Rare and Unusual Case of Intramedullary Spinal Cord Neurofibroma
- 1. Department of Pathology, Anderson Cancer Center, USA
- 2. Department of Pathology, Hospital Nacional Edgardo Rebagliati Martins, South America
- 3. Department of Neurosurgery, MD Anderson Cancer Center, USA
- 4. Department of Neuro Imaging, MD Anderson Cancer Center, USA
Abstract
A previously healthy eighteen year old female presented with interscapular pain of 6 months duration. She also experienced progressive decline in her ability to perform fine motor skills such as handwriting as well as deficiency in coordination and motor strength. Imaging of the spine revealed a well demarcated intradural intramedullary lesion in the central portion of the cervical spinal cord. Based on radiographic appearance a diagnosis of ependymoma was favored. To prevent further motor and sensory decline, surgical intervention was deemed appropriate. Osteoplastic laminoplasty of C6 and C7 was performed with microsurgical resection of the lesion using concurrent somatosensory and motor evoked potentials. Subsequent microscopic assessment of the resected mass showed a benign nerve sheath tumor, further classified as neurofibroma. Intradural intramedullary neurofibromas are extremely rare neoplasms with only a handful of reported cases. In this report we would like to share our experience with this entity.
Keywords
Neurofibroma ; Intramedullary ; Cervical spine.
CITATION
Jedrzkiewicz J, Salazar R, Weinberg JS, Tatsui CE, Guha-Thakurta N, et al. (2016) Rare and Unusual Case of Intramedullary Spinal Cord Neurofibroma. JSM Spine 1(1): 1003.
INTRODUCTION
The most common intraspinal tumors are meningiomas and schwannomas, which are dural based or grow around nerves, respectively [1]. Intramedullary spinal tumors are rare lesions more commonly encountered in children and account for only 4% of all central nervous system tumors [2]. The radiographic differential diagnosis depends on the position of the lesion within the spinal cord. A central spinal cord location is more typical for ependymomas and peripheral position is more common in astrocytomas [1,3]. Although non-glial tumors and metastases can occur in the intramedullary spinal cord, the overwhelming majority (80-90%) are glial neoplasms [3]. Notably, intramedullary neurofibromas are very rare with only handful reported cases. Herein, we report a pediatric case of an intramedullary neurofibroma of the spinal cord and discuss our experience with this diagnosis and subsequent management.
CASE PRESENTATION
The patient’s consent was obtained according to the ethical committee of MD Anderson Cancer Center, Houston, TX. An eighteen year old female with no significant past medical or family history, presented with interscapular pain of six months duration. Her symptoms persisted and worsened over time. She started to experience headaches, numbness and tingling in her hands (more severe on the left side), a decline in her ability to perform fine motor skills such as handwriting as well as deficiency in coordination and motor strength. Her neurologic exam demonstrated intact cognitive function and no abnormalities in cranial nerves. Muscle strength was 5/5 in all groups tested with the exception of the left hand, which was 4+ in the hand intrinsic muscles. Reflexes were increased to 3+, and there was Hoffmann sign on the left hand. Babinski and Romberg signs were negative and gait was unassisted. The proprioception and superficial sensation were intact. There was no significant family history. Her magnetic resonance imaging of the spine, revealed an intramedullary lesion in the cervical cord centered at the C7 level. The lesion demonstrated contrast enhancement, T2 hypointensity and measured 14 mm in its maximum craniocaudal dimension (Figure 1A and 1B).
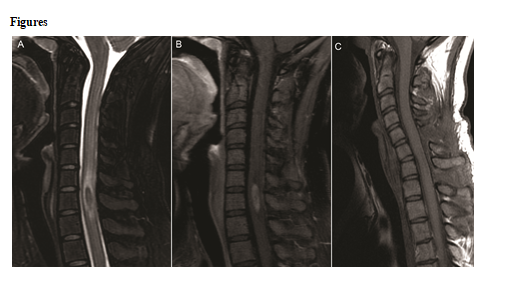
Figure 1 Magnetic resonance images. A – sagittal T2 weighted image demonstrating a T2 hypointense lesion centered within the cord at the C7 level with surrounding hyperintensity reflective of edema, B – sagittal T1 weighted post contract image demonstrating enhancement within the lesion, C – sagittalT1 weighted post contract image on postsurgical follow up.
