements between the two raters. No significant differences were observed in facial measurements of CLEFT-Q survey scores across ethnicity (Caucasian vs. non-caucasian) or gender (Table 2A-2C).
Table 2A: CLEFT-Q Scores by Ethnicity
|
Domain |
Mean Score: Caucasian (Standard Deviation) |
Mean Score: Non- Caucasian (Standard Deviation) |
P-Value |
|
Face |
27.2 (6.4) |
30 (5.8) |
0.376 |
|
Nose |
35.6 (8.7) |
33.8 (9) |
0.696 |
|
Nostrils |
18.3 (5.3) |
15.6 (4.3) |
0.305 |
|
Teeth |
22.5 (7.4) |
22.4 (6.7) |
0.979 |
|
Lips |
27.3 (7.3) |
27.8 (7.7) |
0.902 |
|
Scar |
22.6 (6.1) |
22.2 (5.5) |
0.891 |
|
Jaws |
23.5 (5) |
22.2 (4.2) |
0.65 |
|
Speech Function |
29.8 (5.1) |
31.5 (4.2) |
0.554 |
|
Speech Distress |
27.9 (2.6) |
28.2 (2.9) |
0.834 |
|
Psychiatric Distress |
34.1 (6.1) |
36.8 (4.6) |
0.428 |
|
School |
34.8 (5.1) |
34.5 (4.2) |
0.911 |
|
Social |
34.9 (4.7) |
34.5 (6.2) |
0.894 |
|
Eating/Drinking |
32.6 (5) |
35.8 (0.5) |
0.226 |
|
Total Raw Score |
303.1 (139.4) |
330.6 (125.1) |
0.691 |
Table 2B: Summary of Correlation analysis of CLEFT-Q Scores and Age at Cleft Revision
|
Domain |
R2 Value |
P-Value |
|
Face |
-0.05 |
0.807 |
|
Nose |
-0.31 |
0.144 |
|
Nostrils |
-0.21 |
0.327 |
|
Teeth |
-0.06 |
0.796 |
|
Lips |
-0.36 |
0.095 |
|
Scar |
-0.47 |
0.031* |
|
Jaws |
-0.02 |
0.936 |
|
Speech Function |
0.19 |
0.422 |
|
Speech Distress |
-0.1 |
0.682 |
|
Psychiatric Distress |
-0.32 |
0.159 |
|
School |
-0.21 |
0.372 |
|
Social |
0.13 |
0.596 |
|
Eating/Drinking |
-0.13 |
0.585 |
|
Total Raw Score |
0 |
0.984 |
Table 2C: CLEFT-Q Scores by Sex
|
Domain |
Mean Score: Female (Standard Deviation) |
Mean Score: Male (Standard Deviation) |
P-Value |
|
Face |
26.6 (7.2) |
28.7 (5.4 |
0.433 |
|
Nose |
33.4 (9.1) |
36.8 (8.2 |
0.346 |
|
Nostrils |
16.3 (5.9) |
19.1 (4.2) |
0.198 |
|
Teeth |
19.4 (6.7) |
25.3 (6.5) |
0.042* |
|
Lips |
25.5 (8.5) |
29.2 (5.7) |
0.237 |
|
Scar |
20.7 (6.2) |
24.5 (5) |
0.143 |
|
Jaws |
22.1 (4.7) |
24.2 (4.9) |
0.308 |
|
Speech Function |
29.8 (5) |
30.5 (5.1) |
0.769 |
|
Speech Distress |
27.9 (2.5) |
28.1 (2.7) |
0.869 |
|
Psychiatric Distress |
34.2 (6.5) |
35 (5.3) |
0.761 |
|
School |
35.2 (6.1) |
34.3 (3.4) |
0.688 |
|
Social |
35.4 (5.5) |
34.2 (4.3) |
0.592 |
|
Eating/Drinking |
34 (2.6) |
32.4 (6.1) |
0.453 |
|
Total Raw Score |
340.6 (92.2) |
284.8 (158) |
0.306 |
Sex was significant in the context of teeth scores (p=0.042), with female participants reporting lower satisfaction with the appearance of their teeth than males. Age showed a moderate inverse correlation with scar scores (R2 -0.47, p=0.031) among both males and females and across all ethnicities.
