Female Orgasmic Dysfunction and Gynecological Pathologies
- 1. Center for Reproductive Medicine “Universe”, Tbilisi, Georgia
- 2. Department of Obstetrics-Gynecology-Reproductology of Medical Faculty of Tbilisi State University, Georgia
- 3. Medical Corporation Evex, Tbilisi, Georgia
Abstract
Background: Despite of access data on influence of gynecological pathologies on development of sexual dysfunctions, there is no clear scientifically proved evidence on influence of sexual disorders, such as anorgasmia, on development of gynecological pathologies.
Objective: Objective of study was detection of relationship between women’s sexual functions (orgasm and libido) and gynecological pathologies.
Materials and methods: 676 sexually active women (aged 18-55yy, mean age 31, 7+3) have been investigated on the basis of Center for Reproductive Medicine “Universe” and outpatient clinics of Medical Corporation Evex. They were divided in 3 groups:I gr. – 148 women with ovarico-varicocele (OVVC), II gr. – 125 women with dilatation of myometrium veins (DMV) and III gr. - 403 women with other gynecological pathologies (myoma, inflammatory diseases, gynecological-endocrine disorders, etc.). In all groups frequency of orgasms (never, rare, often, always) and grade of libido (low, medium, high) have been assessed by interviewing.
Results: In I group rate of women with anorgasmia (70,9%) and rare orgasms (20,9%) was significantly higher (P<0.01) than rate women, who had orgasms often (6,1%) or always (2,0%). In II group rate of women with anorgasmia (39,2%) and rare orgasms (44,0%) was significantly higher (P<0.01) than women, who had orgasms often (12,8%) or always (4,0%). In III group generally was observed prevalence of women without absolute absence or presence of orgasms -rate of women, who had orgasms often (36,7%) or rarely (44,4%) was significantly higher (P<0.01) than women, who had orgasm always (5,2%) or never (13,6%). As of relationship between intensity of sexual drive (libido) and frequency of orgasms – in all groups there was inverse dependence - women with anorgasmia and rare frequency of orgasms mainly had low or medium libido and in women, who had orgasms often or always libido was mainly medium or high.
Conclusion: Orgasmic dysfunctions (anorgasmy) can promote congestive process in pelvis, development of varicosis of ovarian and pelvic veins (with corresponding other gynecological complications), which themselves can determine chronic pelvic pain that deepens the anorgasmic process.
In younger ages and early stages of beginning of sexual life, timely management of anorgasmy might be good prevention for further development of gynecological pathologies. The issue needs further investigation for revealing of cause-result relationship.
KEYWORDS
- Anorgasmy; Libido; Ovarico-varicocele; Dilatation of myometrium veins
CITATION
Kobaladze L, Kristesashvili J, Andguladze S (2021) Female Orgasmic Dysfunction and Gynecological Pathologies. JSM Sexual Med 5(3): 1074.
INTRODUCTION
Good sexual and reproductive health is a state of complete physical, mental and social well-being in all matters relating to the reproductive system [1]. Orgasmic dysfunction in women is one of the most important sexual disorders that determine decrease of quality of life in women as well as couples.
Frequency of female anorgasmia according to country data is very different [2-5]: USA – 26%, Australia - 29%, Turkey – 43%,Iran – 37%, Nigeria – 55%, Brazil - 21%, China - 31%.Dr. Elisabeth A. Lloyd summarized 32 studies conducted over 70+ years, on the frequency of women’s orgasms with intercourse- intercourse alone, not orgasm with additional direct clitoral stimulation – anorgasmy - 5-10% [6].
There is a huge data base on causes of sexual dysfunctions in women, indicating on most frequent factors such as anatomic, hormonal, vascular, neurological, psycho-emotional, situational, data, it’s possible to conclude that the endometriosis leads to a significant disruption of sexual health of women and marital relations and correspondingly reduced quality of life for both partners [8-10].
Despite of access data on influence of gynecological pathologies on development of sexual dysfunctions, we couldn’t find scientifically proved evidence on influence of sexual disorders, such as anorgasmia, on development of gynecological pathologies. Only in few articles, dedicated to varicose extension of pelvic veins (VEPV), dyspareunia and anorgasmia are indicated as risk factors for development of VEPV [11,12].
