Anterior Vaginal Wall Augmentation using Cross-Linked Hyaluronic Acid versus Platelet Rich Plasma: A Prospective Pilot Study Assessing Female Sexual Function
- 1. Obstetrics and Ginecology Service, Vithas Universitary Hospital Las Palmas, Atlantico Medio University, Spain
Abstract
Background: Augmentation of the anterior vaginal wall, commonly referred to as G-spot amplification (GSA), has gained increasing interest as a minimally invasive procedure aimed at improving female sexual satisfaction. Injectable therapies such as cross-linked hyaluronic acid (HA) and platelet-rich plasma (PRP) have been proposed for this purpose; however, comparative clinical data evaluating sexual outcomes remain limited.
Objective: To compare the impact of anterior vaginal wall augmentation using cross-linked HA versus PRP on female sexual function, assessed using the Female Sexual Function Index (FSFI). Methods: A prospective comparative pilot study was conducted including 16 sexually active women undergoing anterior vaginal wall augmentation. Patients were allocated into two groups: a HA group (n = 8) treated with cross-linked HA (Armonía®) and a PRP group (n = 8) treated with autologous PRP. Sexual function was evaluated using the FSFI questionnaire at baseline and at 3 months post-treatment. Changes in total FSFI scores and domain-specific outcomes were analyzed within and between groups.
Results: Both treatment groups demonstrated statistically significant improvements in total FSFI scores compared with baseline. The HA group showed a mean improvement exceeding 68%, with particularly notable gains in desire, arousal, and orgasm domains. The PRP group also exhibited significant improvement, although to a slightly lesser extent. Between-group comparison revealed a statistically significant difference favoring HA treatment (p < 0.05). No major adverse events were reported.
Conclusion: Anterior vaginal wall augmentation using both cross-linked HA and PRP appears to be a safe and effective minimally invasive approach to enhance female sexual satisfaction. HA demonstrated a greater short-term improvement in FSFI scores, although PRP also provided meaningful clinical benefits. Larger randomized controlled studies with longer follow-up are warranted.
Keywords
• G-spot augmentation
• Female sexual function
• Hyaluronic acid
• Platelet-rich plasma (PRP)
• FSFI (Female Sexual Function Index)
Citation
Barber MA, Eguiluz I (2026) Anterior Vaginal Wall Augmentation using Cross-Linked Hyaluronic Acid versus Platelet-Rich Plasma: A Pro spective Pilot Study Assessing Female Sexual Function: A Pilot Study. JSM Sexual Med 10(1): 1174.
INTRODUCTION
Female sexual dysfunction is a multifactorial condition influenced by anatomical, physiological, psychological, and relational factors. In recent years, minimally invasive genital aesthetic and functional procedures have gained attention as potential therapeutic options for selected patients seeking improvement in sexual satisfaction [1]. The anterior vaginal wall, commonly associated with the so-called G-spot, has been proposed as a sensitive anatomical region whose stimulation may enhance sexual arousal and orgasmic response [2]. Augmentation techniques aimed at increasing volume and sensitivity in this area have been described using injectable materials, including cross-linked HA and autologous PRP [3]. HA provides immediate volumetric enhancement and mechanical support, whereas PRP is believed to exert its effects through tissue regeneration and neurovascular modulation [4]. Despite growing clinical use, comparative data evaluating sexual outcomes between these two approaches remain scarce. The present study aims to compare the effectiveness of cross-linked HA versus PRP for anterior vaginal wall augmentation using a validated sexual function questionnaire, the FSFI [5].
MATERIALS AND METHODS
Study Design
This prospective comparative pilot study included 16 sexually active women undergoing anterior vaginal wall augmentation with HA or PRP. All participants provided written informed consent prior to study inclusion. The study was conducted at Vithas University Hospital, Las Palmas, between January 2018 and December 2024. The study protocol was reviewed and approved by the institutional Ethics Committee of Vithas University Hospital and was conducted in accordance with the ethical principles of the Declaration of Helsinki and its subsequent amendments. Sexual function was assessed using the validated Spanish version of the FSFI, administered at baseline and at 3 months post-treatment to evaluate changes in sexual function. Quantitative variables are presented as mean ± standard deviation. Within-group comparisons were performed using paired t-tests, while between-group comparisons were conducted using independent-samples t-tests. A p-value < 0.05 was considered statistically significant. Statistical analyses were performed using the Statistical Package for the Social Sciences (SPSS), version 26.0 (IBM Corp., Armonk, NY, USA).
HA Group
With the patient in the dorsal lithotomy position, topical anesthetic lidocaine cream (EMLA®) was applied. The cervix was then visualized using a metallic Pederson speculum with right lateral opening. Following antiseptic preparation, a clockwise rotation of approximately 20 degrees was performed to identify the paramedial periurethral area of the anterior vaginal wall. A total of 2.5 mL of cross-linked HA was injected into the submucosal layer, approximately 2.5 cm posterior and 2 cm lateral to the mid-urethra. Prior to injection, gentle and sustained aspiration was maintained for at least 10 seconds to minimize the risk of intravascular administration and embolic complications [6] (Figures 1and 2).

