Cumulative Live Birth Rate and Prognostic Stability of POSEIDON Classification in IVF/ICSI Patients
- 1. Centre for Reproductive Medicine, Antwerp University Hospital, Belgium
- 2. Department of Gynecology, Antwerp University Hospital, Belgium
Abstract
Background: The POSEIDON criteria classify IVF/ICSI patients with hyporesponse, but their clinical value and stability remain uncertain. Objectives: This study evaluates the POSEIDON criteria using Anti-Müllerian Hormone (AMH) as an ovarian reserve biomarker. It compares the Cumulative Live Birth Rate (CLBR) per IVF/ICSI cycle in POSEIDON-defined hyporesponders versus normal responders, assesses whether redefining suboptimal response as 4–7 oocytes improves classification, and examines how many patients in POSEIDON groups transition to normal responders after adjusted stimulation protocols. Methods: A retrospective cohort study of 800 women aged 19-43 undergoing their first IVF/ICSI cycle at Antwerp University Hospital (2018-2022). Participants were post-hoc categorized into POSEIDON groups (n= 532, 66.5%) or a control group (n=268, 33.5%) based on AMH, age, and retrieved oocytes. Results: CLBR in POSEIDON groups was significantly lower than in normal responders (24.1% vs. 56.8%; p<0.001). Younger groups 1 (36.5%) and 3 (24.4%) had higher CLBR than groups 2 (22.4%) and 4 (11.3%). Adjusted criteria yielded similar patterns. After modified stimulation, 39% of POSEIDON patients transitioned to normal responders, while 38% of initial normal responders shifted to POSEIDON. Gonadotropin dose and protocol type influenced reclassification. Conclusions: Patients in POSEIDON groups have a significantly lower prognosis following IVF/ICSI compared to normal responders, with CLBR variation driven by age and oocyte number. The results confirm the importance of oocyte quality over quantity. The instability of POSEIDON classifications calls for reconsideration of their clinical utility, based on the observation that patients transition in and out of the POSEIDON classification.
Keywords
• Anti-Müllerian hormone; Assisted reproductive techniques; Cumulative live birth rate; Infertility; In vitro fertilization; POSEIDON classification
Citatiom
Missault B, Janssens L, De Neubourg D (2026) Cumulative Live Birth Rate and Prognostic Stability of POSEIDON Classification in IVF/ICSI Patients. JSM Sexual Med 10(2): 1179.
ABBREVIATIONS
AFC: Antral Follicle Count; AMH: Anti-Müllerian Hormone; BELRAP: Belgian Register for Assisted Procreation; BMI: Body Mass Index; CLBR: Cumulative Live Birth Rate; COS: Controlled Ovarian Stimulation; CRG: Centre for Reproductive Medicine/Centrum voor Reproductieve Geneeskunde; GnRH: Gonadotropin-Releasing Hormone; ICMART: International Committee for Monitoring Assisted Reproductive Technologies; ICSI: Intracytoplasmic Sperm Injection; IUI: Intrauterine Insemination; IVF: In Vitro Fertilization; FSH: Follicle-Stimulating Hormone; hMG: Human Menopausal Gonadotropin; LH: Luteinizing Hormone; PCOS: Polycystic Ovary Syndrome; PGT: Preimplantation genetic testing; POR: Poor Ovarian Reserve; POSEIDON: Patient-Oriented Strategies Encompassing IndividualizeD Oocyte Number; UZA: Antwerp University Hospital/Universitair Ziekenhuis Antwerpen
INTRODUCTION
In In Vitro Fertilization/Intracytoplasmic Sperm Injection (IVF/ICSI) treatment, the primary objective is the birth of a healthy child. Globally, there is a rising trend in the number of women of advanced age seeking fertility treatments. It is well-established that pregnancy rates in this demographic group are notably lower compared to their younger counterparts [1,2]. Besides age, the success of IVF/ICSI is influenced by various factors, including ovarian reserve and the efficacy of controlled ovarian stimulation (COS) [3]. Secondary objectives of IVF/ICSI encompass achieving the shortest time to live birth while minimizing the risk of complications. To accomplish these objectives, the development of a patient-centered treatment strategy is imperative [4-6].
In the past, the prediction of ovarian stimulation outcomes relied on patient characteristics, treatment history, and ovarian reserve biomarkers. These biomarkers, including antral follicle count (AFC) and anti Müllerian hormone (AMH), were utilized to anticipate ovarian response to exogenous gonadotropin stimulation. However, their efficacy in predicting reproductive success in IVF/ICSI is suboptimal [7-9]. The definition of poor ovarian reserve (POR) varies widely and presents a challenge for reproductive specialists. The pathophysiology of POR is characterized by a diminished number of follicles responsive to follicle-stimulating hormone (FSH) stimulation. This condition may arise from reduced ovarian reserve in women of advanced age or from factors such as inadequate gonadotropin dosage or genetic polymorphisms affecting endogenous gonadotropins or their receptors in women with an adequate ovarian reserve [10-12]. In such cases, the response to COS with exogenous gonadotropins is compromised, leading to an insufficient number of recruited follicles [13-15]. Poor and suboptimal responses to COS are defined by the retrieval of fewer than 4 oocytes and 4-9 oocytes, respectively. Given that the number of retrieved oocytes independently predicts likelihood of pregnancy and live birth, it represents a critical cornerstone of IVF/ICSI and plays an important role in treatment success [5,6,16-19].
In 2011, the Bologna criteria for POR were introduced, aiming to standardize the definition of poor responders [20]. While initially intended to enhance the selection of a more uniform study population for clinical trials, subsequent research revealed that the Bologna criteria identified a diverse population with varying baseline characteristics and underlying etiologies, resulting in variable prognoses and reproductive outcomes [21]. Primarily due to their failure to account for the impact of age on oocyte quality, these criteria lacked sufficient guidance for managing POR in a clinical context [22-26].
