Erectile Dysfunction as a Sentinel Presenting Feature of Cauda Equina Syndrome
- 1. Department of Neurosurgery, The Alfred Hospital, Australia
Abstract
Cauda equina syndrome is a neurosurgical emergency that can be a diagnostic challenge as no single history or examination feature has been found to be pathognomonic. We present the case of a twenty-seven-year-old male presenting only with erectile dysfunction and found to have critical cauda equina compression from a large disc prolapse. Whilst sexual dysfunction is a recognized complication of spinal cord injury, the prevalence of erectile dysfunction as a presenting symptom of cauda equina compression is not known. Sexual histories are often poorly taken by clinicians and this case highlights that erectile dysfunction alone can signify cauda equina syndrome.
Keywords
Cauda equina syndrome , Erectile dysfunction,Disc prolapse, Neurosurgery, Spinal surgery.
CITATION
Pham C, Tee JW (2018) Erectile Dysfunction as a Sentinel Presenting Feature of Cauda Equina Syndrome. JSM Spine 3(1): 1014.
ABBREVIATIONS
CES: Cauda Equina Syndrome; MRI: Magnetic Resonance Imaging
INTRODUCTION
No single history or examination finding is pathognomonic for cauda equina syndrome, which can be represented by a broad constellation of symptoms and signs [1,2]. As such, understanding the neuroanatomy of the cauda equina and its nerve roots is critical for the prompt work up and diagnosis [3]. Whilst sexual dysfunction is recognized as a possible complication of spinal cord injury, erectile dysfunction as the only feature of acute cauda equina syndrome has not previously been reported. Sexual histories are often overlooked by clinicians and this case signifies that it can signify critical lumbosacral pathology.
CASE PRESENTATION
A twenty-seven-year-old male presents with erectile dysfunction. He reported an initial two weeks of lower back pain that resolved by the time of review, whereby the only symptom of note was sexual dysfunction. There was no history of lower limb radicular pain, weakness, paresthesia, numbness or bowel and bladder dysfunction
Lower limb neurological examination was unremarkable with normal sensation to light touch in all dermatomes. Ankle reflexes were present bilaterally. Power was full and equal at all movements. Anal tone was unremarkable on digital rectal examination.
Lumbar spine magnetic resonance imaging (MRI) elicited severe spinal canal stenosis at the S1 level secondary to posterior protrusion of a degenerative L5/S1 disc (Figure1,2).
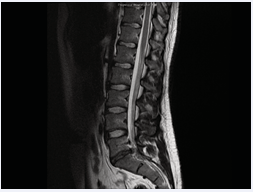
Figure 1: Sagittal T2 weighted MRI showing extruded disc (from L5/S1) causing central compression of the thecal sac at the S1 level just after the S1 nerve roots have lateralized.
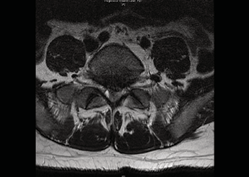
Figure 2: Axial T2 weighted MRI at the level of L5/S1 showing extruded disc (from L5/S1) causing central compression of the thecal sac at the S1 level just after the S1 nerve roots have lateralized.
There was loss of cerebrospinal fluid signal surrounding the cauda equina fibres consistent with cauda equina compression.
The patient proceeded to an emergency S1 laminectomy and discectomy. He had an uncomplicated recovery and was discharged day two post-operatively. He reported resolution of his erectile dysfunction the day after surgery.
DISCUSSION
The spinal cord terminates at the level of the first and second lumbar vertebrae as the conus medullaris. Lumbosacral nerve roots exiting distal to this are gathered in a ‘horse-tail’ appearance known as the cauda equina. Compression can result in cauda equina syndrome (CES). Somatic and autonomic neuroanatomical pathways are both involved in the normal penile erection. Somatosensory and motor function innervating sacral dermatomes (e.g. penile skin, glans) and skeletal muscle (e.g. ischiocavernosus, bulbospongiosus) travel by peripheral nerves and communicate with the spinal cord via the cauda equina nerve roots. These somatic pathways either synapse (sensory) or originate (motor) at cell bodies in the second to fourth sacral segments of the spinal cord. Onuf’s nucleus, located at S2-S4, is the major somatomotor centre of penile innervation.
Preganglionic parasympathetic fibres also arise from the second to fourth sacral spinal cord segments, exiting via the cauda equina to pass in pelvic nerves to the pelvic plexus and innervate smooth muscle cells of the corpora cavernosa and penile vasculature responsible for tumescence. Sympathetic innervation of urogenital viscera bypasses the cauda equina,
“red flags” for CES, there is a paucity of available literature on the prevalence of erectile dysfunction as a presenting symptom. Whilst sexual dysfunction is a recognized complication in patients with spinal cord injury, to our knowledge there are no documented cases of erectile dysfunction as the single, sentinel feature signifying cauda equina compression [4]. Sexual histories are often poorly taken and this case highlights its critical importance.
Severe back pain, urinary retention and lower limb weakness are well known to be suggestive of CES [1,2,5]. Saddle sensory deficits has also been reported to be a positive predictive feature on examination [1]. However, no single history or examination feature has been found to be pathognomonic for CES [1,2]. CES is a neurosurgical emergency indicating imminent or active lumbosacral nerve fiber damage from which recovery of neurologic deficits is uncertain. Whilst CES may be an uncommon cause of erectile dysfunction and other causes require exclusion, physician vigilance and knowledge of the neurological function conveyed by the nerves contained within the cauda equina is crucial in the diagnosis and treatment of CES [3].
REFERENCES
4. Podnar S. Oblak C, Vodusek D. Sexual function in men with cauda equina lesions: a clinical and electromyographic study. J Neurol Neurosurg Psychiatry. 2002; 73: 715-720.









































































































































