Degenerative Spine Disease and Cancer: Is there a Link?
- 1. Department of Radiology, Drexel University College of Medicine, USA
Abstract
Objective: Within our radiology department, we anecdotally observed that patients over the age of 65 with cancer demonstrated significantly less degenerative disease of the spine (DDD) compared to patients without cancer when reviewing CT scans of the abdomen and pelvis. The objective of this study is to determine if a statistical correlation exists between cancer and DDD.
Materials and Methods: A list of subjects with CT scans of the abdomen and pelvis between January 1, 2014 and February 28, 2016 was compiled for retrospective review. Test subjects with known cancer were selected from our institution’s Tumor Board Registry and control subjects without a diagnosis of cancer were selected chronologically from our PACS system. After vetting for inclusion and exclusion criteria, the CT scans were anonymized and reviewed by three radiologists who subjectively evaluated degenerative changes of the anterior column, facet joints, and sacroiliac joints using a 4-point severity scale. Subjects were subdivided into 40-49, 50-59, 60-69, and 70-79years old age groups for comparison purposes.
Results: Out of 164 test subjects (with cancer) and 421control subjects (without cancer), 75 test subjects and 90 control subjects satisfied the inclusion and exclusion criteria. With increasing age, the overall incidence and severity of DDD was less in the test group compared to the control group. The 70-79years-old test group demonstrated a 37% lower overall degenerative disease severity score in the anterior column compared to the control group. Overall intraobserver reliability was 84%.
Conclusions: The results support our observation that there is a significant difference in DDD in cancer patients compared to non-cancer patients. With further research and investigation, an underlying factor associated with the generation or suppression of degenerative changes may be discovered and exploited to prevent or treat cancer.
Keywords
Degenerative disease of the spine , DDD in cancer.
CITATION
Stark I, Shames J, Misiura A, Thomas B, Hirsch D, et al. (2017) Degenerative Spine Disease and Cancer: Is there a Link? JSM Spine 2(1): 1012.
INTRODUCTION
The driving force behind our need to develop more effective treatment and preventative strategies for cancer is clear with one in five people ultimately succumbing to cancer and 14.5 million annual new diagnoses of cancer in the United States alone [1]. Some of the more elegant and significant breakthroughs in medicine have been accomplished by unveiling unique relationships between two presumably distinct disease processes. We believe we found one such unique relationship between degenerative disease of the spine (DDD) and cancer.
Test subjects were derived chronologically from the January 1, 2014 through February 28, 2016 Drexel College of Medicine/ Hahnemann University Hospital Tumor Board Registry to ensure the subject had a biopsy confirmed diagnosis of cancer. Additional inclusion criteria included having a CT of the abdomen and pelvis performed at Hahnemann University Hospital or its outpatient imaging center between January 1, 2014 and February 28, 2016. Exclusion criteria for the test group included a history of spinal surgery, traumatic back injury, a syndrome associated with cancer, or visible metastatic disease in or around the spine. Patients that only had a CT of the abdomen or CT of the pelvis were excluded. The target number of subjects per age group was set at 25 (Figure 1).
Control subjects were derived from a chronologic list of patients with a CT of the abdomen and pelvis performed at Hahnemann University Hospital or its outpatient imaging center between January 1, 2014 and February 28, 2016. This list was generated by our institutions PACS (McKesson, San Francisco, CA, USA). The date range was limited to obtain a maximum of 25 subjects per age group. This subject list was then crossreferenced with our electronic medical record system (Cerner, North Kansas City, MO, USA) to ensure that an adequate history and physical was documented. Exclusion criteria included a diagnosis of cancer, history of spinal surgery, traumatic back injury, or a syndrome associated with cancer. Subjects with non-traumatic vertebral fractures, diffuse idiopathic skeletal hyperostosis, spondylolisthesis and scoliosis were also excluded. Patients that only had a CT of the abdomen or CT of the pelvis were additionally excluded (Figure 2).
