Intensive Multimodal Penile Rehabilitation after Nerve-Sparing Robotic Radical Prostatectomy: Insights from the PEHAB-I Feasibility Study
- 1. Netherlands Cancer Institute- Antoni van Leeuwenhoek Hospital, Urology, The Netherlands
- 2. Amsterdam University Medical Centres, Urology, The Netherlands
- 3. Leiden University Medical Centre, Urology, The Netherlands
Citation
Cox IL, van Muilekom EAM, Vis AN, van Leeuwen PJ, Elzevier HW, et al. (2026) Intensive Multimodal Penile Rehabilitation after Nerve Sparing Robotic Radical Prostatectomy: Insights from the PEHAB-I Feasibility Study. JSM Sexual Med 10(1): 1175.
ABBREVIATIONS
AP: Adherent Patients; BMI: Body Mass Index; DO: Dropouts; ED: Erectile Dysfunction; EAU: European Association of Urology; EF: Erectile Function; EHS: Erection Hardness Score; FP-score/FP: Fascia Preservation Score; FU: Follow up; ICI: Intracavernosal Injection; IIEF: International Index of Erectile Function; IIEF EF: International Index of Erectile Function – Erectile Function Domain; IQR: Interquartile Range; IRBd: Institutional Review Board Designation; ISUP: International Society of Urological Pathology; mg: Milligram; mo: Months; NAP: Non Adherent Patients; NCI: Netherlands Cancer Institute; NVB: Neurovascular Bundle; ns: Nerve-sparing; nsRP: Nerve-sparing Radical Prostatectomy; OD: On demand; PCa: Prostate Cancer; PDE5i: Phosphodiesterase Type 5 Inhibitor; PROM: Patient Reported Outcome Measure; PSA/ iPSA: (Initial) Prostate Specific Antigen; pT: Pathological Tumor Stage; RCT: Randomized Controlled Trial; RARP: Robot Assisted Radical Prostatectomy; RP: Radical Prostatectomy; SD: Standard Deviation; TIA: Transient Ischaemic Attack; VED: Vacuum Erection Device; yr: Year
INTRODUCTION
Robot-assisted radical prostatectomy (RP) demonstrates excellent oncologic outcomes for men with localized prostate cancer (PCa) [1]. However, post-operative challenges in achieving satisfactory erectile function (EF)—defined as the ability to achieve and maintain an erection [2], are common among patients, primarily due to damage to the neurovascular bundle (NVB) responsible for erections. This decline in EF after RP is often accompanied by impaired mental well-being and reduced self-esteem, negatively impacting patients’ quality of life [3-5]. Despite attempts to improve NVB sparing, such as the neurovascular structure-adjacent frozen-section examination (NeuroSAFE, which appears to yield favorable results in improving EF recovery [6-12], the rate of EF recovery after bilateral nerve-sparing surgery without the use of phosphodiesterase 5 inhibitors (PDE5i) remains relatively low, ranging from 7% to 47.7% (10-12). Ongoing erectile dysfunction (ED) in these patients is caused by temporary or permanent neuronal damage, which can take up to four years to heal, or may not recover at all [13,14]. Consequently, corporal tissue fibrosis develops, causing the tissue to lose functionality by the time the nerves have recovered [15]. To improve neuronal recovery and prevent corporal tissue fibrosis, rehabilitation therapies have been explored. According to literature, unimodal rehabilitation therapies using high daily doses of PDE5i or penile vacuum devices (VED) are potentially associated with better EF recovery compared to placebo one year post surgery [16-18]. However, multimodal prospective studies on the combination of high-dose sildenafil, VED use, and optional injection therapy, or those with longer follow-up periods allowing more neuronal recovery time, are still lacking [19-23]. Additionally, adherence to each individual erectile aid in existing less intensive multimodal rehabilitation strategies varied widely, from 40% to 100% [21, 23], making it difficult to determine the true effect of the rehabilitation program on EF. Therefore, further investigation is needed to understand the impact on adherence, side effects, and EF when combining a novel rehabilitation strategy involving a daily high PDE5i dosage with an intensive VED regimen within a dedicated counselling program, before performing a well-powered randomized trial. The primary aim of this feasibility study was to assess adherence to an intensive multimodal rehabilitation program. Additionally, inclusion rates, dropout rates, and a preliminary estimation of the intervention’s effect were also considered key feasibility indicators, as they reflect the intervention’s acceptability and logistical practicality. The program included relatively high doses of sildenafil (75-100 mg), nearly daily use of a VED, optional intracavernosal injection therapy (ICI), and regular guidance from a urologist specialized in andrology or a specialized andrology-oriented nurse.
MATERIALS AND METHODS
Study design
This prospective single-centre feasibility study evaluated a penile rehabilitation program after nerve sparing radical prostatectomy (nsRP) at the Netherlands Cancer Institute (July 2021–June 2024). All patients underwent at least full unilateral nsRP in a high-volume centre (≥400 a year). Approval for this study from the Institutional Review Board was obtained (IRBd21-070). All patients signed informed consent.