In 2016, the POSEIDON group introduced a novel and more refined classification system for categorizing patients with “low prognosis,” distinguishing between those with expected and unexpected inadequate ovarian responses to exogenous gonadotropins. These patients were stratified based on the Patient-Oriented Strategies Encompassing IndividualizeD Oocyte Number (POSEIDON) criteria [22,25]. Utilizing factors such as female age, ovarian reserve markers (AFC and/or AMH), and the number of oocytes retrieved in a standard ovarian stimulation cycle, patients were assigned to one of four groups [27]. Initially, patients were categorized into “unexpected poor responders” and “expected poor responders.” The former comprised patients with adequate ovarian reserve yet exhibited a poor or suboptimal response to standard stimulation, retrieving respectively 4 and 4-9 oocytes during a previous ovarian stimulation cycle. The latter group included patients with compromised ovarian reserve. These groups were further divided into young and older patient subgroups, using the age threshold of 35 years. Through these criteria, distinctions related to suboptimal or poor treatment outcomes were delineated, leading to the creation of more homogeneous patient groups and influencing the clinical management of subfertility [28].
Compared to normal responders with an adequate ovarian reserve, patients in POSEIDON groups are presumed to face an elevated risk of failing to complete a pregnancy after IVF/ICSI. It is suggested that the cumulative live birth rate (CLBR) per stimulated aspiration cycle (including all subsequent fresh and/or frozen embryo transfers, until one delivery with a live birth occurred or until all embryos were used, whichever occurred first) is a critical outcome that distinguishes the different POSEIDON groups [29].
In a comprehensive multicenter retrospective cohort study, Esteves et al. demonstrated that the CLBR was diminished in POSEIDON groups compared to non POSEIDON groups, with notable variations observed across distinct POSEIDON groups [30]. Patient classification in this study was based on AFC as the biomarker for ovarian reserve, highlighting the need for further investigation using alternative ovarian reserve markers such as AMH [30-39].
Building on these findings, the present study evaluates and refines the POSEIDON criteria using data from the Belgian Register for Assisted Procreation (BELRAP), offering population-specific insights into ovarian stimulation outcomes. Analysis of the 2020 BELRAP data revealed a mean number of oocytes of 8.7 per aspiration cycle [40-54], suggesting that a substantial proportion of patients currently classified as POSEIDON hyporesponders may not align with the intended definition of low-prognosis patients. This observation serves as the basis for revising the criteria to better reflect clinical realities.
Objectives
The study addresses three interconnected research objectives, validating the POSEIDON criteria using AMH as the biomarker for ovarian reserve. First, it aims to assess the CLBR per aspiration IVF/ICSI cycle in hyporesponder patients defined by the current POSEIDON criteria, comparing outcomes to those of normal responders. Secondly, the study investigates whether redefining suboptimal responses (subgroups 1b and 2b) as the retrieval of four to seven oocytes based on insights from the 2020 BELRAP data, rather than four to nine, provides a better selection of patients with hyporesponse. This revision reclassifies patients retrieving eight or more oocytes as normal responders, allowing a reassessment of CLBR under the updated criteria. Finally, the study examines consecutive stimulated cycles of POSEIDON patients to determine how many can transition to normal responders following adjustments to COS protocols. These findings aim to refine the clinical utility of the POSEIDON criteria, ensuring they align with real-world patient outcomes and improve IVF/ICSI strategies.
MATERIALS AND METHODS
Study design and population
This retrospective cohort study examined patients aged 19 to 43 years undergoing their first IVF/ICSI cycle at the Centre for Reproductive Medicine, Antwerp University Hospital, Belgium, between April 2018 and December 2022. Patients who underwent preimplantation genetic testing (PGT) and those treated with minimal stimulation protocols (daily FSH dose <100 IU) were excluded. AMH was used as the biomarker for ovarian reserve and was determined at the time of intake, with a maximum interval of one year between AMH assessment and the first ovarian stimulation. For each included patient, all available cycles within the study’s specified time frame were analyzed.
Cycles were cancelled for medical or non-medical reasons. However, cycles were included if they were cancelled because of elevated FSH at baseline, hyporesponse after stimulation leading to cancellation of IVF/ICSI or switch to intrauterine insemination (IUI), or a drop in estradiol levels and/or stagnation of follicle growth after the initiation of the antagonist.
Treatment characteristics
The protocols used for ovarian stimulation include either a Gonadotropin-Releasing Hormone (GnRH) antagonist protocol or a short or long GnRH agonist protocol. Ovarian stimulation was done with recombinant FSH (rec FSH) (Gonal-F® [Merck], Bemfola® [Gedeon Richter], Puregon® [MSD], Rekovelle® [Ferring] or Elonva® [Organon]), rec-FSH in combination with recombinant luteinizing hormone (rec-LH) (Pergoveris® Merck]), or highly purified human menopausal gonadotrophin (hMG) (Menopur® [Ferring]). The ovarian stimulation protocol was primarily based on female age, ovarian reserve, and, if available, previous ovarian stimulation history. Ovarian response was monitored using transvaginal ultrasonography and measurements of serum oestradiol, progesterone and LH. Final oocyte maturation was induced by subcutaneous administration of either Human Chorionic Gonadotropin (hCG) or a GnRH agonist. Oocytes were retrieved using transvaginal ultrasound-guided pickup and inseminated via IVF or ICSI. Subsequently, embryos were cultured to the cleavage or blastocyst stage and were then either transferred fresh or vitrified. Pregnancy was monitored until delivery.
Data input
Demographic and patient data included female age, Body Mass Index (BMI), obstetric and general medical history, duration of infertility, infertility factors and AMH values. If a male partner was present, data collected included male age, BMI, and male infertility factors.
Treatment data comprised the type of IVF/ICSI treatment, type of GnRH analogue used, type of gonadotropin used, total and mean daily dose of gonadotropin administered, duration of stimulation, and type of trigger used. Laboratory data included the number of oocytes retrieved, embryos obtained, embryos transferred, cryopreserved embryos, and amount of fresh or frozen-thawed embryo transfer cycles. Additionally, pregnancy rate and live birth rate were collected.
Patient classification
Patients were classified into four groups based on the POSEIDON criteria [27]. Those who did not meet any of the four POSEIDON group criteria were placed in a fifth, non POSEIDON group. This non-POSEIDON group comprises patients with a normal ovarian reserve and an adequate response to COS, serving as a control group of normal responders. As previously mentioned, AMH was used as the biomarker for ovarian reserve and was utilized to classify patients into the different POSEIDON groups.
For the second research question, subgroups 1b and 2b are redefined, creating new subgroups 1b bis and 2b bis, which include patients who retrieved 4–7 oocytes. Patients who retrieved eight or more oocytes are classified as normal responders and moved to the non-POSEIDON control group.
