Cancer Rehabilitation
- 1. Prain Medical Center, Bucharest, Romania
INTRODUCTION
Head and neck cancers are diseases with major debilitation, loss of anatomical structures and/or organ functions concentrated at this level, causing notable dramas - loss of part or all of the tongue, loss of part of the mandible, loss of an eye, a pavilion auricular, of the nasal pyramid, interferes with the alteration of the physical appearance corresponding to the notion of stuttering, with the loss of speech, mastication, swallowing, being improved or even corrected by reconstructive techniques and / or prosthetic rehabilitation. Such a patient is condemned to the absence of a minimal social life.
The multimodal treatment of cancer obliges the oncological surgeon and to the same extent the plastic surgeon - oncologist to perform operations and/or reconstructions before or immediately after chemotherapy.
The timing of the reconstruction (immediate or late) is also very important and the treatment planning is done in the team, appreciating [1] that the immediate reconstruction is preferable to the late one.
Immediate reconstruction techniques [2] are recommended for patients whose oncological surgery has excised a part of their body.
The advantages for the patient are obvious:
- can no longer bear a new surgical intervention;
the psychological impact of the mutilations is diminished or even eliminated. The patient returns to social activity quickly and with minimal or faded deformities.
- the cost / benefit ratio is better, the cost of waiting being higher than the cost of action.
The most feared disadvantage is the possible masking of a tumor remnant and the prolongation of the operating time.
Tumors of the nose (nasal pyramid) that develop on lupus lesions - are recurrent, reaching progressive mutilations [3]. Surgical reconstruction is allowed only after a while. Until then, nasal prosthesis is recommended.
Oral-maxillofacial prosthetic rehabilitation benefits from an important number of situations [1] in which immediate reconstructions are useful - oral cavity, mandible, nose, upper jaw (including orbit), cervical esophagus, auricle, integuments are recommended for immediate reconstruction .
The impact of mutilating head and neck resections on thepatient’s psychological profile and on his relationships with family and society can be mitigated by these immediate reconstruction techniques. We must not neglect possible inconveniences of immediate reconstruction [4] bearing in mind the following:

Figure 1 Tumors of the nose.
![Figure 2 Carcinoma of the nasal pyramid [1].](https://www.jscimedcentral.com/public/assets/images/uploads/image-1705924621-1.png)
Figure 2 Carcinoma of the nasal pyramid [1].