Figure 1 Injection of 2.5 mL cross-linked hyaluronic acid into the submucosal layer of the anterior vaginal wall, 2.5 cm posterior and 2 cm lateral to the mid-urethra.

Figure 2 Instruments and HA preparation used for submucosal injection in the anterior vaginal wall.
PRP Group
After application of topical anesthetic to the vaginal introitus and clitoris, autologous blood was collected and processed by centrifugation for 8 minutes. Five milliliters of PRP were activated with 0.2 mL of 10% calcium chloride. Four milliliters were injected into the anterior vaginal wall between the urethra and the vaginal wall, and 1 mL was injected into the clitoral cavernous body, following previously described protocols [7] (Figure 3).

Figure 3 Injection of autologous PRP into the anterior vaginal wall and clitoral body.
Outcomes
A total of 16 sexually active women were included and allocated into two treatment groups: the HA group (n = 8) and the PRP group (n = 8). The mean age of the overall study population was 42.9 ± 6.6 years (range: 32–56 years). All participants were sexually active at the time of inclusion and sought treatment for decreased sexual satisfaction. The mean age in the HA group was 43.1 ± 6.4 years (range: 34 56 years), while the mean age in the PRP group was 42.6 ± 6.9 years (range: 32–52 years). No statistically significant differences in age were observed between groups, ensuring adequate demographic comparability at baseline Table 1. The primary outcome was the change in total FSFI score from baseline to 3 months post-treatment. Secondary outcomes included domain-specific FSFI changes (desire, arousal, lubrication, orgasm, satisfaction, and pain). Safety outcomes were assessed through the systematic recording of adverse events. Both groups demonstrated significant improvements in total FSFI scores compared with baseline Table 2. The HA group showed a mean improvement exceeding 68%, whereas the PRP group also exhibited significant, albeit slightly lower, improvement. Between-group analysis revealed a statistically significant difference favoring the HA (p < 0.05) (Figure 4).

Figure 4 Percentage Change in Total FSFI Score at 3 Months. Percentage improvement in total Female Sexual Function Index (FSFI) score at 3 months following anterior vaginal wall augmentation. Patients treated with cross-linked hyaluronic acid showed a mean improvement of 68.1%, whereas patients treated with platelet-rich plasma (PRP) demonstrated a mean improvement of 45.7%. The between-group difference was statistically significant (p < 0.05).
Regarding secondary outcomes, improvement across individual FSFI domains was observed in both treatment groups, with the most pronounced changes noted in arousal and orgasm domains. Overall satisfaction with the procedure was high in both groups, reported in 87.5% of patients in the hyaluronic acid group and 75% in the PRP group (Figure 5).
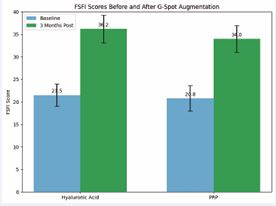
Figure 5 Comparison of FSFI scores at baseline and 3 months after anterior vaginal wall augmentation. Hyaluronic acid and PRP groups both demonstrated significant improvements, with hyaluronic acid showing slightly higher post-treatment scores.
No major adverse events were observed. These findings suggest that anterior vaginal wall augmentation may represent a minimally invasive option to enhance sexual satisfaction in selected patients.
Table 1: Demographic characteristics of study participants.
|
Characterisitc |
HA Group (n=8) |
PRP Gropup (n=8) |
Total (n=16) |
|
Age, years (mean +SD) |
43.1+6.4 |
42.6+6.9 |
42+ 6.6 |
|
Age range, years |
34-56 |
32-52 |
32-56 |
|
Sexually active |
100% |
100% |
100% |
|
Informed conset obtained |
Yes |
Yes |
Yes |
|
Follow-up 3 month |
100% |
100% |
100% |
Data are presented as mean ± standard deviation (range). The study included 16 sexually active women undergoing anterior vaginal wall augmentation, divided into two groups: hyaluronic acid (HA) and platelet-rich plasma (PRP). No statistically significant differences in age were observed between groups, ensuring demographic comparability at baseline.
Table 2: Changes in FSFI Scores After Anterior Vaginal Wall Augmentation Values are presented as mean ± standard deviation.
|
FSFI Outcome |
HA Group (n = 8) |
PRP Group (n = 8) |
p-value (between groups) |
|
Total FSFI - Baseline |
18.2 + 3.1 |
18.6 + 3.4 |
NS |
|
Total FSFI - 3 months |
30.6 + 3.8 |
27.1 + 3.6 |
- |
|
Mean % Improvement |
+68.1% |
+45.7% |
< 0.05 |
|
Desire domain |
↑ Significant |
↑ Significant |
< 0.05 |
|
Arousal domain |
Significant |
↑ Moderate |
< 0.05 |
|
Lubrication domain |
↑ Moderate |
↑ Moderate |
NS |
|
Orgasm domain |
Significant |
↑ Moderate |
< 0.05 |
|
Satisfaction domain |
↑ Significant |
↑ Significant |
NS |
|
Pain domain |
No change |
No change |
NS |
FSFI = Female Sexual Function Index; HA= Hialuronic acid; PRP = Platelet-Rich Plasma; NS = not significant.