CT scans of the abdomen and pelvis were acquired on multidetector CT machines (including a GE Light speed 16 and GE Discovery CT750 HD, Milwaukee, WI, USA and Toshiba Aquillon 64, Tustin, CA, USA) with a slice thickness of 2.5 mm. The CT scans of the abdomen and pelvis of the test and control groups were assigned a randomized number from 1-165. Next, the extra-axial soft tissues were removed and axial and sagittal reconstructions in a bone algorithm were generating using GE AW Server software (Little Chalfont, United Kingdom). These post-processed images were transferred to K-PACS (London, United Kingdom), Digital Imaging and Communications in Medicine (DICOM) imaging software, to anonymize the reconstructions and re-identity the patients with their randomized number.
Three radiologists, with greater than ten years of experience, participated in this study. These included a board certified neuroradiologist, a board certified musculoskeletal radiologist, and a board certified body imager.The radiologists individually reviewed the anonymized studies on K-PACS and assessed for degenerative changes at three locations; the anterior column (AC), facet joints, and sacroiliac joints (SI) (Table 1). The severity of degenerative change of the AC and SI were defined using a 4-point scale; 0 indicating no degenerative changes, 1 indicating minimal degenerative changes, 2 indicating moderate degenerative changes, and 3 indicating severe degenerative changes. AC degenerative changes were further characterized as focal or diffuse using a 2-point scale; 1 indicating degenerative disease seen only at one vertebral level and 2 indicating degenerative disease seen at more than one level. Facet arthropathy (FA) was also defined using a 4-point scale; 0 indicating no arthropathy, 1 indicating minimal arthropathy, 2 indicating moderate arthropathy, and 3 indicating significant arthropathy. FA was further defined as focal or diffuses using a 2-point scale; 1 indicating disease only occurring at one level and 2 indicating disease seen at more than one level.
MATERIALS AND METHODS
Institutional Review Board (IRB) approval was obtained for this retrospective data analysis prior to the commencement of the study. Two study groups were compiled: a test group consisting of patients with known cancer and a control group consisting of patients without a diagnosis of cancer. The two groups were subdivided by age: 40–49, 50–59, 60–69, and 70–79 years-old.
Test subjects were derived chronologically from the January 1, 2014 through February 28, 2016 Drexel College of Medicine/ Hahnemann University Hospital Tumor Board Registry to ensure the subject had a biopsy confirmed diagnosis of cancer. Additional inclusion criteria included having a CT of the abdomen and pelvis performed at Hahnemann University Hospital or its outpatient imaging center between January 1, 2014 and February 28, 2016. Exclusion criteria for the test group included a history of spinal surgery, traumatic back injury, a syndrome associated with cancer, or visible metastatic disease in or around the spine. Patients that only had a CT of the abdomen or CT of the pelvis were excluded. The target number of subjects per age group was set at 25 (Figure 1).
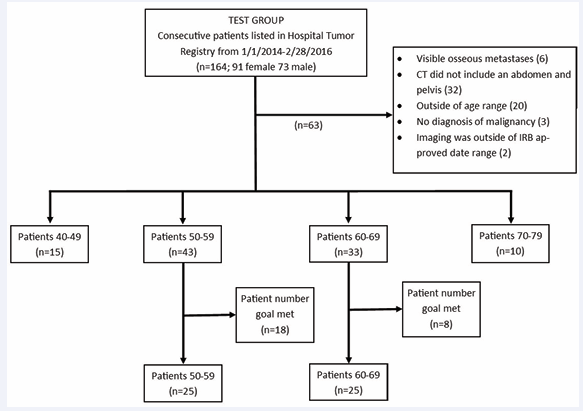
Figure 1: Test group selection flow chart. Flow chart delineating the inclusion and exclusion criteria that formulated the test group (cancer group). Targeted goal was 25 subjects per age group.
Control subjects were derived from a chronologic list of patients with a CT of the abdomen and pelvis performed at Hahnemann University Hospital or its outpatient imaging center between January 1, 2014 and February 28, 2016. This list was generated by our institutions PACS (McKesson, San Francisco, CA, USA). The date range was limited to obtain a maximum of 25 subjects per age group. This subject list was then cross referenced with our electronic medical record system (Cerner, North Kansas City, MO, USA) to ensure that an adequate history and physical was documented. Exclusion criteria included a diagnosis of cancer, history of spinal surgery, traumatic back injury, or a syndrome associated with cancer. Subjects with non-traumatic vertebral fractures, diffuse idiopathic skeletal hyperostosis, spondylolisthesis and scoliosis were also excluded. Patients that only had a CT of the abdomen or CT of the pelvis were additionally excluded (Figure 2).