For us logical chain was under question-mark:in sexual response cycle during excitement and plateau phases blood supply of pelvic organs increases and orgasm is the retraction mechanism for shedding blood back from these organs during resolution phase. In case of anorgasmic coitus, blood stays in pelvic organs for longer time, causing venous stasis and correspondingly pelvic congestion syndrome, that itself can determine development of ovaricovaricocele and dilatation of myometrium veins Figures 1 and 2.
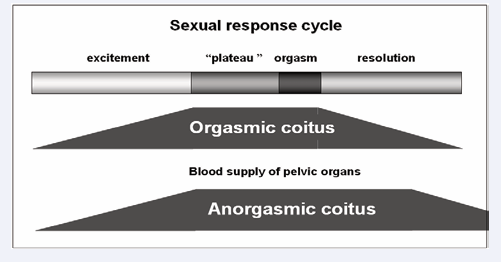
Figure 1: Blood supply of pelvic organs during anorgasmia in women.
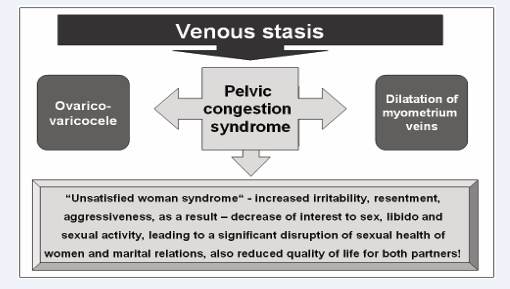
Figure 2: Anorgasmia in women – possible results.
Based on above-mentioned, objective of our study was detection of relationship between women’s sexual functions (orgasm and libido) and gynecological pathologies. relationship problems, chronicle diseases, pharmaceuticals, aging, etc [6].
Well investigated is also the role of gynecological pathologies and pain related to them in development of sexual disorders.
According to Fugl-Meyer KS & Fugl-Meyer AR [7] a lot of women, who report manifested sexual genital pain, also report: low level of sexual interest (67%), insufficient vaginal lubrication (61%), manifested orgasmic dysfunction (48%), vaginismus (9%).
Several studies indicate on direct influence of endometriosis on development of sexual dysfunctions in women [8-10]. Stenyaeva N and co-authors in their study of women with endometriosis revealed that in the structure of sexual dysfunctions prevailed deep dyspareunia (87.1%), decreased libido (83.3%), coital anorgasmia (80.6%), accompanied by disruption in sexual adaptation in pair (93.5%). All patients demonstrated depression and anxiety. On the bases of literature
MATERIALS AND METHODS
676 sexually active women (aged 18-55yy, mean age 31,7+3) have been investigated on the basis of Center for Reproductive Medicine “Universe” and outpatient clinics of Medical Corporation Evex. They were divided in 3 groups:I gr. – 148 women with ovarico-varicocele (OVVC), II gr. – 125 women with dilatation of myometrium veins (DMV) and III gr. - 403 women with other gynecological pathologies (myoma, inflammatory diseases, gynecological-endocrine disorders, etc.).
Diagnosis of patients was based on analysis of patient records. Diagnosis of OVVC and DMV were based on results of iinvestigation by transvaginal US of the pelvic venous system with Doppler examination of blood flow in the uterine veins.
In all groups frequency of orgasms (never, rare, often, always) and grade of libido (low, medium, high) have been assessed by interviewing.
Statistical analysis was conducted by SPSS.21. The independent t-test was used for variables, e.g. age, duration of sexually active years and frequency of intercourse per month. Pearson Chi-square test was performed for comparing categorial data. Conclusions of study results were based on statistically reliable results in 95% confidence interval – P<0,05).