DISCUSSION
GSA is a functional intimate procedure consisting of a temporary increase in the thickness of the anterior vaginal wall through filler injection into the vesicovaginal septum, with the aim of enhancing female orgasm during vaginal penetration [8]. The rationale for this approach is based on anatomical and functional studies suggesting that women who experience vaginal orgasms have a thicker urethrovaginal space [9], and that a direct correlation exists between urethrovaginal space thickness and orgasmic capacity [10]. Although there remains considerable controversy regarding both the existence and precise localization of the G-spot [11–16], the majority of contemporary reviews support the concept of a functional clitourethrovaginal complex rather than a discrete anatomical structure [17,18]. Current evidence suggests that increasing anterior vaginal wall thickness may improve sexual function and orgasmic response in selected women [18]. The FSFI represents a validated and objective instrument for assessing changes in female sexual function following therapeutic interventions [5,19]. Several techniques have been described to increase anterior vaginal wall thickness, including injections of HA, autologous PRP, and autologous fat [20–22]. Comparative studies evaluating HA acid and PRP for vulvovaginal conditions have demonstrated both treatments to be safe and effective, with some evidence suggesting superior FSFI improvement and vaginal wall thickening following HA injection [23]. PRP has also been described as an effective treatment for female sexual dysfunction, with multiple studies reporting significant improvements in FSFI scores following PRP injections into the anterior vaginal wall [24,25]. Combination therapies involving HA and PRP in the genital and perineal region have also been reported, showing high patient satisfaction and favorable safety profiles [22,26]. To date, no randomized or controlled trials have specifically evaluated GSA using HA or PRP with FSFI as the primary endpoint.
FINDINGS
The present study contributes comparative prospective data using a validated questionnaire, although it is limited by small sample size and short follow-up. Both treatment modalities resulted in clinically meaningful improvements in FSFI scores. The HA group demonstrated a greater than 68% improvement from baseline, particularly in arousal and orgasm domains. This may be explained by the immediate volumetric and mechanical effect of cross linked HA, enhancing anterior vaginal wall stimulation during intercourse. PRP also produced significant improvement, although to a slightly lesser extent, possibly reflecting its regenerative mechanism, which may require longer follow-up to reach maximal efficacy. No significant complications were observed, supporting the safety of both procedures when performed by experienced clinicians.
CONCLUSION
Anterior vaginal wall augmentation using cross-linked HA and PRP appears to be a safe and effective minimally invasive approach to enhance female sexual satisfaction. Both treatments resulted in significant improvements in FSFI scores, with HA demonstrating a statistically greater short-term benefit. PRP also provided meaningful improvement and may represent a regenerative alternative. Larger randomized controlled studies with longer follow-up are needed to confirm these findings and to better define long-term outcomes.
REFERENCES
- Furnas HJ, Canales FL, Pedreira RA, Comer C, Lin SJ, Banwell PE. The Safe Practice of Female Genital Plastic Surgery. Plast Reconstr Surg Glob Open. 2021; 9: e3660.
- Kilchevsky A, Vardi Y, Lowenstein L, Gruenwald I. Is the female G-spot truly a distinct anatomic entity? J Sex Med. 2012; 9: 719-726.
- Panicker R, Pandurangan T. Cosmetic surgical procedures on the vulva and vagina - an overview. Indian J Med Ethics. 2022; VII: 1-9.
- D’Agostino A, d’Agostino M, Nardini M, Muraglia A, Di Meo C, Mastrogiacomo M, et al. Novel platelet-rich plasma/ hyaluronic acid lyophilized formulations for wound healing applications. Front Bioeng Biotechnol. 2025; 13: 1619633.
- Rosen R, Brown C, Heiman J, Leiblum S, Meston C, Shabsigh R, et al. The Female Sexual Function Index (FSFI): a multidimensional self- report instrument for the assessment of female sexual function. J Sex Marital Ther. 2000; 26: 191-208.
- Kong J, Yang T, Yang X, Zhang F, Liao X, Li D. Death from Pulmonary Embolism Caused by Vaginal Injection of Hyaluronic Acid: a Case Report and a Literature Review. Aesthetic Plast Surg. 2023; 47: 1535- 1541.
- Runels C, Melnick H, Debourbon E, Roy L. A pilot study of the effect of localized injections of autologous platelet rich plasma (PRP) for the treatment of female sexual dysfunction. J Women´s Health Care. 2014; 3: 169-214.
