Paratesticular Leiomyoma
- 1. Department of Urologic Oncology, FUCDIM Urological Center, Argentina
- 2. Department of Reconstructive Surgery, FUCDIM Urological Center, Argentina
- 3. Department of Reconstructive Surgery, FUCDIM Urological Center, Argentina
- 4. Department of Urologic Oncology, FUCDIM Urological Center, Argentina
- 5. Chairman of FUCDIM, Cordoba, Argentina
Abstract
Objective: to describe a conservative approach of a paratesticular leiomyoma, an unusual diagnosis among scrotal tumors.
Methods: A hypogonadic 55 year-old man, complaining of gradual and painless growth of the right scrotum. Studies were done, and surgery was indicated, with the possibility of orchiectomy.
Results: Through an inguinal approach, with transient clamping of the inguinal cord, after a thorough local examination, lesion was excised, preserving the testicle. Imaging and laboratory postoperative controls were normal.
Conclusion: When facing scrotal lesions, surgery must be planned as an oncologic procedure (inguinal approach, clamping of the cord); however, if testicle and inguinal cord are not compromised, the lesion does not appear to be malignant and can be properly dissected, a conservative surgery can be done.
Keywords
Paratesticular tumour; Conservative surgery; Leiomyoma
Citation
Dellavedova T, Olmedo J, Malizia E, Quinteros L, Minuzzi F (2022) Paratesticular Leiomyoma – A Case Report. JSM Sexual Med 6(3): 1090
INTRODUCTION
Primary paratesticular tumours are infrequent findings, with an incidence of 2%, and represent 7-10% of all intrascrotal lesions. Most of them are benign and 75% arise from the spermatic cord.
Among them, there are benign cord tumours (lypoma being the most frequent) and epydidimal lesions (adenomatoid tumours, first in incidence, followed by leiomyoma) [1].
CASE PRESENTATION
A 55-year old hypogonadic patient, with a painless slowly growing right hemi-scrotum, with four years without searching medical attention.
On physical examination, the upper pole of the right testicle was compromised with a solid intrascrotal lesion; Left testicle was hypotrophic. Serum testicular markers were negative, and both ultrasound and MRI confirmed the paratesticular lesion (Figure 1).
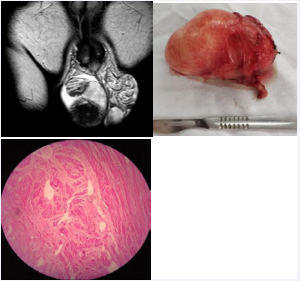
Figure 1: Paratesticular leiomyoma.
Acces was made by the groin, spermatic cord was dissected and carefully clamped, bringing outside the solid lesion and the right testicle. The described lesion could be dissected from the testicle and the cord, both looking normal and without compromise. Tumor was extracted; cord was unclamped [2]. Orchydopexy of the right testis was done. Immediate postoperative follow-up was normal and both late controls on imaging and laboratory were normal [3].
CONCLUSION
Genito-urinary leiomyoma derives from mesenchymal cells, arising more frequently from renal capsule, bladder wall, epidydimis and tunica albuginea.
When managing non-testicular scrotal lesions, a radical surgery must be planned, with inguinal approach and clamping of the cord. However, if no compromise of the testicle and cord is found, lesion looks benign and can be satisfactorily resected, a conservative approach is feasible.










































































































































{kind=link}