RESULTS
There were no statistically significant differences (P>0.05) in women with different frequency of orgasms in age, sexually active years, number of intercourses per month (Tables 1-3).
|
Table 1: Association of age, sexually active years and number of intercourses per month with frequency of orgasms (Total number of investigated women – 676). |
|||||
|
Orgasm |
Number of women |
Mean age |
Mean duration of sexually active years |
Mean number of intercourses per month |
|
|
abs |
% |
||||
|
Always |
29 |
4.3 |
29.7+2.1 |
7.7+0.8 |
19.7+1.4 |
|
Often |
173 |
25.6 |
30.3+1.9 |
6.8+0.6 |
16.8+1.5 |
|
Rare |
265 |
39.2 |
32.5+2.4 |
9.8+1.0 |
14.6+1.3 |
|
Never |
209 |
30.1 |
34.4+2.5 |
11.2+1.2 |
12.2+0.9 |
|
Total |
676 |
100 |
31,7+2.2 |
8.9+0.9 |
15.8+1.3 |
|
Table 2: Assessment of orgasm according to groups. |
|||||||||
|
Orgasm |
I group |
II group |
III group |
P1 |
P2 |
P3 |
|||
|
abs. |
% |
abs. |
% |
abs. |
% |
||||
|
Always |
3 |
2.0 |
5 |
4.0 |
21 |
5.2 |
P<0.01 |
P<0.01 |
P<0.05 |
|
Often |
9 |
6.1 |
16 |
12.8 |
148 |
36.7 |
P<0.01 |
P<0.01 |
P<0.01 |
|
Rarely |
31 |
20.9 |
55 |
44.0 |
179 |
44.4 |
P<0.01 |
P<0.01 |
P>0.05 |
|
Never |
105 |
70.9 |
49 |
39.2 |
55 |
13.6 |
P<0.01 |
P<0.01 |
P<0.01 |
|
Total |
148 |
100 |
125 |
100 |
403 |
100 |
|
|
|
|
P1 – difference between I gr and II gr P2 – difference between I gr and III gr P3 – difference between II gr and III gr |
|||||||||
|
Table 3: Assessment of libido according to groups. |
|||||||||
|
Libido |
I group |
II group |
III group |
P1 |
P2 |
P3 |
|||
|
abs. |
% |
abs. |
% |
abs. |
% |
||||
|
Low |
49 |
33.1 |
44 |
35.2 |
140 |
34.7 |
P>0.05 |
P>0.05 |
P>0.05 |
|
Medium |
63 |
42.6 |
57 |
45.6 |
168 |
41.7 |
P>0.05 |
P>0.05 |
P>0.05 |
|
High |
36 |
24.3 |
24 |
19.2 |
95 |
23.6 |
P>0.05 |
P>0.05 |
P>0.05 |
|
Total |
148 |
100 |
125 |
100 |
403 |
100 |
|
|
|
|
P1 – difference between I gr and II gr P2 – difference between I gr and III gr P3 – difference between II gr and III gr |
|||||||||
Assessment of orgasms in different groups revealed significant prevalence of anorgasmia in I and II groups, comparing to III group.
There were no statistically significant differences (P>0.05) in any group between frequencies of grades of libido
Sexological evaluation of women according to groups
In I group (women with ovarico-varicocele) rate of women with anorgasmia (70,9%) and rare orgasms (20,9%) was significantly higher (P<0.01) than rate women, who had orgasms often (6,1%) or always (2,0%).
As of relationship between intensity of sexual drive (libido) and frequency of orgasms – there was inverse dependence - women with anorgasmia (70,9%) and rare frequency of orgasms (20,9%) mainly had low (38,7-41,9%) or medium (35,2-43,8%) libido and in women, who had orgasms often (6,1%) or always (2,0%) libido was mainly medium (44,4-55,6%) or high (100%) (Table 4).
|
Table 4: Sexological evaluation of women in I group. |
||||||||
|
Orgasm |
Number of women |
Libido low |
Libido medium |
Libido high |
||||
|
abs |
% |
abs |
% |
abs |
% |
abs |
% |
|
|
Always |
3 |
2.0 |
|
|
|
|
3 |
100 |
|
Often |
9 |
6.1 |
|
|
4 |
44.4 |
5 |
55.6 |
|
Rarely |
31 |
20.9 |
12 |
38.7 |
13 |
41.9 |
6 |
19.4 |
|
Never |
105 |
70.9 |
37 |
35.2 |
46 |
43.8 |
22 |
21.0 |
|
Total |
148 |
100 |
49 |
|
63 |
|
36 |
|
In II group (women with dilatation of myometrium veins) rate of women with anorgasmia (39,2%) and rare orgasms (44,0%) was significantly higher (P<0.01) than women, who had orgasms often (12,8%) or always (4,0%).