Main outcome measures
The primary outcome is the Cumulative Live Birth (CLB), defined as at least one live birth per aspirated IVF/ ICSI cycle, according to the ICMART definition [40]. Cycles were included for analysis of CLB when a live birth had been achieved following a fresh or frozen-thawed embryo transfer or did not achieve a live birth after transferring all embryos obtained in each cycle.
Statistical analysis
Baseline and treatment characteristics are presented across different groups, using median and interquartile ranges for continuous variables, and absolute and relative frequencies for categorical variables. Female age, BMI and AMH between groups were compared using either Kruskal Wallis test and Dunn’s test for pairwise comparisons, or Mann-Whitney-Wilcoxon test. Frequencies of live births were compared between groups using Pearson’s Chi squared test. All p-values from pairwise comparisons were adjusted using the Bonferroni correction. The total and daily doses of FSH between the first and second cycle were compared using paired t-tests. P-values below 0.05 were considered statistically significant. All analyses were performed using Stata/SE 18.0.
Ethical approval
This study was approved by the Ethics Committee of the UZA (project ID 6334). The requirement for informed consent was waived due to the retrospective nature of the study.
RESULT
Number of subjects
This study includes a total of 1.437 cycles from 800 patients. Among these, 532 patients (66.5%) were classified into the pre-defined POSEIDON groups, while the remaining 268 patients (33.5%) served as the control group (Figure 1).
Patient and treatment characteristics
Table 1: Baseline characteristics (values are in median and interquartile range or number and percentage). Subscript letters denote statistically significant differences between the respective groups (p < 0.05)
|
|
POSEIDON Group 1 |
POSEIDON Group 2 |
POSEIDON Group 3 |
POSEIDON Group 4 |
Control Group <35j |
Control Group ≥35j |
|||
|
1a n = 42 |
1b n = 150 |
2a n = 18 |
2b n = 67 |
n = 78 |
n = 177 |
n = 203 |
n = 65 |
||
|
Baseline characteristics |
|||||||||
|
Female age |
30.5 |
31.1 |
39.7 |
38.6 |
32.1 |
39.7 |
30.0 |
37.0 |
|
|
(years) |
[27.6- 32.6]a1 |
[29.0-32.9]a2 |
[37.6-40.5]c1 |
[36.9-40.3]c2 |
[30.4-33.7]a,b |
[36.9-41.1]d |
[28.3-32.4]b |
[35.8-39.2]c,d |
|
|
BMI (kg/m2) |
24.9 |
24.8 |
23.6 |
25.7 |
23.8 |
24.5 |
22.9 [ |
22.5 |
|
|
[22.2 -29.2] |
[21.6 -28.7] |
[21.9 -31.5] |
[22.4 -28.7] |
[22.1 -27.7] |
[21.9 -28.6] |
20.5 -26.8] |
[20.8 -25.8] |
||
|
Infertility duration |
2.2 |
2.3 |
2.7 |
3.1 |
2.5 |
3.0 |
2.4 |
3.0 |
|
|
(years) |
[1.7 -3.1] |
[1.8 -3.3] |
[1.9 -3.7] |
[2.2 -5.1] |
[1.9 -3.6] |
[2.2 -5.6] |
[1.7 -3.4] |
[2.2 -4.8] |
|
|
Cause of infertility |
|||||||||
|
vulatory |
13 (37.1) |
32 (23.2) |
2 (13.3) |
11 (20.0) |
38 (58.5) |
82 (54.0) |
65 (35.1) |
11 (20.4) |
|
|
1 (2.9) |
10 (7.3) |
2 (13.3) |
7 (12.7) |
7 (10.9) |
25 (16.8) |
9 (4.9) |
4 (7.4) |
||
|
Uterine factor |
|||||||||
|
9 (25.7) |
36 (26.5) |
8 (53.3) |
13 (23.6) |
18 (28.1) |
47 (31.8) |
48 (26.4) |
12 (22.6) |
||
|
Tubal |
|||||||||
|
Endometriosis |
11 (32.4) |
39 (28.7) |
2 (13.3) |
8 (14.8) |
21 (32.3) |
40 (26.9) |
40 (22.0) |
11 (20.8) |
|
|
Male factor |
|||||||||
|
21 (50.0) |
92 (61.7) |
13 (76.5) |
34 (55.7) |
48 (62.3) |
80 (48.5) |
121 (60.5) |
29 (50.9) |
||
|
Combined |
|||||||||
|
11 (32.4) |
43 (32.1) |
9 (60.0) |
12 (24.0) |
37 (58.7) |
57 (40.4) |
53 (30.1) |
10 (22.7) |
||
|
AMH (ng/mL) |
3.6 [1.8-6.3]e1 |
2.7 [1.9 -4.2]e2 |
1.5 [1.3 -1.6]f1 |
1.9 [1.5 -2.9]f2 |
0.7 [0.5-1.0] |
0.5 [0.3-0.9] |
3.3 [2.3-5.1]e |
2.8 [1.9 -3.9]f |
|
Table 1 presents the baseline characteristics of the study population. In both age categories, the control groups had a slightly lower median age than their corresponding
POSEIDON groups. Within the <35 years group, significant age differences were found. Group 1 had a lower median age than group 3 (p = 0.004), and group 3 had a higher median age than the <35 years control group (p < 0.001). In the ≥35 years category, both group 2 and group 4 had higher median ages compared to the control group (p = 0.01 and p < 0.001, respectively). Other age comparisons between groups were not statistically significant.
Median BMI was significantly higher in the POSEIDON groups compared to the control groups (p < 0.001) but did not vary significantly among the different POSEIDON groups.