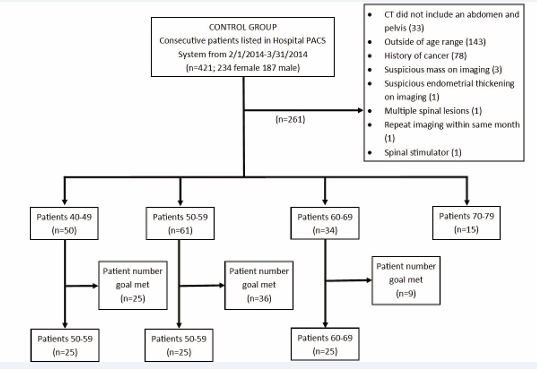
Figure 2: Control group selection flow chart. Flow chart delineating the inclusion and exclusion criteria that formulated the control group (non-cancer group). Targeted goal was 25 subjects per age group.
CT scans of the abdomen and pelvis were acquired on multidetector CT machines (including a GE Light speed 16 and GE Discovery CT750 HD, Milwaukee, WI, USA and Toshiba Aquillon 64, Tustin, CA, USA) with a slice thickness of 2.5 mm. The CT scans of the abdomen and pelvis of the test and control groups were assigned a randomized number from 1-165. Next, the extra-axial soft tissues were removed and axial and sagittal reconstructions in a bone algorithm were generating using GE AW Server software (Little Chalfont, United Kingdom). These post-processed images were transferred to K-PACS (London, United Kingdom), Digital Imaging and Communications in Medicine (DICOM) imaging software, to anonymize the reconstructions and re-identity the patients with their randomized number.
Three radiologists, with greater than ten years of experience, participated in this study. These included a board certified neuroradiologist, a board certified musculoskeletal radiologist, and a board certified body imager.The radiologists individually reviewed the anonymized studies on K-PACS and assessed for degenerative changes at three locations; the anterior column (AC), facet joints, and sacroiliac joints (SI) (Table 1).
| Table 1: Degenerative Disease Score. Three board certified radiologists, specializing in musculoskeletal radiology, neuroradiology and body imaging, provided a subjective analysis of the severity of degenerative disease within the anterior column of the lumbar spine (AC), lumbar facet joints (FA) and sacroiliac joints (SI) of subjects with a known diagnosis of cancer (test group) and those without cancer (control group). Listed is the average severity score per age and control or test group. AC= degenerative disease of the anterior column; 0- none, 1.0- minimal, 2.0- moderate, 3.0- severe. FA= lumbar facet joints; 0- none, 1.0- minimal, 2.0- moderate, 3.0- severe.SI= sacroiliac joints; 0- none, 1.0- minimal, 2.0- moderate, 3.0- severe. F/ D= focal/ diffuse; 1.0- degenerative disease at one vertebral level and 2.0- disease at more than one level. Overall= average of degenerative changes of spine, facet and sacroiliac joint. | ||||||
| Degenerative Disease Score | AC C | AC T | FA C | FA T | SI C | SI T |
| 40-49 | 0.71 | 1.09 | 0.95 | 0.56 | 0.80 | 0.76 |
| 50-59 | 1.21 | 1.17 | 0.85 | 1.17 | 0.65 | 0.76 |
| 60-69 | 1.49 | 1.28 | 1.31 | 1.20 | 0.93 | 0.83 |
| 70-79 | 2.16 | 1.37 | 1.91 | 1.70 | 0.96 | 0.77 |
| Total p-value | AC | FA | SI | |||
| 40-49 | 0.10 | 0.04 | 0.41 | |||
| 50-59 | 0.43 | 0.09 | 0.26 | |||
| 60-69 | 0.19 | 0.32 | 0.31 | |||
| 70-79 | 0.02 | 0.28 | 0.20 | |||
The severity of degenerative change of the AC and SI were defined using a 4-point scale; 0 indicating no degenerative changes, 1 indicating minimal degenerative changes, 2 indicating moderate degenerative changes, and 3 indicating severe degenerative changes. AC degenerative changes were further characterized as focal or diffuse using a 2-point scale; 1 indicating degenerative disease seen only at one vertebral level and 2 indicating degenerative disease seen at more than one level. Facet arthropathy (FA) was also defined using a 4-point scale; 0 indicating no arthropathy, 1 indicating minimal arthropathy, 2 indicating moderate arthropathy, and 3 indicating significant arthropathy. FA was further defined as focal or diffuses using a 2-point scale; 1 indicating disease only occurring at one level and 2 indicating disease seen at more than one level.