As of relationship between intensity of sexual drive (libido) and frequency of orgasms – in this group also there was inverse dependence - women with anorgasmia (39,2 %) and rare frequency of orgasms (44,0 %) mainly had low (20,0-59,2%) or medium (40,8-52,7%) libido and in women, who had orgasms often (12,8%) or always (4,0%) libido was mainly medium (20,0- 43,8%) or high (20,0-80,0%) (Table 5).
|
Table 5: Sexological evaluation of women in II group. |
||||||||
|
Orgasm |
Number of women |
Libido low |
Libido medium |
Libido high |
||||
|
abs |
% |
abs |
% |
abs |
% |
abs |
% |
|
|
Always |
5 |
4.0 |
0 |
0 |
1 |
20 |
4 |
80 |
|
Often |
16 |
12.8 |
4 |
25.0 |
7 |
43.8 |
5 |
31.3 |
|
Rarely |
55 |
44.0 |
11 |
20.0 |
29 |
52.7 |
15 |
27.3 |
|
Never |
49 |
39.2 |
29 |
59.2 |
20 |
40.8 |
0 |
0 |
|
Total |
125 |
100 |
44 |
|
57 |
|
24 |
|
In III group generally we observed prevalence of women without absolute absence or presence of orgasms - rate of women, who had orgasms often (36,7%) or rarely (44,4%) was significantly higher (P<0.01) than women, who had orgasm always (5,2%) or never (13,6%);
As of relationship between intensity of sexual drive (libido) and frequency of orgasms – in this group also there was inverse dependence, but not so expressed as in I and II groups - women with anorgasmia (13,6 %) and rare frequency of orgasms (44,4%) mainly had low (41,9-49,1%) or medium (23,6-45,3%) libido and in women, who had orgasms often (36,7%) or always (5,2%) libido was mainly medium (14,3-48,0%) or high (26,4-85,7%) (Table 6).
|
Table 6: Sexological evaluation of women in III group. |
||||||||
|
Orgasm |
Number of women |
Libido low |
Libido medium |
Libido high |
||||
|
abs |
% |
abs |
% |
abs |
% |
abs |
% |
|
|
Always |
21 |
5.2 |
0 |
0 |
3 |
14.3 |
18 |
85.7 |
|
Often |
148 |
36.7 |
38 |
25.7 |
71 |
48.0 |
39 |
26.4 |
|
Rarely |
179 |
44.4 |
75 |
41.9 |
71 |
45.3 |
23 |
12.8 |
|
Never |
55 |
13.6 |
27 |
49.1 |
13 |
23.6 |
15 |
27.3 |
|
Total |
403 |
100 |
140 |
|
168 |
|
95 |
|
DISCUSSION
Study results provide fruitful field for analysis and discussion. Prevalence of anorgasmia and rare frequency of orgasms in women with OVVC and DMV might be considered as an evidence of causal influence of anorgasmic coitus on development of congestive processes in small pelvis with further development of varicose changes of ovarian veins and dilatation of myometrium veins. Itself OVVC and DMV might be good bases for amplification of other gynecological pathologies and conditions.
Ovarian varicose veins characterize themselves in the form of dilated, tortuous and congested veins next to the ovarian gland, often causing chronic pelvic pain and a feeling of heaviness in the pelvis in women [13,14].
Several studies have demonstrated that over 50% of patients with ovarian varicose veins have polycystic ovaries [15-30] and that the morphologic and functional change in the polycystic ovary syndrome increases the risk of cancer [16,18], venous thrombosis [17,18], infertility and cardiovascular problems [19], as well as decreasing the ovarian reserve16.
Increased oxidative stress (OS) in varicose dilations provokes histological damage in the ovaries and suggests a negative effect related to fertility [20]. Moreover, researchers have also evidenced that female infertility may increase the risk of cancer and other pathologies [21,22].
Some authors have demonstrated the frequency of ovarian varicose veins in women by pathology: in women who suffered from chronic pelvic pain, the prevalence was of 50% [23,24], in women with endometriosis, the prevalence was of 80% [25], in women who had endometriomas in the left ovary, the prevalence was of 100% [26].
The therapeutic test suggests that varicose veins cause destruction of tissue and organs, OS in endothelial cells and, as a result of these damages, the alteration of the expression of several genes [27-29].