Table 2: Treatment characteristics (values are in median and interquartile range or number and percentage)
|
|
Poseidon Group 1 |
POSEIDON Group 2 |
POSEIDON Group 3 |
POSEIDON Group 4 |
Control Group <35j |
Control Group ≥35j |
||
|
1a (n = 42) |
1b (n = 150) |
2a (n = 18) |
2b (n = 67) |
n = 78 |
n = 177 |
n = 203 |
n = 65 |
|
|
Treatment characteristics |
||||||||
|
N° of ovarian stimulation cycles |
2 [1-2] |
1 [1-2] |
2 [2-3] |
1 [1-2] |
2 [1-2] |
2 [1-3] |
1 [1-1] |
1 [1-2] |
|
Number of oocytes retrieved |
3 [2-3] |
7 [6-8] |
3 [2-3] |
6 [5-8] |
5 [4-8] |
4 [2-6] |
14 [12-17] |
12 [11-15] |
|
Number of embryo transfers per aspiration cycle |
1 [0-1] |
1 [1-2] |
0.5 [0-1] |
1 [1-2] |
1 [1-2] |
1 [0-1] |
1 [1-2] |
1 [1-2] |
|
Ovarian stimulation protocol Agonist - long Agonist - short Antagonist |
|
|||||||
|
7 (16.7) |
44 (29.3) |
5 (27.8) |
10 (14.9) |
24 (30.8) |
28 (15.8) |
55 (27.2) |
19 (29.2) |
|
|
4 (9.5) |
11 (7.3) |
1 (5.6) |
12 (17.9) |
15 (19.2) |
58 (32.7) |
11 (5.5) |
6 (9.2) |
|
|
31 (73.8) |
95 (63.3) |
12 (66.7) |
45 (67.2) |
39 (50.0) |
91 (51.4) |
136 (67.3) |
40 (61.5) |
|
|
Method of fertilization IVF ICSI IVF/ICSI combined |
|
|||||||
|
21 (50.0) |
73 (48.7) |
8 (44.4) |
38 (56.7) |
28 (35.9) |
106 (59.9) |
95 (46.8) |
36 (55.4) |
|
|
10 (23.8) |
43 (28.7) |
6 (33.3) |
11 (16.4) |
29 (37.2) |
42 (23.7) |
65 (32.1) |
16 (24.6) |
|
|
11 (26.2) |
34 (22.7) |
4 (22.2) |
18 (26.9) |
21 (26.9) |
29 (16.4) |
43 (21.2) |
13 (20.0) |
|
|
Source of sperm Partner Donor |
|
|
|
|
|
|
|
|
|
42 (100) |
147 (98) |
17 (94.4) |
59 (88.1) |
77 (98.7) |
162 (91.5) |
199 (98.0) |
57 (87.7) |
|
|
0 (0.0) |
3 (2.0) |
1 (5.6) |
8 (11.9) |
1 (1.3) |
15 (8.5) |
4 (2.0) |
8 (12.3) |
|
|
Use of OAC before stimulation No Yes |
|
|||||||
|
16 (38.1) |
45 (30.0) |
6 (33.3) |
29 (43.3) |
26 (33.3) |
90 (50.9) |
78 (38.8) |
28 (43.1) |
|
|
26 (61.9) |
105 (70.0) |
12 (66.7) |
38 (56.7) |
52 (66.7) |
87 (49.2) |
123 (61.2) |
37 (56.9) |
|
|
Stimulation duration (days) |
10 [8.3-11.5] |
9.9 [8.5-11] |
8.3 [6.8-10.5] |
9 [8-11] |
9.5 [8-11] |
9 [8-11] |
9.5 [8.5-11] |
10 [8.7-10.7] |
|
Total gonadotropin dose (IU) |
1606.9 [1350-1990] |
1603.3 [1313-1932] |
1800.0 [1316-2119] |
1912.5 [1575-2138] |
2119.8 [1688-2475] |
2215.0 [1820-2720] |
1500.0 [1250-1688] |
1650.0 [1350-2044] |
|
Daily gonadotropin dose (IU) |
151.9 [131-190] |
168.8 [150-194] |
215.6 [186-245] |
214.3 [188-225] |
225.0 [206-256] |
237.0 [222-265] |
150.0 [147-187] |
187.5 [150-210] |
As per definition, AMH levels were lower in POSEIDON groups 3 and 4 compared to groups 1 and 2, but also decreased with age, being lower in group 2 compared to group 1. Furthermore, the median AMH levels of the control groups were significantly higher compared to those in POSEIDON groups 1 and 2 (group 1 vs control group <35y (p= 0.005); group 2 vs control group ≥35y (p< 0.001)).
Details of the treatment characteristics of the studied patients are provided in Table 2.
Cumulative live birth rate
A total of 128 patients out of 532 (24.1%) in the POSEIDON groups and 152 patients out of 268 (56.7%) in the control group achieved a live birth following their first stimulation cycle and the transfer of one or more embryos derived from this cycle. The CLBR was significantly lower in POSEIDON groups compared to the control group (p < 0.001) and varied across the POSEIDON subgroups.
Among the subgroups, those with the youngest populations had the highest CLBR, with group 1 at 36.5% and group 3 at 24.4%. The CLBR in group 3 was 22.4%, while the lowest rate was observed in group 4 (11.3%). The CLBR was significantly higher in the control group <35 years compared to both group 1 and group 3 (p < 0.001). Similarly, the control group ≥35 years had a significantly higher CLBR compared to group 4 (p < 0.001). No other comparisons reached statistical significance (Figure 2).
Adjusted POSEIDON groups
With the application of the adjusted POSEIDON criteria, there was a shift from the original POSEIDON groups to the control group, classifying 465 patients (58.1%) into the pre-defined POSEIDON groups, while the remaining 335 patients (41.9%) served as the control group.
Adjusted POSEIDON groups: cumulative live birth rate
The CLBR was 21.5% (100/465) in the adjusted POSEIDON groups and statistically significantly lower than 53.7% (180/335) in the control groups (p <0.001). The CLBR was 21.4% (9/42) for group 1a, 35.3% (36/102) for group 1b, 0.00% (0/18) for 2a, 33.3% (16/48) for 2b, with a total of 31.3% (45/144) for group 1 and 24.2% (16/66) for group 2. The CLBR’s of group 3 and 4 remained 24.4% (19/78) and 11.3% (20/177), respectively.
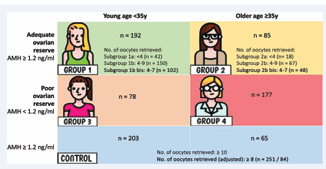
Figure 1 POSEIDON classification and adjusted POSEIDON classification. Adjustments from the POSEIDON classification are in bold
Compared to the original POSEIDON classification, the CLBR for group 1b was lower (40.7% vs. 35.3%), while it was higher for group 2b (28.4% vs. 33.3%). The CLBR for the control groups also declined (65.0% vs. 62.5% for the younger control group and 30.8% vs. 27.4% for the older control group). The observed differences did not reach statistical significance.

