Peyronie
- 1. Department of Urology, Magna Graecia University of Catanzaro, Italy
- 2. Department of Urology, University of Florence, Italy
DISCUSSION
CCH/Xiaflex®; Xiapex® is a mixture of two Clostridium histolyticum collagenases [AUX-I (a Class I clostridial collagenase) and AUX-II (a Class II clostridial collagenase)]. Administered by intralesional injection, it is available in various countries for the treatment of adult men with PD. In two doubleblind, multinational, phase III studies, CCH improved the physical (penile curvature) and psychological (patient-reported bother) aspects of PD in adult men (1). Such beneficial effects were also seen in two open-label, multinational, phase III studies, with potential benefits for patients’ partners and maintained efficacy over up to 5 years additionally reported [4]. Large realworld studies generally supported the efficacy of CCH. CCH is generally well tolerated by patients, with most treatment-related adverse events being mild or moderate in severity and commonly referred as penile hematoma or ‘bruising’, pain and swelling [5]. Moreover, the use of CCH is not associated with penile length shortening. Current evidence indicates that CCH is an effective, generally well-tolerated, and, compared with surgery, minimally invasive option for the treatment of adult men with PD. Although
CCH is not clearly indicated for treatment during the acute phase of PD, recently data advice that CCH use during this phase can be effective and safe [6,7]. Few studies are currently available on the prevalence of male sexual diseases, and PD in particular, due to the difficult application of observational studies or andrological disease prevention campaigns on apparently healthy subjects [8]. Tal et al., reported thirty-two teenaged males were evaluated for PD in a single institution over a 10-year period [2]. The median age was 18 (15-19) years. Sixteen percent of patients reported antecedent penile trauma, half of which happened during coitus or masturbation, and 18% of patients had hemoglobin (Hb) A1c levels > 5%. Dupuytren’s contracture was not seen in this population. Twenty-two percent of patients presented with penile pain. Subsequent erectile disfunction (ED) was seen in 37% of patients. Multiple noncontiguous plaques
were seen in 37% of patients. Twelve percent were previously treated with vitamin E, while another 12% had previous intralesional verapamil. High distress was reported by 94% of patients. Thirty-four percent sought medical attention for
anxiety/mood disorder, and 28% had a negative encounter with a sexual partner related to PD. All of the 32 patients had penile curvature with a mean of 32 ± 12 degrees. Seventy-two percent of the patients had dorsal curvature while 22% had an associated deformity. Using duplex Doppler ultrasound, 12% had a calcified plaque, while none of the patients had abnormal hemodynamics. When compared with PD in adults, teenagers had greater than seven times the prevalence of multiple noncontiguous plaques (37% vs. 5%). When PD occurs in teenagers it often causes high distress levels [2]. Our three patients (15-17 years old) differed from the previous series in that they are two-thirds virgins and
none reported penile trauma. In one case, the presence of PD in the father and grandfather suggested the possible hereditability. Apart from the small hematomas caused by the injections, the treatment was safe and effective in all patients.
CONCLUSIONS
These three cases confirmed that the treatment with collagenase can also be carried out under 18 years. Both in the acute phase (<12 months) and in the stabilized phase (>12 months) with excellent results. This case series demonstrates that CCH can be an alternative to surgery that would result in penile shortening occuring at a stage of fundamental psychosexual development. These three patients re-propose the problem related to the possible use of the drug in Europe related to costs and a health care system not based on the insurance model [9].
REFERENCES
1. Hoy SM. Collagenase Clostridium Histolyticum: A Review in Peyronie’s Disease. Clin Drug Investig. 2020; 40: 83–92.
2. Tal R, Hall MS, Alex B, Choi J, Mulhall JP. Peyronie’s disease in teenagers. J Sex Med. 2012; 9: 302–8.
3. Abdel Raheem A, Capece M, Kalejaiye O, Abdel-Raheem T, Falcone M, Johnson M, et al. Safety and effectiveness of collagenase clostridium histolyticum in the treatment of Peyronie’s disease using a new modified shortened protocol. BJU Int. 2017; 120: 717–723.
4. Gelbard M, Goldstein I, Hellstrom WJG, McMahon CG, Smith T, Tursi J, et al. Clinical efficacy, safety and tolerability of collagenase clostridium histolyticum for the treatment of peyronie disease in 2 large doubleblind, randomized, placebo controlled phase 3 studies. J Urol. 2013; 190: 199–207.
5. Natale C, McLellan DM, Yousif A, Hellstrom WJG. Review of Intralesional Collagenase Clostridium Histolyticum Injection Therapy and Related Combination Therapies in the Treatment of Peyronie’s Disease (an Update). Sex Med Rev. 2021; 9: 340–349.
