Endometrioma
- 1. Department of Gynaecology-Obstetrics and Endoscopy, University Hospital Center IBN SINA, Morocco
- 2. Department of Gynaecology-Obstetrics and Endocrinology, University Hospital Center IBN SINA, Morocco
Abstract
Background: Endometriosis is a chronic inflammatory condition defined by the presence of ectopic endometrial tissue outside the uterus. It affects 6 to 15% of women worldwide and the clinical manifestations are diverse and linked to its location: abdomino-pelvic pain, infertility, urinary or digestive problems. Endometriosis affects women consulting for fertility problems and many have one or more endometriomas. They are more frequently associated with severe endometriosis, particularly in the context of infertility.
The management of endometriomas differs according to the symptomatology but also according to the related infertility problem. It is known that traditional cystectomy affects the ovarian reserve. We will describe through this case report ethanol sclerotherapy, highlighting its indications and advantages.
Case Presentation: We hereby present the case of a 32-year-old woman followed in our structure for primary infertility for two years and endometriosis. The spermogram of her husband, 10 years older than her, revealed severe oligo-asthenospermia. The indication for ICSI was therefore given. The patient presented with a painful endometrioma in the right ovary measuring 58x43mm with a typical ground glass appearance on endovaginal ultrasound. An abdomino-pelvic MRI did not reveal any other endometriotic location. To allow an oocyte puncture in good conditions, it was indicated to treat her endometrioma first. Ethanol sclerotherapy was chosen and was performed in our facility on an outpatient basis. The patient remained under surveillance for four hours after the intervention and then discharged home. Ovarian stimulation was started three weeks later, after ultrasound verification that the endometrioma had disappeared. No adverse effects were reported during or after the procedure.
Conclusions: Ethanol sclerotherapy is therefore an interesting alternative in the treatment of endometriomas to improve pregnancy rates in IVF. EST could therefore be discussed before IVF as a first-line treatment in infertile women with initially decreased ovarian reserve and painful endometrioma.
Keywords
Infertility, Endometrioma, Ethanol Sclerotherapy
ABBREVIATIONS
ICSI: Intra Cytoplasmic Sperm Injection; MRI: Magnetic Resonance Imaging; IVF: In Vitro Fertilization; EST: Ethanol ScleroTherapy; ESHRE: European Society of Human Reproduction
Citation
SLAOUI A, LOUZALI FZ, MAHTATE M, TALIB S, ZERAIDI N, et al. (2022) Endometrioma’s Ethanol Sclerotherapy is an Attractive Alternative to Surgery: About a Case Report. JSM Sexual Med 6(1): 1082.
BACKGROUND
Endometriosis is a chronic inflammatory condition defined by the presence of ectopic endometrial tissue outside the uterus. It affects 6 to 15% of women worldwide and the clinical manifestations are diverse and linked to its location: abdomino-pelvic pain, infertility, urinary or digestive problems. Endometriosis affects women consulting for fertility problems and many have one or more endometriomas. They are more frequently associated with severe endometriosis, particularly in the context of infertility.
The management of endometriomas differs according to the symptomatology but also according to the related infertility problem. It is known that traditional cystectomy affects the ovarian reserve. We will describe through this case report ethanol sclerotherapy, highlighting its advantages and indications.
CASE PRESENTATION
We hereby present the case of a 32-year-old woman followed in our structure for primary infertility of two years and endometriosis. The spermogram of her husband, 10 years older than her, revealed a severe oligo-asthenospermia. The indication of an ICSI was therefore made. The patient presented a painful endometrioma in the right ovary measuring 58x43mm with a typical ground glass appearance on endovaginal ultrasound (Figure 1). An abdomino-pelvic MRI did not reveal any other endometriotic localization. To allow oocyte puncture in good conditions, it was therefore indicated to first treat her endometrioma. Sclerotherapy by ethanol injection was chosen.
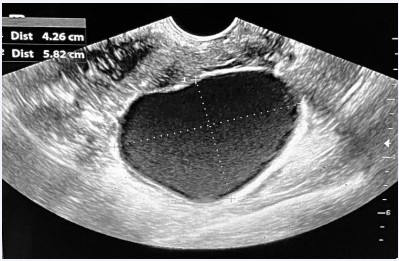
Figure 1: Ultrasound image showing the endometrioma in the right ovary measuring 58x43mm with a typical ground glass appearance.
The procedure was performed in our outpatient clinic, in the lithotomy position, by a trained gynecologist, under general anesthesia and transvaginal ultrasound control. Antibiotic prophylaxis with 2g of Cefazolin was administered. She had a sterile vaginal swab one week before the procedure. The position and size of the endometrioma were initially recorded, and then the endometrioma was punctured by transvaginal ultrasound guidance using a 17G x 250 mm single lumen oocyte puncture needle. The cyst contents were completely aspirated and the volume was measured at 76 mL. A portion of the fluid was sent to cytology for analysis. The cyst was rinsed twice with saline until a clear fluid was obtained. Ethanol at 96% was injected at 60% of the initial volume of the endometrioma, i.e. 45 mL, in order not to distend the cyst too much and to avoid its rupture and leakage of ethanol into the pelvis. The maximum volume of 96% ethanol tolerated for the intracystic injection of 60 mL was respected. The ethanol was then left in place in the cyst for 10 minutes and then completely reaspirated. There was 42 mL reaspirated with a negligible loss of 3 mL. The patient was kept under surveillance for four hours and then discharged home. Ovarian stimulation was started three weeks later, following ultrasound verification of the disappearance of the endometrioma. The procedure was considered a success since the remaining endometrioma was less than 20 mm on ultrasound within three months. We did not report any adverse effects during or after the procedure.