- Bachelet JT, Mojallal A, Boucher F. Chirurgie génitale féminine, les techniques d’amplification du point-G--État de la science [Female genital surgery, G-spot amplification techniques--state of the science]. Ann Chir Plast Esthet. 2014; 59: 344-347.
- Ostrzenski A. G-Spotplasty: A New Surgical Plastic Intervention-The Preliminary Study. Aesthetic Plast Surg. 2018; 42: 1126-1132.
- Gravina GL, Brandetti F, Martini P, Carosa E, Di Stasi SM, Morano S, et al. Measurement of the thickness of the urethrovaginal space in women with or without vaginal orgasm. J Sex Med. 2008; 5: 610-618.
- Ostrzenski A, Krajewski P, Ganjei-Azar P, Wasiutynski AJ, Scheinberg MN, Tarka S, et al. Verification of the anatomy and newly discovered histology of the G-spot complex. BJOG. 2014; 121: 1333-1339.
- Puppo V, Puppo G. Anatomy of sex: Revision of the new anatomical terms used for the clitoris and the female orgasm by sexologists. Clin Anat. 2015; 28: 293-304.
- Puppo V, Gruenwald I. Does the G-spot exist? A review of the current literature. Int Urogynecol J. 2012; 23: 1665-1669.
- Hoag N, Keast JR, O’Connell HE. The “G-Spot” Is Not a Structure Evident on Macroscopic Anatomic Dissection of the Vaginal Wall. J Sex Med. 2017; 14: 1524-1532.
- Sivasl?o?lu AA, Köseo?lu S, Dinç Elibol F, Dere Y, Keçe AC, Çal??kanE. Searching for radiologic and histologic evidence on live vaginal tissue: Does the G-spot exist? Turk J Obstet Gynecol. 2021; 18: 1-6.
- Jannini EA, Buisson O, Rubio-Casillas A. Beyond the G-spot: clitourethrovaginal complex anatomy in female orgasm. Nat Rev Urol. 2014; 11: 531-538.
- Vieira-Baptista P, Lima-Silva J, Preti M, Xavier J, Vendeira P, Stockdale CK. G-spot: Fact or Fiction?: A Systematic Review. Sex Med. 2021; 9: 100435.
- Foldes P, Buisson O. The clitoral complex: a dynamic sonographic study. J Sex Med. 2009; 6:1223-1231.
- Ellibe? Kaya A, Çal??kan E. Women self-reported G-spot existence and relation with sexual function and genital perception. Turk J Obstet Gynecol. 2018; 15: 182-187.
- Willison N, Behnia-Willison F, Aryan P, Padhani ZA, Mirzaei Damabi N, Nguyen T, et al. Application of Platelet-Rich Plasma in Gynaecologic Disorders: A Scoping Review. J Clin Med. 2025; 14: 5832.
- Herold C, Motamedi M, Hartmann U, Allert S. G-spot augmentation with autologous fat transplantation. J Turk Ger Gynecol Assoc. 2015; 16: 187-188.
- Aguilar P, Hersant B, SidAhmed-Mezi M, Bosc R, Vidal L, Meningaud JP. Novel technique of vulvo-vaginal rejuvenation by lipofilling and injection of combined platelet-rich-plasma and hyaluronic acid: a case-report. Springerplus. 2016; 5: 1184.
- Ragy S, Kahky HE, Elfakkar NMZ, Nassar SAM, El-Husseiny RM. Injection of hyaluronic acid versus platelet rich plasma for treatment of vulvovaginal atrophy in post-menopausal females. Arch Dermatol Res. 2025; 317: 305.
- Dankova I, Pyrgidis N, Tishukov M, Georgiadou E, Nigdelis MP,Solomayer EF, et al. Efficacy and Safety of Platelet-Rich Plasma Injections for the Treatment of Female Sexual Dysfunction and Stress Urinary Incontinence: A Systematic Review. Biomedicines. 2023; 11: 2919.
- Sukgen G, Ellibe? Kaya A, Karagün E, Çal??kan E. Platelet-rich plasma administration to the lower anterior vaginal wall to improve female sexuality satisfaction. Turk J Obstet Gynecol. 2019; 16: 228-234.
- Yang F, Liu Y, Xiao H, Ma J, Cun H, Wu C. A Novel Technique Combining Human Acellular Dermal Matrix (HADM) and Enriched Platelet Therapy (EPT) for the Treatment of Vaginal Laxity: A Single-Arm, Observational Study. Aesthetic Plast Surg. 2022; 46: 1884-1892.










































































































































{kind=link}