6. Cocci A, Di Maida F, Russo GI, Capogrosso P, Francesco L, Rizzo M, et al. Efficacy of Collagenase Clostridium histolyticum (Xiapex®) in Patients with the Acute Phase of Peyronie’s Disease. Clin Drug Investig. 2020; 40: 583–588.
7. Nguyen HMT, Anaissie J, DeLay KJ, Yafi FA, Sikka SC, Hellstrom WJG. Safety and Efficacy of Collagenase Clostridium histolyticum in the Treatment of Acute-Phase Peyronie’s Disease. J Sex Med. 2017; 14: 1220–1225.
8. Mondaini N, Silvani M, Zenico T, Gallo F, Rosso F, Cai T et al. Genital diseases awareness in young male students: Is information necessary to protect them? Arch Ital di Urol Androl organo Uff [di] Soc Ital di Ecogr Urol e Nefrol. 2013; 85: 14–9.
9. Cocci A, Russo GI, Salamanca JIM, Ralph D, Palmieri A, Mondaini N. The End of an Era: Withdrawal of Xiapex (Clostridium histolyticum Collagenase) from the European Market. Eur Urol. 2020; 77: 660–661.
INTRODUCTION
Peyronie’s disease (PD) is commonly seen in middle-aged men, and is rare in teenagers [1]. Collagenase Clostridium Histolyticum (CCH) is actually the non-surgical gold standard treatment for PD as its safety and efficacy has been demonstrated in large well-designed clinical trials. CCH is indicated for the treatment of adult men (>18 years old) with Peyronie’s disease having a palpable plaque and curvature deformity ≥ 30° at baseline [2]. Hereby we present three cases of PD in teenagers (15-17 years old) effectively treated with CCH.
CASE 1
A 15-year-old boy came to our attention with PD that had arisen 4 months ago. Both his father (52 years old) and grandfather (77 years old) suffered from PD. Doppler ultrasonography of the penis showed a lesion. Given the age, a congenital form was ruled out. Genital trauma and absence of Dupuytren’s contracture were also excluded. The boy was a virgin. The patient and parents were informed of the existence of palliative treatments with poor results. The possibility of collagenase treatment was exposed, which, given his age and onset period (4 months), was off-label. After both parents signed consent, the treatment was performed, and the curvature was reduced by 17 degrees after 3 treatments following the modified protocol described by Raheem [3]. Ecchymosis developed and resolved in about 48 hours in all three treatments. At 36 months follow-up, the disease had not progressed (Figure 1).
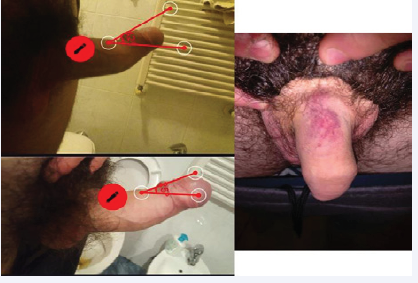
Figure 1: Penis before and after treatment with CCH; Ecchymosis developed and resolved in about 48 hours.
CASE 2
A 17-year-old boy came to our attention with a history of Peyronie’s disease that had been onset for 1 year. During this time, the patient took vitamin D 300 mg daily for 6 months. He then underwent six ESWL treatments with no results and a current curvature of 45 degrees. History was negative for genital trauma and Dupuytren’s disease. Doppler ultrasonography of the penis showed a lesion. Again, the collagenase treatment was out of indication due to the patient’s age. After consent was signed by both parents, the treatment was performed achieving a curvature reduction of 15 degrees. A hematoma developed and resolved in 72 hours only for the first injection. At 24 months follow-up, PD was stabilized.
CASE 3
A 15-year-old boy with disease onset dating back 18 months earlier, presented with a left lateral curvature of about 40 degrees. The patient reported a preceding curvature of 20 degrees as per congenital penile curvature. Doppler ultrasound of the penis showed a lesion. History was negative for sexual activity or traumatic events, but positive for intense masturbation in the past 2 years. After consent was signed by both parents, treatment was performed with a curvature reduction of 15 degrees and no side effects. At 24 months follow-up, the patient had no worsening of the disease.










































































































































{kind=link}