Inclusion and exclusion criteria
All eligible nsRP patients interested in improving their sexual health were referred to the outpatient clinic for sexual health. Referral occurred within four mo post surgery to minimize fibrosis. Inclusion criteria included satisfactory preoperative anamnestic EF (defined as the ability to penetrate and maintain an erection), a serum testosterone >8 nmoll/L, and at least one-sided nerve sparing surgery. Exclusion included pelvic radiotherapy, hormonal therapy, contraindications for sildenafil or VED, systemic neurological disorders, or good postoperative EF.
The penile rehabilitation program and follow up
The rehabilitation program started after full recovery from nsRP. For the first 12 mo, patients used daily sildenafil (75-100 mg) and performed VED therapy at least five sessions per week, creating five erections per session and maintaining each for two minutes. Both sildenafil and VED (ACTIVE erection systemNT® (Kessels Medintim and Memidis Pharma)) were provided free of charge. Patients could use the VED and constriction ring for intercourse and to prevent climacturia. Unsatisfied patients were offered ICI therapy, and all were referred to a pelvic floor physiotherapist. The program was de-intensified or stopped if patients reported satisfactory spontaneous erections, defined as EHS ≥ 3 and maintained long enough for satisfactory sexual activity. Depending on the frequency of these satisfactory spontaneous erections the use of VED and sildenafil was reduced or even stopped, i.e. in case of daily morning erections.
Definitions of Adherence, Non-adherence and dropout
If Patients experienced severe side effects of sildenafil 100mg, they were allowed to reduce the dose to 75mg. Patients were classified as adherent, non-adherent, or dropouts. Full adherence was defined as daily sildenafil and VED use as prescribed or physician-approved de intensification. Non-adherence included insufficient use of Sildenafil (i.e. lower dose) or VED (i.e. less than 5 times/ week); discontinuation classified as drop-out.
Primary and secondary outcome measures
Primary outcome was adherence rate throughout the 12-mo rehabilitation program. Secondary outcomes were inclusion rate, dropout rate (i.e. due to side effects) and the potential effect of the program (including adherence) on satisfactory EF. Adherence and side effects were assessed at 2 weeks, 3, 6, and 12 mo after program initiation. EF was evaluated at 3, 6, 12, and 18 mo using the Erection Hardness Score (EHS) after program initiation, and using the IIEF-EF at 6, 12, and 18 mo post-nsRP (only in patients engaging in penetrative sex). At 18 mo, program satisfaction, treatment satisfaction, and climacturia (with or without a constriction ring) were assessed.
Statistical analysis
Baseline normality was assessed using the Kolmogorov Smirnov test, Q–Q plots, and Levene’s test. Categorical data are presented as n (%), and continuous data as mean (SD) or median (IQR), depending on distribution. Differences in baseline characteristics and EF at 18 mo between adherent, non-adherent, and dropout groups were analyzed using Student’s t-test, Mann–Whitney U-test, Pearson’s Chi squared test, or Fisher’s exact test, as appropriate. All analyses were performed in RStudio (2024).
RESULTS
Baseline characteristics
Of the 66 referred eligible patients, 51 (77,3%) were enrolled in the study. The main known reasons for non inclusion were prior start of rehabilitation (n=4) and unwillingness to commit to program intensity (n=4) (Figure 1).

Figure 1 Flow chart: presenting amount of dropouts at each time point. FU = Follow up. This figure gives an overview of dropout and dropout reasons throughout follow up.
The baseline characteristics of enrolled patients are summarized in Table 1.
Table 1: Baseline characteristics of all included patients.
|
|
Total N=51 |
Completed FU N=41 |
DO N=10 |
p Value |
|
|
|
|
AP N=24 |
NAP N=17 |
|
|
|
Age at start (yr), mean (SD) |
61.9 (6.1) |
59.9 (6.0) |
63.4 (6.1) |
63.8 (5.61) |
0.091 |
|
Partner, no. (%) |
|
|
|
|
|
|
Female partner |
43 (84.3) |
18 (75.0) |
17 (100) |
8 (80.0) |
0.087 |
|
No partner |
8 (15.7) |
6 (25.0) |
0 (0) |
2 (20.0) |
|
|