Figure 2 CLBR after the first aspiration cycle in POSEIDON groups
Among patients under 35 years old, CLBRs differed significantly between groups (p < 0.001), with both group 1 and group 3 showing significantly lower rates than the control (p < 0.001), but no difference between group 1 and 3 (p = 0.84).
In patients aged 35 years and above, overall differences were also significant (p = 0.002). Group 2 did not differ
from the control (p = 1.00), whereas group 4 showed significantly lower CLBRs compared to both group 2 (p = 0.04) and the control (p = 0.003).
Transition of POSEIDON groups in consecutive cycles
Out of 800 patients, 371 underwent at least two cycles, of which 114 (30.8%) patients were switching groups in the second cycle. POSEIDON groups 3 and 4 are predefined by a low AMH value and cannot change groups.
POSEIDON Group 1 and control group <35y
In group 1, 98 patients underwent a second stimulation cycle and 43 of these patients (43.9%) transitioned from group 1 to the control group (<35 years). In the younger control group, 38 patients underwent at least two cycles of which 16 patients (42.1%) transitioned into the POSEIDON groups.
Among the patients who changed groups, 46.4% experienced a change in their stimulation protocol and 50% had alterations in the type of gonadotropin used. Furthermore, 71.4% received a higher total gonadotropin dose, and 83.9% received a higher daily gonadotropin dose.
POSEIDON Group 2 and control group ³ 35y
In group 2, 48 patients underwent a second stimulation cycle and 14 of these patients (29.2%) transitioned from a POSEIDON group 2 to the control group ³ 35 years. In the older control group, 30 patients underwent at least two cycles of which 10 (33.3%) shifted into the POSEIDON groups.
Among the patients who changed groups, 58.3% had an altered stimulation protocol and 41.7% patients had their type of gonadotropin adjusted. Additionally, 60.9% received a higher total gonadotropin dose, and 65.2% were administered a higher daily gonadotropin dose.
Patients changing groups between POSEIDON group 1 and the young control group and between POSEIDON group 2 and the older control group are displayed in Figure 3.
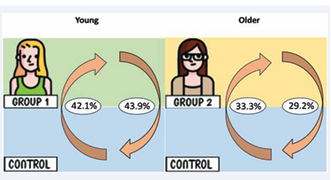
Figure 3 Patients changing groups between POSEIDON group 1 and the young control group and between POSEIDON group 2 and the older control group
Overall, 39% of patients in POSEIDON groups 1 and 2 transitioned to normal responders after adjusted stimulation protocols, while 38% of initial normal responders shifted into POSEIDON groups.
DISCUSSION
This retrospective observational cohort study assessed the CLBR per aspiration IVF/ICSI cycle in hyporesponder patients, as defined by the POSEIDON criteria, using AMH as the biomarker for ovarian reserve. After investigating a total of 1.437 cycles from 800 patients, 532 patients (66.5%) were classified into the POSEIDON groups, while the remaining 268 patients (33.5%) served as the control group.
Analysis revealed that the CLBR in POSEIDON patients was 24.1% compared to 56.7% in patients with an adequate ovarian reserve and effective response to COS. These findings substantiate the concept that patients meeting the POSEIDON criteria have a significantly lower prognosis following IVF/ICSI compared to normal responders.
As discussed in literature, differences in CLBR across POSEIDON groups are primarily attributable to female age and the number of oocytes retrieved, highlighting the importance of both oocyte quality and quantity on fertility and outcomes after IVF/ICSI treatment [41-43]. The impact of female age on reproductive potential is explained by both the age-related decline in oocyte quality and the coinciding progressive decrease in primordial follicles [44,45]. After the age of 35, the number of euploid embryos decreases rapidly, which most likely explains the significantly lower CLBR in the older POSEIDON groups [46,47]. Secondarily, the differences in CLBR were attributable to the number of oocytes retrieved. Studies show that, within specific age
categories, reduced ovarian response and lower AMH are both associated with a decreased probability of live birth [18,48,49]. The fact that the CLBR of older patients with a normal ovarian reserve (group 2) did not exceed that of younger patients with a low ovarian reserve (group 3) suggests that female age has a greater impact on the CLBR than quantitative parameters. This likely reflects the higher importance of oocyte quality over quantity in obtaining high-quality embryos with good implantation capacity, creating the well-known protective age-related effect on oocyte and embryo quality in younger POSEIDON groups [45,50-52].
Prior studies have reported on CLBR in POSEIDON groups, each with a slightly different scope on the definition of CLBR [30-39]. The majority of this study’s results align with the CLBRs reported in the literature. The most notable differences are observed in POSEIDON groups 1 and 3, likely partially due to the small sample sizes in this study. However, it is important to note that in this study, AMH was used as the biomarker for ovarian reserve to classify patients into their respective POSEIDON groups. In the reviewed literature, only the studies by Leijdekkers et al. [34], and Yan et al. [38], also utilized AMH as their biomarker for ovarian reserve. Although Leijdekkers et al. [34], used data from the OPTIMIST study to focus on CLBR after 18 months of observation, the CLBRs after the first stimulation cycle for all POSEIDON subgroups were available and, upon comparison, were found to be very similar to the CLBRs of this study. Notably, they excluded all patients with Polycystic Ovary Syndrome (PCOS) from their study population and included a separate control group, the rationale for which remains undisclosed. Conversely, Yan et al. [38], reported only on POSEIDON groups 1 and 3 and noted a remarkably higher CLBR than those observed in this research.
Considering our population, which comprises multiple ethnicities with a predominance of Caucasians, the generalizability of results from studies conducted in other populations, such as an Asian population, is questionable. For instance, Gu et al. [33], reported a normal BMI in 80% of their population, a significant divergence from our study where 42.8% of patients were overweight or obese. Given the well-established influence of BMI on fertility, this factor warrants careful consideration [53].
Esteves et al. [30], conducted a substantial multicenter study involving 4.433 patients, using AFC as the ovarian biomarker for classifying patients into their respective POSEIDON groups. Remarkably, they were the sole study in the reviewed literature to also stratify their control group into two age categories: under and over 35 years of age. Their findings revealed a CLBR after one aspiration cycle nearly 50% lower, on average, in the POSEIDON group compared to that of normal responders, aligning with our results.