Congestive processes in pelvis can influence on varicose dilatation of pelvic veins including myometrium veins [30,31] that might be complicated with thrombosis, development of cystic and malignant formations [32,33].
Congestive processes and varicose of ovarian or pelvic veins often are causes of chronic pelvic pain [34,35], that in turn can influence on orgasmic functions and determine anorgasmy.
Summarizing all above-mentioned, we can conclude that orgasmic dysfunctions (anorgasmy) can promote congestive process in pelvis, development of varicosis of ovarian and pelvic veins (with corresponding other gynecological complications), which themselves can determine chronic pelvic pain that deepens the anorgasmic process. So, locked, vicious circle is forming and only strategy to manage this situation is complex approach for treating all components and conditions. Also in younger ages and early stages of beginning of sexual life, timely management of anorgasmy might be good prevention for further development of gynecological pathologies.
REFERENCES
- www.unfpa.org/sexual-reproductive-health.
- Abdo CH, Oliveira WM Jr, Moreira ED Jr, Fittipaldi JA. Prevalence of sexual dysfunctions and correlated conditions in a sample of Brazilian women--results of the Brazilian study on sexual behavior (BSSB). Int J Impot Res. 2004; 16: 160-6.
- Najafabady MT, Salmani Z, Abedi P. Prevalence and related factors for anorgasmia among reproductive aged women in Hesarak, Iran. Clinics (Sao Paulo). 2011; 66: 83-86.
- Ojomu F, Thacher TD, Obadofin M. Sexual problems among married Nigerian women. International Journal of Impotence Research. 2007; 19: 310-6.
- Elisabeth A. Lloyd. The Case of the Female Orgasm: Bias in the Science of Evolution. 2005.
- Women’s Sexual Function and Dysfunction: Study, Diagnosis and Treatment. By Irwin Goldstein, Cindy M. Meston, Susan Davis, Abdulmaged Traish. 2006.
- Fugl-Meyer KS, Fugl-Meyer AR. Sexual disabilities are not singularities. Int J Impot Res. 2002; 14: 487–93.
- Jia SZ, Leng JH, Sun PR, Lang JH. Prevalence and associated factors of female sexual dysfunction in women with endometriosis. Obstet Gynecol. 2013; 121: 601-6.
- Fritzer N, Haas D, Oppelt P, St Renner, D Hornung, M Wölfler, et al. More than just bad sex - sexual dysfunction and distress in patients with endometriosis. Eur J Obstet Gynecol Reprod Biol. 2013; 169: 392-6.
- Stenyaeva N, Chritinin D, Sukhikh G. Open cross-sectional study of mental and sexual helth in women with endometriosis. 16th World Congress on Human Reproduction. 2015.
- Artymuk N.V.. Female small pelvic varicose veins.
- Varicose dilatation of myometrial veins - symptom or disease?
- Mathias SD, Kuppermann M, Liberman RF, et al. Chronic pelvic pain: prevalence, health-related quality of life, and economic correlates. Obstet Gynecol. 1996; 87: 321-7.
- Beard RW, Highman JH, Pearce S, Reginald PW. Diagnosis of pelvic varicosities in women with chronic pelvic pain. Lancet. 1984; 2: 946-9.
- Elizabeth A Ignacio, Ruchika Dua, Shawn Sarin, Amy Soltes Harper, Douglas Yim, Vivek Mathur, et al. Pelvic Congestion Syndrome: Diagnosis and Treatment. Semin Intervent Radiol. 2008; 25: 361–368.
- Zuo T, Zhu M, Xu W. Roles of Oxidative Stress in Polycystic Ovary Syndrome and Cancers. Oxid Med Cell Longev. 2016; 2016: 8589318.
- Okoroh EM, Hooper WC, Atrash HK, Yusuf HR, Boulet SL. Is polycystic ovary syndrome another risk factor for venous thromboembolism? United States, 2003-2008. Am J Obstet Ginecol. 2012; 207: 377.
- Pacheco KG, de Oliveira MRF, Pacheco MF. The Role of Ovarian Varicose Veins and Varicocele in Cancer and Venous Thrombosis. J Gyn Research. 2018; 4: 1.
