Multicystic Paradidymis: A Rare Incidental Finding during Pediatric Inguinal Hernia Repair
- 1. Division of Urology, American University of Beirut-Medical Center, Lebanon
- 2. Division of Urology, Beirut Arab University, Lebanon
Abstract
Paradidymis, or the organ of Giraldes, is a rather uncommon paratesticular appendage that has been very infrequently clinically reported and remains a drawing in textbook illustrations. This is the first report on an incidental presentation of a multicystic paradidymis encountered during a pediatric hernia repair.
Keywords
• Paradidymis
• Testicular appendage
• Hernia repair
• Pediatrics
Citation
El-Hout Y, El-Jaam MR (2018) Multicystic Paradidymis: A Rare Incidental Finding during Pediatric Inguinal Hernia Repair. JSM Pediatr Surg 2(1): 1010.
CASE PRESENTATION
A 3 year old boy presented with a right inguino-scrotal painless bulging mass, typical on physical examination for a right indirect inguinal hernia. By history, he had intermittent left scrotal swelling suggestive of a communicating hydrocele. The family was consented for bilateral inguinal exporation and repair of inguinal hernia/ ligation of sac. On the right side, a standard inguinal incision was made and the inguinal canal was opened. A 3.5 cm inguino-scrotal sac was carefully dissected and delivered through the inguinal incision in continuity with the spermatic cord. The sac was consistent with a non-communicating hydrocele with a hernia sac proximal to it. The sac was carefully dissected off the spermatic cord and suture-ligated at the level of the internal ring. The tunica vaginalis of the non-communicating was incised with care not to injure the testicle inside. Around 20 milliliters of clear fluid was drained and the testicle was delivered. Proximal to the epididymis, an unusual structure was encountered with cluster of 3-4 cysts of variable sizes, the largest measuring 1.5 cm, (Figure 1).
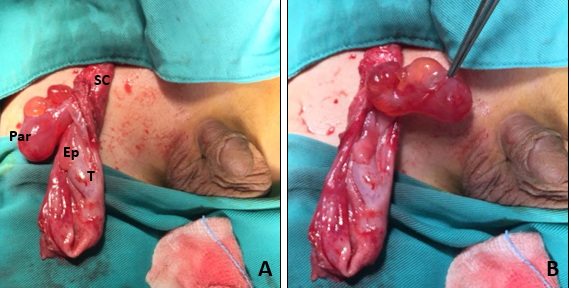
Figure 1 (A) Inguinal exposure showing T: Testicle, Ep: Epididymis, SC: Spermatic cord, Par: Multicystic paradidymis with cluster of cysts of variable sizes. (B) Note pedunculated nature of paradidymis.
The multicystic structure had no visible continuity with the vas deferens. Its location was in keeping with a paradidymis. The dominant cyst was incised and clear fluid was drained. The whole structure was excised and submitted to pathology. The cysts had mesothelial lining and no malignancy was reported. Exploration of the contralateral side revealed a communicating hydrocele and inguinal ligation of a persistent patent processus vaginalis was done.
DISCUSSION
Testicular appendages are anatomical remnants of the upper portion of the paramesonephric (Mullerian) duct persisting after its degradation under the effect of Mullerian-Inhibiting Substance (MIS) during fetal life after 6th week of gestation [1]. Portion of the mesonephric (Wolffian) duct cranial to the testicle is the origin of other appendages, namely, epididymal appendages and paradidymal appendages (organ of Giraldes). Appendages have been described as classified by Favorito et al. [2], (Figure 2).
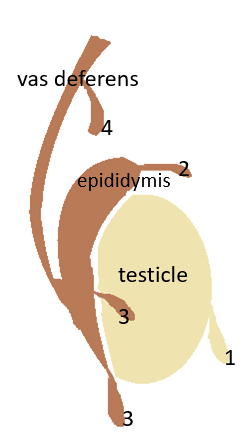
Figure 2 (1) Testicular appendage, (2) Epididymal appendage, (3) Appendage aberrans of Haller, (4) Paradidymis (organ of Giraldes).
In a study by Sahni et el. [3], that looked into paired testis in medicolegal autopsies of 425 adults, 50 children and 10 neonates, testicular and epididymal appendages were seen in 83.3% and 20%, respectively. No literature is available on the actual incidence of paradidymis except for scarce case reports. A single study on torsion of an organ of Giraldes, arising from the distal spermatic cord and presenting as acute scrotum is reported [4]. Another study [5] encountered two tubular structures, distinct from vas, during subinguinal varicocelectomy in a 30 year old infertile man. The structures were lined with ciliated pseudostratified epithelium. Our study is the first to report on a multicystic presentation of a paradidymis, distinct from the vas deferens, without any malignant features. Excision of the paradidymis abolishes the potential risk of future torsion. Given the benign nature of paradidymis, testicular sparing is always to be considered.
CONCLUSION
This case report describes and photographically illustrates a presentation of a rare surgical entity, namely a paradidymis, encountered during a routine hernia repair in a child. This serves to broaden our understanding and appreciation of intricate inguinoscrotal anatomy.









































































































































{kind=link}