All studies reporting on the subgroups of POSEIDON groups 1 and indicated a higher CLBR in subgroup 1b compared to subgroup 1a, highlighting the substantial influence of the number of retrieved oocytes.
In conclusion, the findings of this study, along with the reviewed literature, highlight the importance of female age and the number of oocytes retrieved, emphasizing the critical roles of both oocyte quality and quantity in determining reproductive outcomes.
The application of the adjusted POSEIDON criteria resulted in a reclassification, with 58.1% of patients being categorized into the adjusted POSEIDON groups, while the remaining 41.9% were classified into the control group. The CLBR observations in the adjusted POSEIDON groups remained consistent with previous findings from the original POSEIDON classification. Hence a revision of the current criteria of POSEIDON classification is not warranted.
After examining the first two cycles of patients to examine the potential to leave the POSEIDON classification and become normal responders after the second stimulation cycle, the analysis revealed that 39% of the patients in groups 1 and 2 left the POSEIDON classification to join the control group. Conversely, up to 38% of the patients in the control groups shifted into the POSEIDON groups after the second stimulation cycle. Patients switched groups following changes in their stimulation protocol, type of gonadotropin, and/or increases in their daily and total gonadotropin doses.
Clinical implications
In response to criticisms of the Bologna criteria, the POSEIDON criteria were introduced to create more homogeneous patient groups and improve the clinical management of hyporesponder patients. The consistent CLBR of POSEIDON groups across various studies indicates that these groups are well-defined and reproducible worldwide. The POSEIDON criteria aim to categorize patients into comparable groups based on age and AMH levels, facilitating more accurate comparisons. However, it is notable in this study that both age and AMH are significantly different between the POSEIDON groups and the control groups, with control groups exhibiting lower age and higher AMH levels. Additionally, the significantly lower BMI observed in the control groups compared to the
POSEIDON groups suggests that the POSEIDON criteria do not account for BMI, a crucial factor influencing fertility potential.
Notably, in this study, where POSEIDON and control groups were derived from the same population without exclusions, 66.5% of the study population were assigned to a POSEIDON group and were thus classified as hyporesponders. When applying the adjusted POSEIDON criteria, which are considered more suitable for the Belgian population following the BELRAP data, the percentage of hyporesponder patients decreases to 58.1%. Regardless of the criteria used, more than half of the population is classified as hyporesponders with a “low prognosis.”
Additionally, it is noteworthy how easily patients in POSEIDON groups can switch between groups when reassessed after the second cycle, raising further questions about the stability of these classifications. Given that up to 39% of patients in POSEIDON groups 1 and 2 can transition out of their respective groups, it raises the question of whether these women should be categorized as hyporesponders in clinical practice.
Limitations
The primary limitation of this study is the sample size, particularly within certain subgroups. This constraint reduces the precision of the estimates and diminishes the statistical power to detect significant differences. Consequently, it may hinder the ability to draw definitive conclusions. Nonetheless, the findings provide a valuable contribution to the existing literature and offer a reasonable estimation of the POSEIDON groups within our population.
Another limitation of this study is the post-hoc classification of patients into POSEIDON groups, resulting in treatment regimens that were not always tailored according to these groupings. However, in our clinic, treatment regimens are individually adjusted based on comprehensive patient and treatment data to optimize outcomes for each patient.
Lastly, due to the significant differences in age and AMH levels between the POSEIDON groups and the control groups within the same age and AMH strata, the groups being compared do not possess entirely equivalent characteristics at baseline.
ACKNOWLEDGMENTS
The authors are grateful to Jason Bouziotis of the Clinical Trial Center of the Antwerp University Hospital for his assistance with the statistical aspects of this research.
During the preparation of this work the authors used ChatGPT (OpenAI) in order to improve language and readability. After using this tool/service, the authors reviewed and edited the content as needed and take full responsibility for the content of the publication.
REFERENCES
- Malchau SS, Henningsen AA, Loft A, Rasmussen S, Forman J, Nyboe Andersen A, et al. The long-term prognosis for live birth in couples initiating fertility treatments. Hum Reprod. 2017; 32: 1439-1449.
- Smith ADAC, Tilling K, Nelson SM, Lawlor DA. Live-Birth Rate Associated With Repeat In Vitro Fertilization Treatment Cycles. JAMA. 2015; 314: 2654-2662.
- Haahr T, Roque M, Esteves SC, Humaidan P. GnRH Agonist Trigger and LH Activity Luteal Phase Support versus hCG Trigger and Conventional Luteal Phase Support in Fresh Embryo Transfer IVF/ ICSI Cycles-A Systematic PRISMA Review and Meta-analysis. Front Endocrinol (Lausanne). 2017; 8: 116.
- Dancet EA, Van Empel IW, Rober P, Nelen WL, Kremer JA, D’Hooghe TM. Patient-centred infertility care: a qualitative study to listen to the patient’s voice. Hum Reprod. 2011; 26: 827-833.
- Haahr T, Esteves SC, Humaidan P. Poor definition of poor-ovarian response results in misleading clinical recommendations. Hum Reprod. 2018; 33: 979-980.
- Haahr T, Esteves SC, Humaidan P. Individualized controlled ovarian stimulation in expected poor-responders: an update. Reprod Biol Endocrinol. 2018; 16: 20.
- Broer SL, Dólleman M, Opmeer BC, Fauser BC, Mol BW, Broekmans FJ. AMH and AFC as predictors of excessive response in controlled ovarian hyperstimulation: a meta-analysis. Hum Reprod Update. 2011; 17: 46-54.
- Broer SL, Mol B, Dólleman M, Fauser BC, Broekmans FJ. The role of anti-Müllerian hormone assessment in assisted reproductive technology outcome. Curr Opin Obstet Gynecol. 2010; 22: 193-201.
- Grisendi V, Mastellari E, La Marca A. Ovarian Reserve Markers to Identify Poor Responders in the Context of Poseidon Classification. Front Endocrinol (Lausanne). 2019; 10: 281.
- Alviggi C, Clarizia R, Pettersson K, Mollo A, Humaidan P, Strina I, et al. Suboptimal response to GnRHa long protocol is associated with a common LH polymorphism. Reprod Biomed Online. 2011; 22: S67-S72.