Figure 3 Carcinoma of the jaw with extension.
- it is not easy to plan such a complex intervention;
- a possible previously undetected tumor extension (imaging is not infallible) determines a replanning of the reconstruction;
- possibly postpone the chemotherapy, exactly planned by the oncology team;
- amine irradiation;
- cases with the potential for immediate relapse or the possibility of developing early metastases will “reconstruct” late, hence the role of diagnostic techniques.
Arguments in favor of late surgery; an extensive excision surgery can be performed, considered unfeasible until the adoption of reconstruction techniques.
Nasal sinus tumors can be benign and malignant (sarcomas: round cells, fibrosarcomas and lymphosarcomas, osteogenetic sarcomas).
Surgical treatment of malignant nasal tumors consists of total tumor ablation, pre- and post-operative roentgen therapy and cytostatic chemotherapy.
Favorable results only if applied very early.
Tumors of the paranasal sinuses can be benign or malignant.
Benign tumors are represented by the amyloid tumor of the ethmoid; frontal sinus meningioma; ethmoid mucocele; osteomas that appear only at the end of childhood.
The surgical treatment consists in extirpation of the tumor by the endo or exonasal route. If the ablation is complete, these tumors do not recur.
Malignant tumors: sinus neoplasias are tumors of the mesostructure, they are usually located in the jaw and consist of: round cell sarcomas; lymphoblastic sarcomas; fibrosarcoma; osteogenetic sarcomas.
The treatment differs with the structure of the tumor:
- Fibroblastic and osteogenetic sarcomas are radioresistant and can only be cured by early and radical surgery
- Round cell sarcomas and lymphosarcomas are sensitive to Roentgentherapy, but the yield is only transient.
Tumors of the ethmoid:
- Epitheliomas;
- Conjunctival tumors-sarcomas, finbrosarcomas, lymphosarcomas, reticulosarcomas, plasmacytoma, nerve tumors;.
Tumors of the lower floor of the nasal cavities:
- Malignant tumors of the nasal septum;
- Tumors of the inferior turbinate;
-Special tumors; fibrosarcoma, lymphosarcoma, cylindromas and melanomas.
Tumors of the upper jaw;
![Figure 4 Carcinoma of the jaw with extension to the orbit; Mandibular carcinoma [1].](https://www.jscimedcentral.com/public/assets/images/uploads/image-1705924936-1.png)
Figure 4 Carcinoma of the jaw with extension to the orbit; Mandibular carcinoma [1].
![Figure 5 Neoplasm of the palatine wave – operated [1]](https://www.jscimedcentral.com/public/assets/images/uploads/image-1705924948-1.png)
Figure 5 Neoplasm of the palatine wave – operated [1]
Of the superstructure (ethmoid tumors); - of the mesostructure (maxillonasal);
Tumors of the lower jaw = mandible, are benign and malignant, isolated or with extension to the surrounding tissues. - palatal wave cancer [5].
CITATION
Elena L (2022) Cancer Rehabilitation. JSM Physical Med Rehabil 6(1): 1019.
CASE 1
V.O., 62 years old, diagnosed with carcinoma. An upper and lower obturator, with teeth, was made in the prosthetic reconstructions of the central facial region, in the left hemimaxillectomy, with total rhinectomy and resection of 1/3 of the hard palate. Using titanium magnets, the dental obturator also serves to secure and solidify the silicone facial epitheses, with another upper attachment point on the glasses.
CASE 2
Prosthetic reconstruction of the mandible.
Mandibular neoplasm.
D.N., Bucharest. After resection of the body of the mandible,an attempt was made to reconstruct the mandible with silicone, fixed with adhesive to the remaining integument and also supported by a lower dental prosthesis, with teeth, but the prosthesis was not completed, due to the death of the patient due to lung metastases and cardio-respiratory arrest.
CASE 3
Diagnosis of melanoma of the lower eyelid, with invasion of the orbit, eye. After the exenteration of the orbit and the eyeball, the reconstruction of the orbit + eyes made of silicone and acrylate was done. Fixation with local anatomical means. Very good aesthetic and psychological results.
![Figure 6 Lower dental prosthesis, with teeth [1].](https://www.jscimedcentral.com/public/assets/images/uploads/image-1705925274-1.png)
Figure 6 Lower dental prosthesis, with teeth [1].
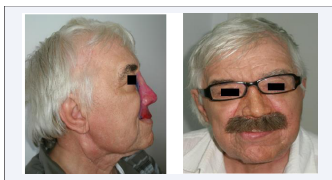
Figure 7 Invasion of the orbit, eye.

Figure 8 Aesthetic and functional reconstruction.
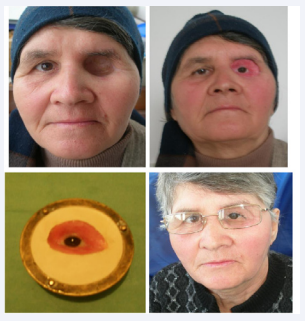
Figure 9 The reconstruction of the orbit + eyes.
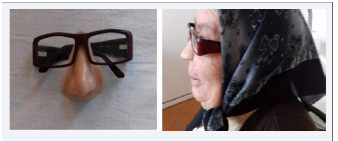
Figure 10 Silicone facial epitheses, with another upper attachment point on the glasses.

Figure 11 Orbit with medical silicone + acrylate eyeball + eyelashes, natural hair eyebrows.

Figure 12 Surgical reconstruction
CASE 4
Maxillary sinus cancer with invasion of the orbit and nasal pyramid - right hemi-face reconstruction, orbit with medical silicone + acrylate eyeball + eyelashes, natural hair eyebrows, fixation with medical adhesive or titanium implants, Branemark method.
CONCLUSIONS
Surgical reconstruction of the nasal pyramid with the multitude of surgery techniques, despite accidents or postoperative complications, is a useful technique in the aesthetic and functional reconstruction of the central region of the face.
- It worth mentioning the modern technique of surgical prosthetic reconstruction in cases of large loss of substance, when the common surgical procedures are inefficient.
- Silicone and titanium implants are well tolerated by the human body, without being toxic or allergic.
- Aesthetic role –the patient regains a normal appearance by restoring the normal anatomy of the respective area.
- Functional role-in breathing , mastication, phonation, hearing.
- Psychological implications in socialization and improvement of the quality of life.
REFERENCES
1. Latcan Elena. Surgical reconstruction - oro-maxillo-facial prosthetic rehabilitation. Doctoral Thesis. Romania, 2012.
3. Thomas KF. Prosthetic Rehabilitation. Quintesance Publishing Co. 1994; 93-103.
4. Thomas KF. The art of clinical Anaplstology.Thomas Publishing. 2006.
5. Meenakshi A, Shah D. The obturator prostheses for maxillectomy. SRM J Res Dent Sci. 2012; 3: 193-7.









































































































































{kind=link}