Race, no. (%) |
|
|
|
|
|
|
Caucasian |
47 (92.2) |
22 (91.7) |
15 (88.2) |
10 (100.0) |
0.570 |
|
Surinam |
3 (5.9) |
1 (4.2) |
2 (11.8) |
0 (0.0) |
|
|
Middle Eastern |
1 (2.0) |
1 (4.2) |
0 (0.0) |
0 (0.0) |
|
|
BMI (kg/m2), mean (SD) |
26.3 ( 2.9) |
26.0 (3.0) |
26.5 (3.4) |
26.7 (1.9) |
0.759 |
|
Testosterone (nmol/l), median (IQR) |
15.1 (12.1-18.2) |
16.1 (12.0- |
14.6 (11.6- |
14.2 (13.5 - 18.2) |
0.534 |
|
19.3) |
16.3) |
||||
|
EAU risk classification, no. (%)a |
|
|
|
|
|
|
Intermediate risk High risk |
41 (80.4) 10 (19.6) |
19 (79.2) 5 (20.8) |
13 (76.5) 4 (23,5) |
9 (90.0) 1 (10.0) |
0.679 |
|
pT Stage, no. (%) |
|
5 (20.8) 2 (8.3) 6 (25.0) 11 (45.8) |
2 (11.8) 1 (5.9) 11 (64.7) 3 (17.6) |
0 (0.0) 1 (10.0) 3 (30.0) 6 (60.0) |
|
|
T2a T2b |
7 (13.7) 4 (7.8) |
0.120 |
|||
|
T2c |
20 (39.2) |
|
|||
|
T3a |
20 (39.2) |
|
|||
|
ISUP Score, no. (%) |
|
|
|
1 (10.0) 6 (60.0) 1 (10.0) 1 (10.0) 1 (10.0) |
|
|
ISUP 1 |
3 (5.9) |
2 (8.3) |
0 (0.0) |
|
|
|
ISUP 2 |
35 (68.6) |
19 (79.2) |
10 (58.8) |
0.081 |
|
|
ISUP 3 |
10 (19.6) |
2 (8.3) |
7 (41.2) |
|
|
|
ISUP 4 |
2 (3.9) |
1 (4.2) |
0 (0.0) |
|
|
|
ISUP 5 |
1 (2.0 |
0 (0.0) |
0 (0.0) |
|
|
|
Pelvic lymph node dissection, no. (%) |
11 (21.6) |
4 (16.7) |
2 (11.8) |
5 (50.0) |
0.048 |
|
Positive lymph nodes, no. (%) |
- |
- |
- |
- |
- |
|
NeuroSAFE, no. (%) |
26 (51) |
12 (50.0) |
8 (47.1) |
6 (60.0) |
0.803 |
|
Degree of nerve sparingb, no. (%) |
|
|
|
|
|
|
Full unilateral Partial bilateral |
13 (25.5) 22 (43.1) |
4 (16.7) 12 (50.0) |
7 (41.2) 3 (17.6) |
2 (20.0) 7 (70.0) |
0.061 |
|
Full bilateral |
16 (31.4) |
8 (33.3) |
7 (41.2) |
1 (10.0) |
|
|
Preoperative IIEF-EFc, median (IQR) Not available, no. (%) |
29 (24.0-30.0) 16 (31.4) |
29.0 (26.5- 30.0) 9 (37.5) |
29.0 (20.0- 30.0) 4 (23.5) |
27.0 (24.0-28.0) 3 (30.0) |
0.319 |
|
Cardiovascular diseases, no. (%) |
15 (29.4) |
6 (25.0) |
6 (35.3) |
3 (30.0) |
0.775 |
|
Hypertension |
9 (17.6) |
5 (20.8) |
4 (23.5) |
0 (0.0) |
0.257 |
|
Myocardial infarction |
1 (2.0) |
0 (0.0) |
0 (0.0) |
1 (10.0) |
0.124 |
|
Hypercholesterolemia |
4 (7.8) |
1 (4.2) |
1 (5.9) |
2 (20.0) |
0.275 |
|
TIA |
1 (2.0) |
0 (0.0) |
1 (5.9) |
0 (0.0) |
0.361 |
|
Diabetes, no. (%) |
2 (3.9) |
0 (0.0) |
2 (11.8) |
0 (0.0) |
0.125 |
|
Smoking, no. (%) |
|
|
|
|
|
|
No |
32 (62.7) |
14 (58.3) |
11 (64.7) |
7 (70.0) |
0.452 |
|
Yes, former |
16 (31.4) |
7 (29.2) |
6 (35.3) |
3 (30.0) |
|
|
Yes, current |
3 (5.9) |
3 (12.5) |
0 (0.0) |
0 (0.0) |
|
|
Exercise, no. (%) |
|
|
|
|
|
|
Almost no exercise <3 times a week, 30 min |
12 (31.6) 15 (39.5) |
5 (20.8) 7 (29.2) |
4 (23.5) 7 (41.2) |
3 (30.0) 1 (10) |
0.623 |
|
>3 times a week, 30 min |
11 (28.9) |
5 (20.8) |
3 (17.6) |
3 (30.0) |
|
|
Unknown |
13 (25.5) |
7 (29.2) |
3 (17.6) |
3 (30.0) |
|
|
Climacturia, no. (%) Yes |
7 (13.7) |
1 (4.2) |
4 (23.5) |
2 (20.0) |
0.128 |
|
Unknown |
12 (23.5) |
5 (20.8) |
3 (17.6) |
4 (40.0) |
|
|
Start program (weeks), median (IQR) |
6.0 (5.0 – 8.5) |
6.0 (5.0- 9.0) |
7.00 (5.0- 9.0) |
5.5 (5.0-6.0) |
0.525 |
FU= Follow-up; DO= Dropouts; AP = adherent patients, NAP; Non adherent patients; SD= Standard deviation; IQR= Interquartile range; BMI= body mass index; iPSA= Initial prostate-specific antigen; EAU= European Association of Urology; ISUP = International Society of Urological pathology; NeuroSAFE = Neurovascular Structure Adjacent Frozen Section Examination; FP-score= Fascia-preservation score; IIEF-EF= international index of erectile function- erectile function domain; TIA= transient ischaemic attack.
Patients have been divided in adherent, non-adherent and dropouts based on their adherence or discontinuation throughout the first 12 mo of follow-up.
a Classified according to the EAU guidelines, using iPSA, clinical tumor stadium and gleason score obtained by biopsies (25).
b In our centre, the fascia preservation (FP) score is used to specify nerve sparing (19). FP-score of 5 or 6 one sided was classified as full unilateral nerve sparing, FP-score of 5 or 6 on both sides was classified as full bilateral nerve sparing, everything in between was classified as partial bilateral nerve sparing.
c Only the IIEF-EF scores of patients who participated in penetrative intercourse are shown.