- Alviggi C, Conforti A, Caprio F, Gizzo S, Noventa M, Strina I, et al. In Estimated Good Prognosis Patients Could Unexpected “Hyporesponse” to Controlled Ovarian Stimulation be related to Genetic Polymorphisms of FSH Receptor? Reprod Sci. 2016; 23: 1103-1108.
- La Marca A, Papaleo E, Alviggi C, Ruvolo G, De Placido G, Candiani M, et al. The combination of genetic variants of the FSHB and FSHR genes affects serum FSH in women of reproductive age. Hum Reprod. 2013; 28: 1369-1374.
- Alviggi C, Mollo A, Clarizia R, De Placido G. Exploiting LH in ovarian stimulation. Reprod Biomed Online. 2006; 12: 221-233.
- Alviggi C, Pettersson K, Longobardi S, Andersen CY, Conforti A, De Rosa P, et al. A common polymorphic allele of the LH beta-subunit gene is associated with higher exogenous FSH consumption during controlled ovarian stimulation for assisted reproductive technology. Reprod biol endocrinol. 2013; 11: 51.
- La Marca A, Sighinolfi G, Argento C, Grisendi V, Casarini L, Volpe A, et al. Polymorphisms in gonadotropin and gonadotropin receptor genes as markers of ovarian reserve and response in in vitro fertilization. Fertil Steril. 2013; 99: 970.e1-978.e1.
- Drakopoulos P, Blockeel C, Stoop D, Camus M, de Vos M, Tournaye H, et al. Conventional ovarian stimulation and single embryo transfer for IVF/ICSI. How many oocytes do we need to maximize cumulative live birth rates after utilization of all fresh and frozen embryos? Hum Reprod. 2016; 31: 370-376.
- Polyzos NP, Sunkara SK. Sub-optimal responders following controlled ovarian stimulation: an overlooked group? Hum Reprod. 2015; 30: 2005-2008.
- Sunkara SK, Rittenberg V, Raine-Fenning N, Bhattacharya S, Zamora J, Coomarasamy A. Association between the number of eggs and live birth in IVF treatment: an analysis of 400 135 treatment cycles. Hum Reprod. 2011; 26: 1768-1774.
- Verberg MF, Eijkemans MJ, Macklon NS, Heijnen EM, Baart EB, Hohmann FP, et al. The clinical significance of the retrieval of a low number of oocytes following mild ovarian stimulation for IVF: a meta-analysis. Hum Reprod Update. 2009; 15: 5-12.
- Ferraretti AP, La Marca A, Fauser BC, Tarlatzis B, Nargund G, Gianaroli L. ESHRE consensus on the definition of ‘poor response’ to ovarian stimulation for in vitro fertilization: the Bologna criteria. Hum Reprod. 2011; 26: 1616-1624.
- Papathanasiou A. Implementing the ESHRE ‘poor responder’ criteria in research studies: methodological implications. Hum Reprod. 2014; 29: 1835-1838.
- Alviggi C, Andersen CY, Buehler K, Conforti A, De Placido G, Esteves SC, et al. A new more detailed stratification of low responders to ovarian stimulation: from a poor ovarian response to a low prognosis concept. Fertil Steril. 2016; 105: 1452-1453.
- Boots CE, Bernardi LA. Bologna criteria: clinically or academically relevant? Fertil Steril. 2018; 109: 59-60.
- Boza A, Oguz SY, Misirlioglu S, Yakin K, Urman B. Utilization of the Bologna criteria: a promise unfulfilled? A review of published and unpublished/ongoing trials. Fertil Steril. 2018; 109: 104.e2-109.e2.
- Humaidan P, Alviggi C, Fischer R, Esteves SC. The novel POSEIDON stratification of ‘Low prognosis patients in Assisted Reproductive Technology’ and its proposed marker of successful outcome. F1000Res. 2016; 5: 2911.
- Younis JS, Ben-Ami M, Ben-Shlomo I. The Bologna criteria for poor ovarian response: a contemporary critical appraisal. J Ovarian Res. 2015; 8: 76.
- Esteves SC, Roque M, Bedoschi GM, Conforti A, Humaidan P, Alviggi C. Defining Low Prognosis Patients Undergoing Assisted Reproductive Technology: POSEIDON Criteria-The Why. Front Endocrinol (Lausanne). 2018; 9: 461.
- Esteves SC, Alviggi C, Humaidan P, Fischer R, Andersen CY, Conforti A, et al. The POSEIDON Criteria and Its Measure of Success through the Eyes of Clinicians and Embryologists. Front Endocrinol (Lausanne). 2019; 10: 814.
- Esteves SC, Conforti A, Sunkara SK, Carbone L, Picarelli S, Vaiarelli A, et al. Improving Reporting of Clinical Studies Using the POSEIDON Criteria: POSORT Guidelines. Front Endocrinol (Lausanne). 2021; 12: 587051.
- Esteves SC, Yarali H, Vuong LN, Carvalho JF, Özbek ? Y, Polat M, et al. Cumulative delivery rate per aspiration IVF/ICSI cycle in POSEIDON patients: a real-world evidence study of 9073 patients. Hum Reprod. 2021; 36: 2157-2169.
- Abdullah RK, Liu N, Zhao Y, Shuang Y, Shen Z, Zeng H, et al. Cumulative live-birth, perinatal and obstetric outcomes for POSEIDON groups after IVF/ICSI cycles: a single-center retrospective study. Sci Rep. 2020; 10: 11822.
- Bansiwal R, Mahey R, Malhotra N, Singh N, Saini M, Bhatt A, et al. Comparison of Cumulative Live Birth Rate (CLBR) According to Patient Oriented Strategies Encompassing Individualized Oocyte Number (POSEIDON) Stratification Among Low Prognosis Women Undergoing IVF-ICSI Cycles. J Reprod Infertil. 2023; 24: 117-131.
- Gu F, Ruan S, Luo C, Huang Y, Luo L, Xu Y, et al. Can repeat IVF/ICSI cycles compensate for the natural decline in fertility with age? an estimate of cumulative live birth rates over multiple IVF/ICSI cycles in Chinese advanced-aged population. Aging (Albany NY). 2021; 13: 14385-14398.