- Wiltgen D, Spritzer PM. Variation in metabolic and cardiovascular risk in women with different polycystic ovary syndrome phenotypes. 91st Annual Meeting of the Endocrine Society, June 10–13, 2009, Washington, DC.
- Kehinde BA, Abolhassani F, Yazdekhasti H, et al. The effects of unilateral varicose ovarian vein on antioxidant capacity and oocyte quality in rat ovary. Iran J Basic Med Sci. 2016; 19: 863-869.
- Tarín JJ, García-Pérez MA, Hamatani T, Cano A. Infertility etiologies are genetically and clinically linked with other diseases in single meta- diseases. Reprod Biol Endocrinol. 2015; 13: 31.
- Buis CC, van Leeuwen FE, Mooij TM, Burger CW. Increased risk for ovarian cancer and borderline ovarian tumors in subfertile women with endometriosis. Hum Reprod. 2013; 28: 3358-69.
- Giacchetto C, Cotroneo GB, Marincolo F, F Cammisuli, G Caruso, F Catizone. Ovarian varicocele: ultrasonic and phlebographic evaluation. J Clin Ultrasound. 1990; 18: 551-5.
- Seong Jin Park, Joo Won Lim, Young Tae Ko, et al. Diagnosis of Pelvic Congestion Syndrome Using Transabdominal and Transvaginal Sonography. Gynecologic and Obstetric Imaging. 2004; 182.
- Pacheco KG, de Oliveira MRF. The Prevalence of Ovarian Varices in Patients with Endometriosis. Ann Vasc Surg. 2016; 34: 135-143.
- Matalliotakis IM, Cakmak H, Koumantakis EE, Anastasia Margariti, Maria Neonaki, Anastasia G Goumenou, et al. Arguments for a left lateral predisposition of endometrioma. Fertil Steril. 2009; 91: 975-8.
- Murphy MA, Joyce WP, Condron C, D Bouchier-Hayes. A reduction in serum cytokine levels parallels healing of venous ulcers in patients undergoing compression therapy. Eur J Vasc Endovasc Surg. 2002; 23: 349-52.
- Flore R, Santoliquido A, Antonio DL, Enrico Pola, Andrea Flex, Roberto Pola, et al. Long saphenous vein stripping reduces local level of reactive oxygen metabolites in patients with varicose disease of the lower limbs. World J Surg. 2003; 27: 473-5.
- Horecka A, Biernacka J, Hordyjewska A, et al. Antioxidative mechanism in the course of varicose veins. Phlebology. 2018; 33: 464-469.
- Adams J, Reginald PW, Franks S, Wadsworth J, Beard RW. Uterine size and endometrial thickness and the significance of cystic ovaries in women with pelvic pain due to congestion. Br J Obstet Gynaecol. 1990; 97:583 –587
- Gultaply NZ, Kurt A, Ýpek A, et al. The relation between pelvic varicose veins, chronic pelvic pain, and lower extremity venous insufficiency in women. Phlebolymphology. 2008; 15: 61-67.
- Beard RW, Highman JH, Pearce S, Reginald PW. Diagnosis of pelvic varicosities in women with chronic pelvic pain. Lancet. 1984; 2: 946- 949.
- Uotila J, Dastidar P, Martikainen P, P Kirkinen. Massive multicystic dilatation of the uterine wall with myometrial venous thrombosis during pregnancy. Ultrasound Obstet Gynecol. 2004; 24: 461-3.
- Park SJ, Lim JV, Ko YT, Dong Ho Lee, Yup Yoon, Joo Hyoung Oh, et al. Diagnosis of pelvic congestion syndrome using transabdominal and transvaginal sonography. Am J Roentgenol. 2004; 182: 683-688.
- Kuligowska E, Deeds L, Lu K. Pelvic pain: overlooked and underdiagnosed gynecologic conditions. Radiographics. 2005; 25:3-20.










































































































































{kind=link}