Mean age was 61.9 years (SD 6.1), 84% (n=43) had a female sexual partner at baseline. Overall, most patients were relatively healthy. Median testosterone was 15.1 nmol/l (IQR 12.1-18.2). Nerve-sparing was full bilateral in 31% of patients (n=16), partial bilateral in 43% (n=22), and full unilateral in 26% (n=13)). All patients had satisfactory pre-operative EF (median IIEF-EF 29, IQR 24.0-30.0), of whom 98% unassisted. One patient needed PDE5i pre operatively. The median time to start rehabilitation post nsRP was 6.0 weeks (IQR=5.0 – 8.5).
Intensification and de-intensification
Five patients wanted to intensify treatment with ICI; one started within 12 mo. At 6 mo, five patients discontinued VED, two switched to on-demand VED, and one to on-demand sildenafil. After 12 mo, more patients switched to on-demand use or stopped using erectile aids (Table 2).
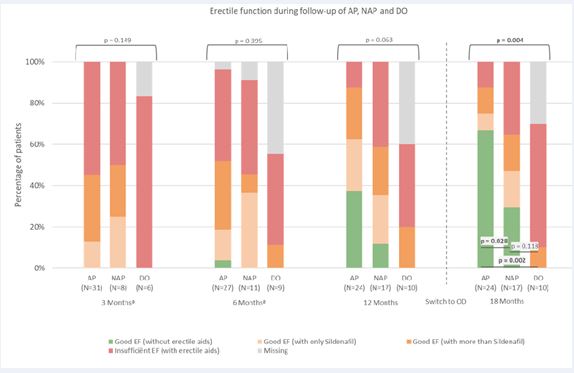
Figure 2 Erectile function during follow-up of Adherent Patients (AP), Non Adherent Patients (NAP) and Dropouts (DO).
AP = adherent patients; NAP = Non adherent patients, DO = dropouts; EF = Erectile function; OD = on demand. Unlike table 3, once a patient is marked as non-adherent or dropout, they stay in the same group at the next time point. At 12 mo, 32 of 41 patients tried intercourse without erectile aids. After 12 mo patients switched to on demand usage of erectile aids. Fischer-exact tests were used to identify differences between the groups at every time-point. At 18 mo, Fisher-exact test was also used to identify differences in erectile function without erectile aids. a The adherence of 6 patients at 3 mo and 4 patients at 6 mo was unknown and therefore could not be assigned to one of three groups.
Adherence, side effects and dropout rate Of 51 patients, 41 (80%) completed the program and 18-mo follow-up; 10 (20%) dropped out (Figure 1), mainly due to side effects of sildenafil (headaches, heartburn). No dropouts were caused by VED (Figure 1 and Table 3). 24 (59%) of the 41 patients with follow-up adhered fully to the protocol at each follow-up point (3, 6, and 12 mo); 17 (41%) were non-adherent (Figure 2). At individual visits, adherence was at least 79% for sildenafil and 76% for VED (Table 2).
Table 2: Reported side effects of sildenafil and penile vacuum devices in all patients (N=51) and dropouts (N=10).
|
Reported Side effects |
N=51 (%) |
DO N=10 (%) |
|
Sildenafil |
|
|
|
Headache, no. (%) |
15 (29,4) |
7 (70.0) |
|
Heartburn, no. (%) |
10 (19.6) |
2 (20.0) |
|
Facial flushing, no. (%) |
5 (9.8) |
1 (10.0) |
|
Dizziness, no. (%) |
3 (5.9) |
2 (20.0) |
|
Myalgia, no. (%) |
3 (5.9) |
1 (10.0) |
|
Nasal congestion, no. (%) |
3 (5.9) |
1 (10.0) |
|
Nausea, no. (%) |
2 (3.9) |
2 (20.0) |
|
Tinnitus, no. (%) |
1 (2.0) |
0 (0.0) |
|
Tachycardia, no. (%) |
1 (2.0) |
0 (0.0) |
|
Insomnia, no. (%) |
1 (2.0) |
0 (0.0) |
|
Penile vacuum device |
|
|
|
Pain, no. (%) |
4 (7.8) |
0 (0.0) |
Reported side effects experienced by patients throughout follow-up. Some patients reported multiple side effects.
Adherence of patients at each follow-up moment. a Low adherence to sildenafil was defined as either a lower frequency or a lower dosage than specified in the protocol. Sildenafil adherence declined early due to side effects. Adherence to VED decreased later on, mainly due to reduced motivation caused by the lack of recovery in unassisted EF, and not as a result of side effects such as pain (Table 2, 3 and 6, Appendix A). By nerve-sparing status, full adherence was seen in 53% of bilaterally spared patients (8/15), 80% of partially bilaterally spared patients (12/15), and 31% of unilaterally spared patients (4/13). No significant baseline characteristic differences were found among adherent, non-adherent patients, and dropouts (Table 1).