- Leijdekkers JA, Eijkemans MJC, van Tilborg TC, Oudshoorn SC, van Golde RJT, Hoek A, et al; OPTIMIST study group. Cumulative live birth rates in low-prognosis women. Hum Reprod. 2019; 34: 1030-1041.
- Li Y, Li X, Yang X, Cai S, Lu G, Lin G, et al. Cumulative Live Birth Rates in Low Prognosis Patients According to the POSEIDON Criteria: An Analysis of 26,697 Cycles of in vitro Fertilization/Intracytoplasmic Sperm Injection. Front Endocrinol (Lausanne). 2019; 10: 642.
- Shi W, Zhou H, Tian L, Zhao Z, Zhang W, Shi J. Cumulative Live Birth Rates of Good and Low Prognosis Patients According to POSEIDON Criteria: A Single Center Analysis of 18,455 Treatment Cycles. Front Endocrinol (Lausanne). 2019; 10: 409.
- Vargas-Tominaga L, Vargas A, Alarcón F, Medina A, Gómez M, BejarK. Cumulative live birth rates of patients in the Peruvian Andes according to the POSEIDON criteria: a single-center retrospective analysis. JBRA Assist Reprod. 2021; 25: 412-416.
- Yan E, Li W, Jin H, Zhao M, Chen D, Hu X, et al. Cumulative live birth rates and birth outcomes after IVF/ICSI treatment cycles in young POSEIDON patients: A real-world study. Front Endocrinol (Lausanne). 2023; 14: 1107406.
- Yang R, Zhang C, Chen L, Wang Y, Li R, Liu P, et al. Cumulative live birth rate of low prognosis patients with POSEIDON stratification: a single-centre data analysis. Reprod Biomed Online. 2020; 41: 834-844.
- Zegers-Hochschild F, Adamson GD, Dyer S, Racowsky C, de Mouzon J, Sokol R, et al. The International Glossary on Infertility and Fertility Care, 2017. Fertil Steril. 2017; 108: 393-406.
- Broer SL, van Disseldorp J, Broeze KA, Dolleman M, Opmeer BC, Bossuyt P, et al. Added value of ovarian reserve testing on patient characteristics in the prediction of ovarian response and ongoing pregnancy: an individual patient data approach. Hum Reprod Update. 2013; 19: 26-36.
- McLernon DJ, Steyerberg EW, Te Velde ER, Lee AJ, Bhattacharya S. Predicting the chances of a live birth after one or more complete cycles of in vitro fertilisation: population based study of linked cycle data from 113 873 women. Bmj. 2016; 355: i5735.
- van Loendersloot LL, van Wely M, Limpens J, Bossuyt PM, Repping S, van der Veen F. Predictive factors in in vitro fertilization (IVF): a systematic review and meta-analysis. Hum Reprod Update. 2010; 16: 577-589.
- Broekmans FJ, Knauff EA, te Velde ER, Macklon NS, Fauser BC. Female reproductive ageing: current knowledge and future trends. Trends Endocrinol Metab. 2007; 18: 58-65.
- Cimadomo D, Fabozzi G, Vaiarelli A, Ubaldi N, Ubaldi FM, Rienzi L. Impact of Maternal Age on Oocyte and Embryo Competence. Front Endocrinol (Lausanne). 2018; 9: 327.
- Demko ZP, Simon AL, McCoy RC, Petrov DA, Rabinowitz M. Effects of maternal age on euploidy rates in a large cohort of embryos analyzed with 24-chromosome single-nucleotide polymorphism-based preimplantation genetic screening. Fertil Steril. 2016; 105: 1307-1313.
- Franasiak JM, Forman EJ, Hong KH, Werner MD, Upham KM, Treff NR, et al. The nature of aneuploidy with increasing age of the female partner: a review of 15,169 consecutive trophectoderm biopsies evaluated with comprehensive chromosomal screening. Fertil Steril. 2014; 101: 656.e1-663.e1.
- Hamdine O, Eijkemans MJC, Lentjes EGW, Torrance HL, Macklon NS, Fauser B, et al. Antimüllerian hormone: prediction of cumulative live birth in gonadotropin-releasing hormone antagonist treatment for in vitro fertilization. Fertil Steril. 2015; 104: 891.e2-898.e2.
- Polyzos NP, Drakopoulos P, Parra J, Pellicer A, Santos-Ribeiro S, Tournaye H, et al. Cumulative live birth rates according to the number of oocytes retrieved after the first ovarian stimulation for in vitro fertilization/intracytoplasmic sperm injection: a multicenter multinational analysis including ∼15,000 women. Fertil Steril. 2018; 110: 661.e1-670.e1.
- Arce JC, Andersen AN, Fernández-Sánchez M, Visnova H, Bosch E, García-Velasco JA, et al. Ovarian response to recombinant human follicle-stimulating hormone: a randomized, antimüllerian hormone-stratified, dose-response trial in women undergoing in vitro fertilization/intracytoplasmic sperm injection. Fertil Steril. 2014; 102: 1633.e5-1640.e5.
- Baart EB, Martini E, Eijkemans MJ, Van Opstal D, Beckers NG, Verhoeff A, et al. Milder ovarian stimulation for in-vitro fertilization reduces aneuploidy in the human preimplantation embryo: a randomized controlled trial. Hum Reprod. 2007; 22: 980-988.
- Esteves SC, Carvalho JF, Martinhago CD, Melo AA, Bento FC, Humaidan P, et al. Estimation of age-dependent decrease in blastocyst euploidy by next generation sequencing: development of a novel prediction model. Panminerva Med. 2019; 61: 3-10.
- Rafael F, Rodrigues MD, Bellver J, Canelas-Pais M, Garrido N, Garcia-Velasco JA, et al. The combined effect of BMI and age on ART outcomes. Hum Reprod. 2023; 38: 886-894.
- Belgian Register for Assisted Procreation (BELRAP). Annual report 2020. Brussels: BELRAP. 2022.










































































































































{kind=link}