RESULTS
A total of 164 test subjects, consisting of 91 females and 73 males, satisfied the inclusion criteria. A total of 63 patients were excluded; 6 with visible osseous metastases in the thoracolumbar spine, 32 who only had a CT of the abdomen or pelvis, 20 that were outside the age ranges, 3 who did not have a biopsy proven cancer diagnosis, and 2 who had imaging beyond the eligible date range. The age group breakdown of test subjects that met both inclusion and exclusion criteria were as follows: 15 subjects age 40-49 “years-old;43 subjects age 50-59 years-old; 33 subjects age 60-69 years-old; and 10 subjects age 70–79 “years-old 18” subjects age 50-59 years-old and 6subjects 60-69 years-old were excluded chronologically in order to maintain 25 subjects per age group (Figure 1). Each age group consisted of a wide variety of cancers delineated by organ of origin (Table 2).
|
Table 2: Cancer delineated by organ of cancer origin correlated with patient’s age. |
||||
|
Cancer Diagnosis |
40-49 y |
50-59 y |
60-69 y |
70- 79 y |
|
Colorectal/anal |
7 |
10 |
3 |
3 |
|
Gastric |
2 |
1 |
2 |
|
|
Pancreatic |
4 |
3 |
3 |
2 |
|
Adrenal |
1 |
|||
|
Ovarian |
1 |
1 |
||
|
Breast |
1 |
|||
|
Small bowel |
2 |
1 |
||
|
Appendiceal |
1 |
1 |
||
|
Esophageal |
1 |
4 |
||
|
Melanoma |
1 |
1 |
||
|
Lymphoma |
1 |
|||
|
Bronchogenic |
1 |
3 |
1 |
|
|
Cervical |
2 |
1 |
||
|
Gall Bladder |
1 |
2 |
||
|
Endometrial |
3 |
1 |
||
|
Renal |
1 |
1 |
||
|
Unknown |
1 |
|||
A total of 421 control subjects, consisting of 234 females and 187 males, were reviewed. The date range reviewed was ultimately limited to February 1, 2014 through March 31, 2014 in order to obtain 25 subjects per age group and to match the reduced number of subjects in the 40-49 and 70-79 years-old test groups. A total of 261 patients were excluded; 33 who only had a CT of the abdomen or pelvis, 143 that were outside the age ranges, 78 with a history of cancer, 3 with suspicious masses, 1 with suspicious endometrial thickening, 1 with multiple spinal masses, 1 with repeat imaging within the same month, and 1 with a spinal stimulator. The age group breakdown for control subjects that met both inclusion and exclusion criteria is as follows: 50 subjects age 40-49 years-old; 61 subjects age 50-59 years-old; 34 subjects age 60-69 years-old; and 15 subjects age 70-79 years-old. 25 subjects age 40-49 years-old, 36 subjects age 50-59 years-old, and 9 subjects age 60-69years-old were excluded chronologically in order to maintain 25 subjects per age group (Figure 2).
Average severity score per age group was calculated by observer and as a composite average. The p–value was calculated for the three observers independently and as a composite score. The composite p-values were as follows: AC-0.10, FA-0.04, and SI-0.41 for the 40-49 years-old group; AC-0.43, FA-0.09, and SI0.26 for the 50-59 years-old group; AC-0.19, FA-0.32, SI-0.31 for the 60-69 years-old group; and AC-0.02, FA-0.28, SI-0.20 for the 70-79 age group. Therefore, only the FA severity scores between the 40-49 years-old test and control groups and AC scores in the 70-79 years-old test and control groups were statistically significant different (Table 1 and Figure3).
