Trichobezoar Causing Intussusception in a Boy : A Case Report
- 1. Department of pediatric surgical emergencies, Mohamed V University, Morocco
Abstract
Trichobezoar is an uncommon but potentially serious cause of abdominal pain in children. It is an unusual cause of gastric outlet obstruction, bleeding, intussusception and perforation in the Pediatric Emergency Department. We present a case of trichobezoar causing intussusception in a healthy, developmentally-normal boy in Morocco. It was treated successfully with surgery followed by psychiatric consultation. The patient’s abdominal symptoms subsided after the bezoars were eliminated; no subsequent gastrointestinal events occurred in the following months
Keywords
• Trichobezoar
• Intussusception
• Child
Citation
Oudrhiri M, Zerhouni H, Oubejja H, Ettayebi F (2018) Trichobezoar Causing Intussusception in a Boy : A Case Report. JSM Pediatr Surg 2(1): 1009.
INTRODUCTION
Trichobezoar is a very rare entity. It is an unusual condition in which hair bundle in the stomach and small intestine. They are related to mental disorders and usually form in a healthy stomach. The clinical presentation is varied and ranging from chronic abdominal pain to gastric perforation. Its early diagnosis is necessary to combat complications. They are a described potential cause of atypical intussusception in children [1]. Most cases of trichobezoar are reported in females, which may be attributed to the traditional long hair. This case report is unusual in that the patient was male and this condition is revealed by an intestinal intussusception and such cases are rarely reported in medical literature. After chirurgical treatment of trichobezoar, a psychiatric evaluation of the patient should be considered to get to the root cause of the problem.
CASE PRESENTATION
A healthy fifteen-year-old school boy was referred to Rabat Children’s Hospital. He had a two-week-history of paroxysmal abdominal pain with vomiting without diarrhea or rectorrhagia. The child had been noted to be losing appetite. He was developmentally appropriate and had no other medical or surgical history. Family history was unremarkable. On examination the child was well built, no sign of malnutrition was apparent and there was no alopecia. He had sparse short hair. Abdomen was distended without palpable mass.
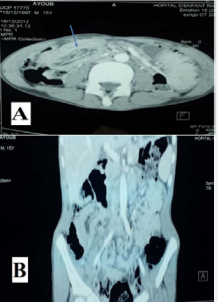
Routine blood investigations were within normal limits. An abdominal ultrasound revealed minimal effusion. A tomographic scan of the abdomen was performed, revealing intestinal intussusception (Figure1).
 \
\
Figure 1 A slice of a computed tomography (CT) scan of the abdomen and pelvis of the patient, with IV contrast, demonstrating intussusception. A: sagittal section, B: coronal section.
The patient was taken to the operating room, laparoscopy was the initial procedure, but it was converted into laparotomy when a trichobezoar was encountered. The surgeon first attempts to reduce the intussusception, the intestine was viable then the segment of bowel with hair ball was exteriorized and enterotomies were performed for extraction.
The trichobezoar weighed 40 g and was 3 cm long (Figure 2,3).

Figure 2 INTRAOPERATIVE photograph demonstrating trichobezoar enclosed in the intestinal lumen.

Figure 3 Enterotomy allowing extraction of the trichobezoar connected by a wire.
His postoperative course was uneventful. He admitted that he liked eating hair. The patient was referred to a psychiatrist for treatment of trycophagia.
DISCUSSION
Bezoars are a rare and fascinating entity that can cause gastric and small bowel obstructions. Several types have been reported. The classification of bezoars depends on their composition: trichobezoar includes hair; phytobezoar, vegetable matter such as skin, seeds, and fiber; lactobezoar, undigested milk curd; and lithobezoar, mud and stones [2].
Trichobezoars make up 55% of all bezoars: 90% occur in adolescent females, probably as a consequence of their long hair, though they may occur in both sexes and have also been described in the new born [3].
They are usually associated with underlying psychiatric disorders, such as depression, obsessive-compulsive disorder, body dysmorphic disorder and, particularly, trichotillomania [4, 5].
The clinical presentation of trichobezoar is usually delayed, after ingestion of large amount of hairs over many years.
Trichobezoars are an uncommon cause of acute abdominal pain. They may undergo complications. Apart from intussusception, other complications reported in unrecognized trichobezoars are obstructive jaundice, protein losing enteropathy, pancreatitis and even death [6].
Most patients present with abdominal pain, nausea, and vomiting; therefore, it is an important diagnosis to consider in this setting. They can even rarely cause peritonitis and perforation [7-9]. The clinical scenario is most common in teenage girls with the diagnosis in a child very rare. Various modalities are used for diagnosis of this rare condition.
The recommended treatment for large or complicated trichobezoars is surgical. After removal of the trichobezoar, the stomach and bowel should be inspected carefully for evidence of perforation and palpated for any residualbezoar.
In addition to the acute surgical treatment for a trichobezoar, psychiatric consultation is crucial to prevent relapses and to treat comorbid conditions that usually accompany this disorder.
CONCLUSION
Trichobezoars causing intussusception intestine is rare and need to be kept in mind in the differential diagnosis of young patients. However, the diagnosis remains difficult when the notion of trichophagia has not been mentioned. If it is diagnosed early and treated successfully, causes no significant complication. However, psychiatric assessment will form an integral form of treatment as recurrences have been described.
CONSENT OF PATIENTS
Written informed consent was obtained from the patient’s next of kin for publication of this case report and any accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal.









































































































































{kind=link}