Table 3: Adherence during follow-up
|
Reported Side effects |
N=51 (%) |
DO N=10 (%) |
|
Sildenafil |
|
|
|
Headache, no. (%) |
15 (29,4) |
7 (70.0) |
|
Heartburn, no. (%) |
10 (19.6) |
2 (20.0) |
|
Facial flushing, no. (%) |
5 (9.8) |
1 (10.0) |
|
Dizziness, no. (%) |
3 (5.9) |
2 (20.0) |
|
Myalgia, no. (%) |
3 (5.9) |
1 (10.0) |
|
Nasal congestion, no. (%) |
3 (5.9) |
1 (10.0) |
|
Nausea, no. (%) |
2 (3.9) |
2 (20.0) |
|
Tinnitus, no. (%) |
1 (2.0) |
0 (0.0) |
|
Tachycardia, no. (%) |
1 (2.0) |
0 (0.0) |
|
Insomnia, no. (%) |
1 (2.0) |
0 (0.0) |
|
Penile vacuum device |
|
|
|
Pain, no. (%) |
4 (7.8) |
0 (0.0) |
Adherence of patients at each follow-up moment. a Low adherence to sildenafil was defined as either a lower frequency or a lower dosage than specified in the protocol
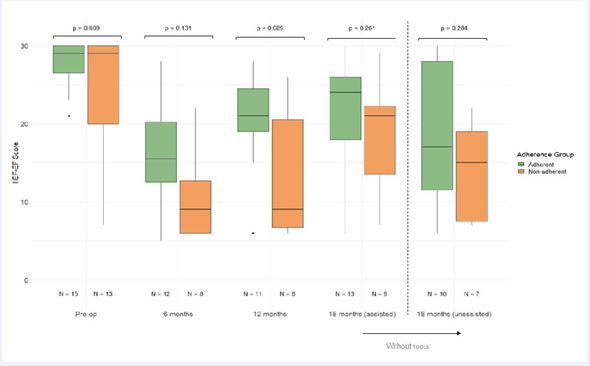
Figure 3 Boxplot of IIEF-EF.
IIEF-EF= international index of erectile function- erectile function domain. This figure displays the IIEF-EF of patients participating in penetrative sex, pre-operative and at 6, 12 and 18 mo of follow-up. Patients are divided in adherent and non-adherent patients based on their adherence at 12 mo. Regarding drop-outs, we could not obtain any patients with filled in IIEF-EF and/or IIEF-EF of patients participating in penetrative sex. Wilcoxon-rank sum test was performed to identify differences between adherent and non-adherent patients at each follow-up point.
Erectile function
At 18 mo, 33 of 51 patients (65%) achieved satisfactory erectile function (EF), with 21 (41%) reporting satisfactory unassisted erections (Figure 2; Table 4, Appendix A). When excluding dropouts, 33 of 41 (80%) achieved good EF, of whom 21 of 41 (51%) did so without erectile aids. Among patients fully adhering to the protocol, the proportion with satisfactory unassisted EF was significantly higher compared to non-adherent patients (67% vs. 29%; p = 0.028). Subgroup analysis by nerve sparing type showed that this difference remained significant only in the partially bilateral group (p = 0.008;
Table 4: Adherence and Unassisted Erectile Function at 18 Mo by Nerve-Sparing Technique
|
Nerve- sparing |
Adherence group |
Satisfactory EF |
Unsatisfactory EF |
Missing |
Total no. (%) |
p Value |
|
Unilateral, no. (%) |
Adherent |
2 (15) |
2 (15) |
0 (0) |
13 (100) |
0.511 |
|
Non- adherent |
1 (8) |
6 (46) |
0 (0) |
|||
|
Drop-out |
0 (0) |
2 (15) |
0 (0) |
|||
|
Partial bilateral, no. (%) |
Adherent |
9 (45) |
3 (15) |
0 (0) |
20 (100) |
0.008 |
|
Non- adherent |
1 (5) |
2 (10) |
0 (0) |
|||
|
Drop-out |
0 (0) |
5 (25) |
0 (0) |
|||
|
Fully bilateral, no. (%) |
Adherent |
5 (28) |
3 (17) |
0 (0) |
18 (100) |
0.619 |
|
Non- adherent |
3 (17) |
4 (22) |
0 (0) |
|||
|
Drop-out |
0 (0) |
0 (0) |
3 (17) |
|||
|
Total, no. (%) |
|
21 (42) |
27 (53) |
3 (6) |
51 (100) |
|
EF = Erectile Function. No = Number. This contingency table shows the distribution of patients by type of nerve sparing and adherence, along with their erectile function outcomes at 18 mo. The difference in satisfactory erectile function among adherent patients, non-adherent patients, and drop-outs in each nerve-sparing group was assessed using the Fisher's exact test.
Table 5: Degree of satisfaction with program of patients that reached 18 mo (N=41)
|
|
Overall N=41 |
Satisfactory EF at 18 mo N=21 |
Unsatisfactory EF at 18 mo N=20 |
p Value |
|
Degree of satisfaction, median (IQR) |
5.0 (3.0-5.0) |
5.0 (5.0-5.0) |
3.0 (2.0-5.0) |
0.001 |
Satisfaction with the program was measured using a 5-point Likert scale. 1= Very dissatisfied, 2= dissatisfied, 3= not dissatisfied/not satisfied, 4= satisfied and 5= very satisfied. The difference in satisfaction between patients with satisfactory and unsatisfactory erectile function without aids was assessed using the Wilcoxon rank- sum test.
