Intraluminal Silastic Tube for Multiple Segment of Bowel Anastomosis in Midgut Volvulus: An Alternative Approach to Preserve Bowel Length
- 1. Department of Surgery, Ministry of Health, Malaysia
- 2. Department of Pediatric Surgery, Ministry of Health, Malaysia
Abstract
Short bowel syndrome is a known complication following long segment resection for intestinal ischaemia secondary to midgut volvulus and associated with much morbidity. Preserving the maximal bowel length by removing only the gangrenous bowel segments is an ideal solution but hindered by time consuming anastamosis. Even though there are various anastomotic methods been studied, auto-anastamosis of bowel as in our has never been described for malrotation. This is the first report of a novel technique utilising intraluminal silastic tube to promote spontaneous bowel anastamosis following multiple segmental resection in a patient diagnosed as midgut volvulus. This is a safe technique to avoid morbidities associated with short gut syndrome in paediatric population.
Keywords
• Midgut volvulus
• Short bowel syndrome
• Bowel Anastomosis
Citation
Aimanan K, Othman MY, Abdullah MY, Zahari Z (2018) Intraluminal Silastic Tube for Multiple Segment of Bowel Anastomosis in Midgut Volvulus: An Alternative Approach to Preserve Bowel Length. JSM Pediatr Surg 2(2): 1016.
INTRODUCTION
Malrotation with midgut volvulus can give rise to catastrophe if delayed recognition and leads to extensive bowel resection thus high incidence of short gut syndrome.
The concept of splinting the bowel with silastic tube to avoid resection has been contemplated long time ago. Literature review showed total number of nine cases of utilisation of the transluminal stent in preserving maximal bowel length in multiple atresia and necrotising enterocolitis. There were no reports on utilisationof similar technique for midgut volvulus.
In our case, we are applying the similar concept in order to achieve a reasonable small bowel length after segmental resection of gangrenous bowel secondary to volvulus to avoid short bowel syndrome.
CASE REPORT
A day ten of life baby boy, borderline premature at 36 weeks with weight of 2.47 kgs was referred to our centre with history of bilious vomiting and upper abdominal distension followed by per rectal bleeding. Clinical examination revealed an ill, dehydrated child with distended abdomen. Patient was acidotic and an abdominal x-ray showed very limited distal bowel gas.
Laparatomy was performed after optimisation and stabilisation of patient’s condition. Intraoperative finding was 360 degree volvulus with multiple segment of unhealthy bowel, which extending from proximal jejunum until terminal ileum. There was a single perforation noted 6cm away from ileocaecal valve which was repaired primarily. Abdomen was closed and planned for relaparatomy after correction of physiologic parameters. Relaparatomy was performed after 40 hours revealed multiple segments gangrenous bowel along the small bowel. Decided to salvage maximal bowel length intra op. Multiple segments resected and anastamosedloosely at three points to orientate them (7 segments of bowel) (Figure 1).
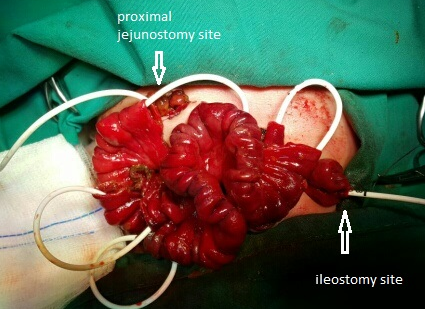
Figure 1 Intraluminal silastic stent used to align the bowel segments.
Proximal jejunostomy and distal ileostomy created. A VYGON tube was threaded through the lumen of bowel segments and proximal end brought out through jejunostomy and distal and through ileostomy.
Post operatively the patient was continued on total parenteral nutrition. He was started on trophic feeding a week after surgery. At 3rd week post op patient developed deranged liver function likely secondary to prolonged total parenteral nutrition. During this course we have withheld the parenteral feeding and started feeding through proximal jejunostomy. On day 36 contrasts study through the intraluminal silastic tube, revealed complete anastomosis of bowel segments. Patient underwent proximal jejunostomy closure on day 42 of life. Oral feeding was established on day 46 and subsequently TPN was withheld. The distal ileostomy closure was carried out on day 77 of life. Patient was started on regular breast feeding and noted a slow weight gain. He was discharged on day 116 of life (post op day 96) and given a regular clinic follow up. He is showing a good progress during follow up of 2 years and no hospitalisation required for malnutrition.
DISCUSSION
Short gut syndrome, and the need for bowel preservation
Short bowel syndrome (SBS) is a malabsorptive state occuring as a result of surgical resection or congenital disease of a significant portion of the small intestine [1]. Looking at the magnitude of this problem surgical techniques need to be revolutionised in order to primarily tackle short bowel syndrome.
Intraluminal silastic stent has been described in literature for multiple intestinal atresias and necrotising enterocolitis. This is the first time this technique utilised for malrotation. The aim of this approach is to preserve maximal bowel length by resecting only completely non-viable tissues and allowing a spontaneous bowel anastamosis.
Intestinal malrotation
Intestinal malrotation occurs because of failure of the normal sequence of rotation and fixation of the bowel. Midgut volvulus can lead to irreversible intestinal necrosis, which is potentially fatal.
Technique highlights
Primary anastomosis of all the bowel segments is time consuming which can be avoided in this technique. However we still applied three sutures at both lateral walls and antimesentric border in order to maintain the long axis of bowel. Lessin et al., has described a similar technique without using any sutures (Table 1) [2].
Table 1: Description of previous reports on use of intraluminal silastic tube for necrotising enterocolitis after multiple segmental resections.
| In our case | Other case | |
| Weight gain | 2.47 2.67kg | |
| TPN duration | 46 days | Lessin MS et al - 150 months Rodrigo L.P. et al - 149 days Sapin E et al - 90 days |
| Vygon tube duration | 42 days | Lessin MS et al - 3months Rodrigo L.P. et al - not available Sapin E et al - Not available |
| Complication | - Sepsis possibilydue to bacterial translocation - TPN induced liver function derangement |
- anastomosis leak - stricture - additional procedures (serial transverse enteroplasty and tapering enteroplasty). |
| Feeding establishment | Day 21 | Lessin MS et al - Not available Rodrigo L.P. et al - day 17 Sapin E et al - Not available |
| Residual length of small intestine | 75 cm | Lessin MS et al - 25cm RyglM et al - 50 cm Rodrigo L.P. et al - Not available Sapin E et al - 95cm |
| Duration of stay | 4 months | Lessin MS et al - 5 months RyglM et al - 5 months Rodrigo L.P. et al - Not available Sapin E et al - Not available |
| Number of sutures applied | 3 sutures | Lessin MS et al – no sutures Rodrigo L.P. et al – 4 sutures Sapin E et al – Not available |
We believe at least few sutures should be applied to maintain the bowel axis to prevent rotation of segments.
Issues
There are few problems we observed post operatively in this patient such as sepsis (possibly secondary to bacterial translocation) and total parenteral nutrition induced deranged liver function test. None of the previously reported papers have discussed regarding this problems [3]. Stricture of anastomotic segments was described in two studies, which require endoscopic stricturoplasty (Table 1).
A mean duration of 31 days was described in literature for removal of Vygon tube following contrast study. We hope in future the duration maybe be shortened with more experience in managing similar condition [4,5]. This will enable starting full feeding early and reduce duration of total parenteral nutrition.
CONCLUSION
Intraluminal silastic tube to promote autoanastamosis of bowel is a safe method and should be widely used in multiple segment bowel perforations to prevent morbidities associated with short gut syndromes.









































































































































{kind=link}