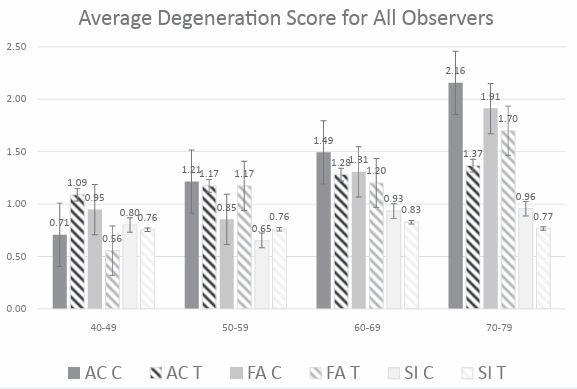
Figure 3: Graph demonstrating degenerative changes in the anterior column of the lumbar spine (AC), facet joints (FA) and sacroiliac joints (SI) with change in the subject age. This is a comparison between test group (with cancer) and control group (without cancer). The degeneration score is an average of the degeneration changes delineated by a 4 point scale.AC= 0- none, 1.0- minimal, 2.0- moderate, 3.0- severe. FA= 0- none, 1.0- minimal, 2.0- moderate, 3.0- severe.SI= 0- none, 1.0- minimal, 2.0- moderate, 3.0- severe. T= test group. C= control group. Solid bars= degenerative disease in the control group. Lined bars= degenerative disease in the test group.
Within this limitation, the AC degenerative severity score in the control group increased at a higher rate with increasing age compared to the test group. The average AC degenerative severity scores for the control group were 0.7, 1.2, 1.5, and 2.2 for the 40-49, 50-59, 60-69, and 70-79 years-old groups respectively and 1.1, 1.2, 1.3 and 1.4 for the test group. This corresponds to a 37% lower severity of DDD in the test group compared to control group in the 70-79 years-old group (Table 1 and Figure3)..
The average degenerative score in the 40-49 and 50-59 yearsold FA control groups minimally decreased from 1.0 to 0.8 while the degenerative score in the test group increased from 0.5 to 1.2. This is in opposition to the hypothesis that subjects with cancer experience less degenerative disease. The average degenerative score in the 60-69 and 70-79 years-old control group increased from 0.8 to 1.8 with a similar increase in the test group, from 1.2 to 1.7 (Table 1 and Figure3).
The average degenerative score in the 40-49 and 50-59 yearsold SI control groups minimally decreased from 0.8 to 0.7 and then increased from 0.9 to 1.0 in the 60-69 and 70-79 years-old group while the degeneratives core in the test group remained stable at 0.8 throughout all age groups (Table 1 and Figure 3).
Intraobserver reliability was calculated as a percentage for the three readers comparing the combined degenerative severity scores of 0 with 1(no and mild degenerative disease) and 2 with 3 (moderate and severe disease) for the control and test groups (Table 3).
|
Table 3: Intra observer reliability between musculoskeletal radiologist (MSK), neuroradiologist (Neu) and body imager (Body). Intra observer reliability was calculated as a percentage for the three readers comparing the degenerative severity scores of 0 combined with 1(no and mild degenerative disease) and 2 combined with 3 (moderate and severe disease) for both the control and test groups. Total intra observer reliability is an average of the three reader’s intra observer reliability. AC= anterior column of the spine. FA= facet arthropathy. SI= sacroiliac joints. Test= cancer group. Control= non-cancer group. |
||||
|
MSK/Neu |
MSK/Body |
Body/Neu |
Total |
|
|
AC Control |
88% |
82% |
81% |
84% |
|
AC Test |
83% |
85% |
92% |
87% |
|
FA Control |
89% |
72% |
79% |
80% |
|
FA Test |
93% |
73% |
80% |
82% |
|
SI Control |
82% |
78% |
80% |
80% |
|
SI Test |
89% |
88% |
96% |
91% |
This was done secondary to the subjective nature of scoring degenerative disease. The average intra observer reliability for all groups is 84 and 87% for the AC control and test groups respectively, 80 and 82% for the FA control and test groups respectively, and 80 and 91% for the SI control and test groups respectively (Table 3).