Table 6. Categories and Reasons for Non-Adherence Among Patients During Follow- Up (N=17)
|
Category |
no. (%) |
|
Lack of motivation Caused by lack of effectiveness on the recovery of unassisted erections Due to a busy work schedule Not further clarified |
5 (29.4) 1 (5.9) 6 (35.3) |
|
Side effects Daily 75mg sildenafil caused too many side effects |
4 (23.5) |
|
Lack of guidance Missed follow-up and lack of information. |
1 (5.9) |
|
Incontinence Incontinence made using the vacuum device 5 times a week unpleasant |
1 (5.9) |
Reasons provided by patients for low adherence. Some patients reported more than one reason.
Table 4, Appendix A). None of the patients who dropped out achieved satisfactory unassisted erections at 18 mo (Figure 2). Furthermore, median IIEF-EF scores, primarily reflecting assisted erections, increased during follow up for both adherent and non-adherent patients. No Significant difference in IIEF-EF scores was found between the three different groups at any time point (Figure 3, Appendix A).
Patients with satisfactory unassisted erections at 18 mo of follow-up were significantly more satisfied with the program than those who were not (p = 0.001; Table 5, appendix A).
DISCUSSION
Erectile dysfunction is a major side effect of robot assisted radical prostatectomy for localized prostate cancer. Despite nerve-sparing surgery, EF recovery remains low [10-12], significantly affecting quality of life [3-5]. Therefore, PDE5i and VED are commonly proposed as treatment options, but robust evidence for their long-term effectiveness on EF recovery in structured rehabilitation programs is still lacking [16-18]. To address this gap, a feasibility study was conducted as a first step toward a large-scale randomized controlled trial (RCT). The aim was to assess whether an intensive, multimodal rehabilitation program could be implemented within a clinical research setting, including accrual, adherence, dropout rates and preliminary effects on erectile function. Of 66 eligible nsRP patients, 51 were enrolled in a standardized protocol involving early initiation (≤4 mo) of VED therapy and daily sildenafil (75/100mg), plus 18 mo follow-up and coaching. Despite the intensity of the program, a relatively high inclusion rate and adherence rate were observed. Notably, patients with unilateral or partial nerve-sparing also demonstrated meaningful recovery when they adhered to the protocol. This challenges the assumption that only bilateral nerve-sparing patients benefit from rehabilitation and suggests that even partial preservation may respond positively to structured intervention. The high proportion of patients regaining unassisted EF (51% of all patients and 67% of adherent patients) was also unexpectedly high compared to previous literature. Several factors explain these high rates. Both inclusion and adherence may be explained by referral of motivated patients and removal of financial barriers. However, while inclusion within the eligible group was high, the proportion of participants relative to the total RARP population was low, especially in a high-volume centre (>400 RARP/year). This highlights that even in specialized settings, the proportion of patients both eligible and willing to participate in intensive rehabilitation remains limited, as also noted by Miranda et al. [22]. Additionally, some patients receive postoperative follow-up elsewhere, limiting exposure to trials offered at the operating centre. Consequently, improved referral pathways and/ or multicentre collaboration may be essential to enhance accrual in future studies, alongside offering randomization arms that are acceptable to patients. Beyond inclusion rates, adherence and dropout rates are arguably even more critical for determining success. Systematic reviews confirm that adherence is rarely reported [16], making this study unique in thoroughly reporting adherence data. In the only other prospective trial with >12 mo follow-up combining PDE5i and VED, Albaugh et al. [21], adherence was poor. VED use dropped to 2–5% at 24 mo, and PDE5i adherence declined slightly over time—despite structured follow-up. One key reason for VED decline, in their study and observed in our cohort, is lack of perceived effectiveness on regaining their unassisted erectile function. In contrast, PDE5i discontinuation is often driven by side effects [21], which also contributed to dropouts in our study. Despite these challenges, our study demonstrated substantially higher adherence overall (59% fully adherent; ≥76% VED and ≥79% sildenafil at individual visits), underscoring the importance of feasible protocols alongside counselling on realistic expectations. Furthermore, future trials should anticipate dropouts by including a larger sample size upfront to maintain statistical power. Turning to functional outcomes, our assisted EF (80%) and unassisted EF (51%) at 18 mo were notably higher than those reported in previous trials using combined PDE5i and VED therapy (Zhang et al. [20]: 39% assisted at 12 mo; Albaugh et al. [21]: 33% assisted at 24 mo). However, direct comparison remains challenging due to differences in follow-up, EF definitions, and assessment tools. Nevertheless, these findings are encouraging and may partly be explained by early initiation of rehabilitation (supported by prior literature), particularly given the heterogeneity of our cohort, which included unilateral, partial, and bilateral nerve-spared patients. While these findings are promising, this study has seral limitations which influence interpretation; The single centre one-armed design and relatively small sample size constrain the applicability of the results regarding EF. Furthermore, missing data may have influenced adherence estimates. Lastly, the IIEF-EF questionnaire was not applicable for all patients due to lack of sexual intercourse, resulting in a reduced amount of data. Future research should therefore consider alternative patient reported outcome measures (PROM) that include patients without sexual activity or a partner, such as the EHS used in the present study. This is important, as lower erectile function is associated with impaired self-esteem [24], which remains relevant for all men regardless of partner status. A strength of the study is the detailed documentation of inclusion, non-inclusion, and dropout reasons. This allows for the identification of subgroups—such as patients with unilateral nerve-sparing or those who discontinue due to side effects or lack of perceived benefit—that may be at higher risk of non-adherence or poor outcomes. These insights are crucial for guiding and stratifying patients in future trials and eventually giving tailored advice regarding rehabilitation options. Future studies, including our upcoming PEHAB-II trial, should adopt a Multicentre design to enhance recruitment and generalizability. A randomized design with stratification by nerve-sparing status is recommended to ensure balanced groups and enable meaningful subgroup analyses, particularly for patients with lower adherence. To reach eligible participants—especially those followed up in other hospitals—structured outreach and referral pathways are essential. Close monitoring and realistic counselling may help reduce dropout rates, improve adherence and data completeness. In addition, planning for a larger sample size upfront will help maintain statistical power despite anticipated dropouts. Lastly, incorporating alternative PROMs will allow inclusion of patients who are not participating in penetrative sex (i.e. due to lack of partner or other reasons). Taken together, these measures will be critical to optimize trial design and strengthen the evidence base for penile rehabilitation.