DISCUSSION
This case series aimed to characterize and analyze patient satisfaction among the patient population treated by an academic multidisciplinary cleft and craniofacial team using the internationally validated CLEFT-Q survey [1].
The field of otolaryngology/ head and neck surgery at large has openly welcomed and appreciated the use of Patient Reported Outcome Measures (PROMs). This has been seen in rhinology through various quality of life measurements such as the Rhinitis Quality of Life questionnaire and the 22 Item Sinonasal Outcome Test. Both of these PROMs have proven to support clinical decision making before surgical intervention and in evaluating patient management post intervention [2]. Additionally, the Nasal Obstruction Symptom Evaluation (NOSE) and Standardized Cosmesis and Health Nasal Outcomes Survey (SCHNOS) scores have been popularized in the characterization of post-operative clinical course for patients who undergo functional as well as cosmetic septorhinoplasty. Beyond rhinology, PROMs have established utility in assessing upper airway-related dyspnea through the Medical Research Council (MRC) Dyspnea scale, the Clinical Chronic Obstructive Pulmonary Disease Questionnaire (CCQ), and the Dyspnea Index (DI) [3].
It has been long established that successful treatment of patients with orofacial clefts exceeds provider-based structural and functional repair. It entails the patient’s intrinsic, psychological, and social satisfaction with their individual clinical outcome, implying the necessity to standardize PROMs in cleft repair surgery and pediatric otolaryngology as a whole. Among the patients who participated in our case series, sex and age emerged as important factors in shaping patients’ CLEFT-Q scores and overall satisfaction highlighting the strong impact of societal influences on patients with orofacial clefts. Additionally, while our study did not identify statistically significant differences in the facial anthropometrics of patients of various ethnicities, likely due to our small sample size, the concept of ethnic congruence in cleft repairs is important and imminent. Racial and ethnic differences must be considered in order to achieve an ethnically congruent aesthetic outcome for the patient [4].
There were inherent limitations to the study, including limited sampling and parental/child dynamics which may have biased patients’ responses towards the opinions of guardians (if they were developmentally delayed or unable to complete the survey on their own). There is potential for our results to be reflective of combined patient and parent satisfaction as was obtained and examined in other studies completed among populations of patients with orofacial clefts, as noted in prior studies [5].
This case series re-iterates the importance of considering holistic patient satisfaction, such as the feedback expressed through patient reported survey tools, when evaluating surgical outcomes. In orofacial cleft care, there is sufficient supporting evidence to suggest that PROMs such as the CLEFT-Q survey should be implemented as central tenets of patient satisfaction following otolaryngologic surgical intervention.
REFERENCES
- Klassen AF, Riff KWW, Longmire NM, Albert A, Allen GC, Aydin MA, et al. Psychometric findings and normative values for the CLEFT-Q based on 2434 children and young adult patients with cleft lip and/or palate from 12 countries. CMAJ. 2018; 190: E455-E462.
- Dykewicz MS, Wallace DV, Bandi S, Mahdavinia M, Sedaghat AR. Patient-Reported Outcome Measures in Rhinitis and Chronic Rhinosinusitis. J Allergy Clin Immunol Pract. 2024; 12: 2574-2582.
- Noud M, Hovis K, Gelbard A, Sathe NA, Penson DF, Feurer ID, et al. Patient-Reported Outcome Measures in Upper Airway-Related Dyspnea: A Systematic Review. JAMA Otolaryngol Head Neck Surg. 2017; 143: 824-831.
- Harrison LM, Cole NA, Derderian CA, Hallac RR. Three-dimensional Anthropometric Analysis of Racial and Ethnic Differences in Unilateral and Bilateral Cleft Nasal Deformity. Cleft Palate CraniofacJ. 2024; 61: 1308-1314.
- Ranganathan K, Kochkodan JM, Baker MK, Matusko N, Bennett KG, Shapiro DN, et al. Variation in the Desire for Cleft Revision Surgery among Children, Caregivers, and Surgeons. Plast Reconstr Surg. 2019; 144: 171-178.








































































































