DISCUSSION
Endometriosis is a chronic inflammatory condition defined by the presence of ectopic endometrial tissue outside the uterus. It affects 6 to 15% of women worldwide [1]. The clinical manifestations are diverse and linked to its location: abdomino-pelvic pain, infertility, urinary or digestive problems [2]. Endometriosis affects 20% to 40% of women consulting for fertility problems [3,4]. Seventeen to 44% of women with endometriosis have one or more endometriomas [5]. They are more frequently associated with severe endometriosis, particularly in the context of infertility. In our patient, however, the workup did not reveal any other endometriotic manifestations except for a right endometrioma. The infertility of the couple was the consequence of the astheno-oligospermia of her 43-year-old husband.
The ovarian reserve is formed during fetal life, with a diminishing stock of definitive follicles from birth until menopause. Any alteration in the ovarian reserve is irreversible and may lead to premature ovarian failure [6]. Conventional laparoscopic endometrioma surgery with divergent traction cystectomy is likely to alter the ovarian reserve by excision of the surrounding ovarian cortex. Roustan et al. [7], showed that women with decreased ovarian reserve after cystectomy had lower live birth rates than a control group with idiopathically decreased ovarian reserve (7.2% vs. 16.9% respectively, p = 0.01). Concerning the management of endometriomas larger than 3 cm in infertile women, the international recommendations of the ESHRE do not recommend systematic cystectomy before IVF management because of the risks of altering the ovarian reserve without improving pregnancy rates [8]. If IVF is planned, it is currently recommended to leave the endometriomas in situ, except if the endometrioma is painful as in the case of our patient or if it masks the follicles, risking reducing the oocyte recovery rate [9].
However, performing oocyte retrieval with endometrioma(s) in situ is not trivial and may result in trans-endometriomal passage with possible contamination of the follicular fluid. This may decrease clinical pregnancy and live birth rates [RR = 0.63 (95% CI: 0.49-0.87, p = 0.005) and RR = 0.60 (95% CI: 0.51-0.86, p = 0.003)] [10]. In addition, Seyhan et al. [11], showed that the volume of endometrioma increased significantly during ovarian stimulation (22.2 ml (12-30 ml) vs. 24.99 ml (11.2-37.4 ml), p = 0.001)), and that endometrioma growth was correlated with the initial cyst volume before stimulation. Uncu et al. [12], showed that women with endometriomas, compared with a control group, had decreased AMH levels and antral follicle count (4.2 ± 2.3 ng/ml vs. 2.8 ± 2.2 ng/ml, p = 0.02 and 14.7 ± 4.1 ng/ml vs. 9.7 ± 4.8 ng/ml, p < 0.01, respectively).
Ethanol sclerotherapy is an old technique, first described in 1985 by Sarin et al. [13], to treat esophageal varices. Its mechanism of action is a combination of cytotoxic lesions, hypertonic dehydration of cells coagulation and thrombosis leading to fibrinoid necrosis [14]. Ethanol sclerotherapy of endometriomas was first described in 1988 by Akamatsu et al. [15], in Japan, and was later standardized by Yasbeck in 2012 [16,17]. In addition to ethanol [16,18-24], various agents have been used over the years to perform intracystic instillations with the aim of inducing direct destruction of the endometriosis present in the cyst wall: tetracycline [25] and methotrexate [26]. In their meta-analysis, Cohen et al. [27], found seven studies on EST and fertility using different protocols. Regarding clinical pregnancy rates, most of them compared laparoscopic cystectomy with sclerotherapy and found similar clinical pregnancy rates [OR = 1.63 (95% CI 0.91-2.9) 3 studies, 214 women, I 2 = 28%]. Regarding the number of oocytes recovered in women treated with or without sclerotherapy, no difference was found between groups [mean difference -0.51, (95% CI -2.23 to 1.21) 3 studies, 148 women, I2 = 17%] [27]. Regarding the retention of ethanol in the cystic duct after aspiration, a recent study published in 2021 by XX Huang et al. [28], showed a statistically significant decrease in AMH levels only in the group where ethanol was left in situ (3-10 mL) compared to the group of patients where there was less than 3 mL of ethanol loss. The authors concluded that the technique is more effective in preserving ovarian reserve if no ethanol remains in situ [28]. Although our single case is not significant, it is noted that similarly the AMH level decreased by only 3.7% six months after the procedure. Another study published in 2022 by Antonaci et al. [28], compared ovarian reserve, oocyte quality and pregnancy outcome between endometrioma treatment by laparoscopic stripping and EST in infertile women waiting in IVF. The authors concluded that the efficacy of EST was superior to LS for endometrioma, particularly on preservation of ovarian function [28].
CONCLUSIONS
Ethanol sclerotherapy is therefore an interesting alternative in the treatment of endometriomas to improve pregnancy rates in IVF. EST could therefore be discussed before IVF as a first-line treatment in infertile women with initially decreased ovarian reserve and painful endometrioma.










































































































































{kind=link}