CONCLUSION
This feasibility study demonstrates that an intensive, early multimodal penile rehabilitation program—using daily sildenafil (75–100 mg) and VED training five times per week—after nerve-sparing RARP is implementable and associated with a trend toward improved EF recovery compared to previous literature. These findings support the need for a Multicentre randomized trial to confirm efficacy and generalizability.
ACKNOWLEDGMENTS
We thank all urologists and nurse practitioners from the urology department for referring patients to the sexual health clinic. Special thanks to Dr. Tillier (nurse practitioner) for obtaining the IIEF questionnaires.
CONFLICTS OF INTEREST
Memidis Pharma provided vacuum erection devices free of charge for use in this study. The authors have no other conflicts of interest to declare.
REFERENCES
- Sighinolfi MC, Montorsi F, Eissa A, Patel V. Outcomes of RALP: An Evidence-Based Approach. In: Wiklund P, Mottrie A, Gundeti MS, Patel V, editors. Robotic Urologic Surgery. Cham: Springer International Publishing. 2022; 199-216.
- Mulhall JP. Defining and reporting erectile function outcomes afterradical prostatectomy: challenges and misconceptions. J Urol. 2009; 181: 462-471.
- Hoffman RM, Hunt WC, Gilliland FD, Stephenson RA, Potosky AL. Patient satisfaction with treatment decisions for clinically localized prostate carcinoma. Results from the Prostate Cancer Outcomes Study. Cancer. 2003; 97: 1653-1662.
- Chambers SK, Chung E, Wittert G, Hyde MK. Erectile dysfunction, masculinity, and psychosocial outcomes: a review of the experiences of men after prostate cancer treatment. Transl Androl Urol. 2017; 6: 60-68.
- Bowie J, Brunckhorst O, Stewart R, Dasgupta P, Ahmed K. Body image, self-esteem, and sense of masculinity in patients with prostate cancer: a qualitative meta-synthesis. J Cancer Surviv. 2022; 16: 95-110.
- Eichelberg C, Erbersdobler A, Haese A, Schlomm T, Chun FKH, Currlin E, et al. Frozen Section for the Management of Intraoperatively Detected Palpable Tumor Lesions During Nerve-Sparing Scheduled Radical Prostatectomy. European Urology. 2006; 49:1011-1018.
- Fosså SD, Beyer B, Dahl AA, Aas K, Eri LM, Kvan E, et al. Improved patient-reported functional outcomes after nerve-sparing radical prostatectomy by using NeuroSAFE technique. Scandinavian J Urology. 2019; 53: 385-391.
- Ambrosini F, Preisser F, Tilki D, Heinzer H, Salomon G, Michl U, et al. Nerve-sparing radical prostatectomy using the neurovascular structure-adjacent frozen-section examination (NeuroSAFE): results after 20 years of experience. Prostate Cancer Prostatic Dis. 2025; 28: 483-489.
- Dinneen E, Almeida-Magana R, Al-Hammouri T, Pan S, Leurent B, Haider A, et al. Effect of NeuroSAFE-guided RARP versus standard RARP on erectile function and urinary continence in patients with localised prostate cancer (NeuroSAFE PROOF): a multicentre, patient-blinded, randomised, controlled phase 3 trial. Lancet Oncol. 2025; 26: 447-458.
- Capogrosso P, Vertosick EA, Benfante NE, Eastham JA, Scardino PJ, Vickers AJ, et al. Are We Improving Erectile Function Recovery After Radical Prostatectomy? Analysis of Patients Treated over the Last Decade. Eur Urol. 2019; 75: 221-228.
- Mirmilstein G, Rai BP, Gbolahan O, Srirangam V, Narula A, Agarwal S, et al. The neurovascular structure-adjacent frozen-section examination (NeuroSAFE) approach to nerve sparing in robot- assisted laparoscopic radical prostatectomy in a British setting - a prospective observational comparative study. BJU Int. 2018; 121: 854-862.
- Nelson CJ, Scardino PT, Eastham JA, Mulhall JP. Back to baseline: erectile function recovery after radical prostatectomy from the patients’ perspective. J Sex Med. 2013; 10: 1636-1643.