DISCUSSION
Imaging has become an integral part of the multidisciplinary approach to the diagnosis and staging of cancer, with MRI and CT imaging specifically playing an important role in medical patient care [8-14]. To date, there is no literature suggesting a correlation between DDD and cancer, however, it is not implausible that the two are related. Cancer is a complex group of biologically variable diseases with numerous outcomes, behaviors and risk factors. It is well established that cancer is caused by many external factors including infectious organisms, toxins, and diet as well as internal factors including hormones, genetic predisposition, immune conditions, and inflammatory factors [1]. The generation of DDD is also believed to develop secondary to a complex interplay of inciting factors related to one’s genetic predisposition and an inflammatory cascade in responses to stress or trauma [22].
Our study demonstrated that degenerative changes, including changes in the anterior column, facet joints and sacroiliac joints, increased with patient age in both test and control groups (Figure3). This was compatible with multiple prior studies in the literature [6,7,15-21]. However, our study additionally demonstrated that degenerative changes progress at a slower rate in patients with cancer compared to those without cancer. This is most pronounced in the anterior column and in subjects over 60 years of age.
Interestingly, the inverse relationship between cancer and DDD was seen in the younger patient population, which incidentally demonstrated a higher prevalence of GI related cancers compared to the older population (Table 2). This raises the question as to whether the pathophysiology behind the progression and development of certain cancer sub types play different roles in the occurrence and severity of DDD.
The facet and sacroiliac joint degenerative changes decreased or were stable in subjects 40-49 to 50-59 and increased as expected from 60-69 to 70-79 years of age without a statistically significant divergence. This correlated with the degenerative changes described in the literature [5,6,15,16,19].
It is possible that certain inflammatory cytokines or cascades triggered during the development of DDD charge the immune system to mitigate aberrant cells preventing oncogenesis. Alternatively, the inflammatory cytokines or cascades triggered during the development of malignancy may inhibit the development of DDD [23]. Likewise, certain genetic factors linked to the development of cancer may inhibit the generation of the DDD, or genetic factors linked to the development of DDD may inhibit the generation of cancer.
Our study was designed as a preliminary evaluation of a hypothesis that presumes a relationship between cancer and DDD. There are several limitations to our study, including a retrospective approach, single center study, and a relatively small sample size. Given the retrospective nature of the study, it is impossible to predict if any of the patients in the control group would later develop cancer. Additionally, while we attempted to eliminate as much selection bias as possible, we are unable to completely eliminate the possibility that some subjects within the control group had an inherent increased propensity for DDD due to factors not delineated in their history and physical exam. It is our hope that presenting this unexpected relationship will incite subsequent research initiatives or hone current projects to elucidate the specific factors governing this inter play. Once exposed, these factors could then be used to formulate novel therapeutic and preventative options for cancer.
REFERENCES
1. Currently Funded Cancer Research.
2. Howlader N, Noone AM, Krapcho M, Miller D, Bishop K, Altekruse SF, et al. SEER Cancer Statistics Review. 1975-2013.
7. Kalichman L, Guermazi A, Li L, Hunter DJ. Association between age, sex, BMI and CT-evaluated spinal degeneration features. J Back Musculoskelet Rehabil. 2009; 22: 189-195.
18.Resnick R, Niwayama G. Degenerative disease of the spine. In: Resnick D. Diagnosis of bone and joint disorders. Philadelphia, PA: WB Saunders Company. 1995. 1372-13462.
22.Stewart BW, Wild CP. Cancer etiology. World Cancer Report. 2014.









































































































