- Kyriazis I, Spinos T, Tsaturyan A, Kallidonis P, Stolzenburg JU, Liatsikos E. Different Nerve-Sparing Techniques during Radical Prostatectomy and Their Impact on Functional Outcomes. Cancers (Basel). 2022; 14: 1601.
- Rabbani F, Schiff J, Piecuch M, Yunis LH, Eastham JA, Scardino PT, et al. Time course of recovery of erectile function after radical retropubic prostatectomy: does anyone recover after 2 years? J Sex Med. 2010; 7: 3984-3990.
- Iacono F, Giannella R, Somma P, Manno G, Fusco F, MironeV. Histological alterations in cavernous tissue after radical prostatectomy. J Urol. 2005; 173: 1673-1676.
- Sari Motlagh R, Abufaraj M, Yang L, Mori K, Pradere B, Laukhtina E, et al. Penile Rehabilitation Strategy after Nerve Sparing Radical
Prostatectomy: A Systematic Review and Network Meta-Analysis of Randomized Trials. J Urol. 2021; 205: 1018-1030.
- Pirola GM, Naselli A, Maggi M, Gubbiotti M, Rubilotta E, Jeremy Yuen-Chun T, et al. Vacuum erection device for erectile function rehabilitation after radical prostatectomy: which is the correct schedule? Results from a systematic, scoping review. Int J Impot Res. 2024; 36: 194-200.
- Nicolai M, Urkmez A, Sarikaya S, Fode M, Falcone M, Albersen M, et al. Penile Rehabilitation and Treatment Options for Erectile Dysfunction Following Radical Prostatectomy and Radiotherapy: A Systematic Review. Front Surg. 2021; 8: 636974.
- Basal S, Wambi C, Acikel C, Gupta M, Badani K. Optimal strategy for penile rehabilitation after robot-assisted radical prostatectomy based on preoperative erectile function. BJU Int. 2013; 111: 658-665.
- Zhang M, Che JZ, Liu YD, Wang HX, Huang YP, Lv XG, et al. A prospective randomized controlled study on scheduled PDE5i and vacuum erectile devices in the treatment of erectile dysfunction after nerve sparing prostatectomy. Asian J Androl. 2022; 24: 473-477.
- Albaugh J, Adamic B, Chang C, Kirwen N, Aizen J. Adherence and barriers to penile rehabilitation over 2 years following radical prostatectomy. BMC Urol. 2019; 19: 89.
- Miranda EP, Benfante N, Kunzel B, Nelson CJ, Mulhall JP. A Randomized, Controlled, 3-Arm Trial of Pharmacological Penile Rehabilitation in the Preservation of Erectile Function After Radical Prostatectomy. J Sex Med. 2021; 18: 423-429.
- Engel JD. Effect on sexual function of a vacuum erection device post- prostatectomy. Can J Urol. 2011; 18: 5721-5725.
- Hilger C, Schostak M, Neubauer S, Magheli A, Fydrich T, Burkert S, et al. The importance of sexuality, changes in erectile functioning and its association with self-esteem in men with localized prostate cancer: data from an observational study. BMC Urol. 2019; 19: 9.
- EAU Guidelines. Edn. presented at the EAU Annual Congress Madrid 2025 ed. Arnhem, The Netherlands: European Association of Urology; 2025.
Abstract
Background & Objective: Radical prostatectomy (RP) is associated with erectile dysfunction and despite nerve-sparing (ns) surgery fewer than 50% of patients regain satisfactory erectile function (EF) within two years. Optimal multimodal rehabilitation strategies remain unclear. This prospective feasibility study evaluated whether an intensive program combining daily sildenafil and vacuum erection device (VED) therapy could be implemented and tolerated.
Methods: Between May 2021 and October 2022, patients with satisfactory preoperative EF and unsatisfactory EF after nsRP, without contraindications for sildenafil, In this single-centre study. The protocol included early initiation (≤4 mo) of daily sildenafil (75/100mg) and regular VED use (5 times a week), with 18 mo follow-up. EF was assessed using clinical reports and patient-reported outcomes (Erection Hardness Score and International Index of Erectile Function).
Key findings and Limitations: Of 66 eligible patients, 51 were enrolled; nerve sparing was full bilateral in 31%, partial bilateral in 43%, and unilateral in 26%. Twenty percent discontinued, mainly due to sildenafil side effects. Among 41 completing follow-up, 59% were fully adherent. At 18 mo, 80% achieved satisfactory EF, including 51% without erectile aids. Limitations include the single-centre, one-arm design, small sample size, and missing data affecting adherence estimates.
Conclusions and clinical implications: Early multimodal penile rehabilitation after nsRP is implementable, associated with high adherence and promising EF recovery. Multicentre randomized trials are needed to confirm efficacy and generalizability.
Keywords
• Penile rehabilitation
• Erectile dysfunction
• Radical prostatectomy
• Vacuum device
• Phosphodiesterase inhibitor










































































































































{kind=link}