There was surrounding T2 hyperintestinty reflective of edema, which mildly increased in extent on subsequent scans. There was no significant alternation in size of the lesion over the duration of 5 months.
Although the patient was being followed with serial scans, surgical intervention was deemed appropriate to prevent further motor and sensory decline. An osteoplastic laminoplasty of C6 and C7 with microsurgical resection of the lesion using intraoperative somatosensory and motor evoked potentials was performed. During the surgery, a plane of cleavage between the tumor and the normal cord was difficult to obtain because of the consistency and color of the tumor, which blended with the surrounding normal tissue. Postoperative assessment demonstrated incomplete tetraparesis with gait abnormality and neuropathic and nociceptive pain. Symptoms improved after rehabilitation. At six months follow up patient had bilateral leg tingling and back pain and intermittent numbness in hands bilaterally. Her postoperative changes appear to be resolving on follow up (Figure 1C).
Microscopic examination showed a hypocellular tumor composed of small wavy hypochromatic spindle cells, which were mitotically inactive. Admixed were collagen bundles and nerve twigs (Figure 2A). The vessels were small and inconspicuous without hyalinization. The microscopic appearance of the tumor was classic for a neurofibroma but the differential diagnosis included schwannoma, solitary fibrous tumor and ganglioglioma.
Immunohistochemical stains were performed to confirm the microscopic impression. Results of immunohistochemical stains showed that the tumor cells were positive for S-100 protein (Figure 2B) and GFAP, but negative for STAT6, synaptophysin and NeuN. Masson’s trichrome special stain highlighted bundles of collagen. Admixed axons were highlighted by neurofilament immunohistochemical stain and this finding can be seen in neurofibromas (Figure 2C). Verocay bodies, Antoni A and B areas were not identified, thus arguing against diagnosis of schwannoma. STAT6 and CD34 immunohistochemical stains were negative, excluding a diagnosis of solitary fibrous tumor. Additionally, synaptophysin and NeuN immunohistochemical stains were negative in the tumor cells arguing against ganglioglioma. The Ki-67/MIB1 proliferation index was less than 2%, consistent with an indolent lesion (Figure 2D).
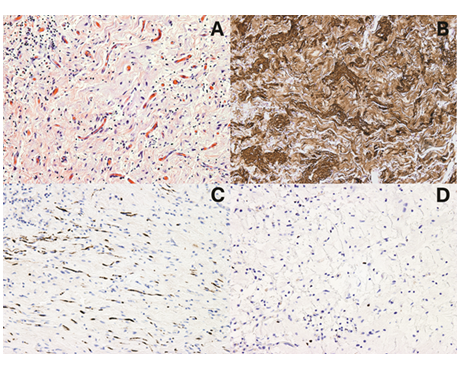
Figure 2 10 X microscopic images. A – H and E section, B – S100 protein immunohistochemical stain, C – neurofilament immunohistochemical stain, D – Ki-67/MIB1 immunohistochemical stain.
The immune profile was in keeping with the diagnosis of neurofibroma. This case was reviewed by two neuropathologists who agreed with the rendered diagnosis.
DISCUSSION
Neurofibromas and schwannomas belong to family of a benign nerve sheath tumors that are thought to arise from Schwann cells in the peripheral nervous system. Hence, central nervous system localization is unusual for these lesions. Spinal nerve sheath tumors are predominantly schwannomas [4]. In a review of 221 spinal nerve sheath tumors in 199 patients Safaee et al, reports that 53 cases were neurofibromas, 163 schwannomas and 5 malignant peripheral nerve sheath tumors. In their cohort, the most common location for the neurofibromas was cervical spinal cord (74% of cases) and most cases were intradural (66%) with the remaining located in extradural paraspinal tissue. Additionally, 56% of cases were associated with neurofibromatosis type 1 [4]. In this review, none of the neurofibromas were located in the intramedullary spinal cord. Both schwannomas and neurofibromas are generally considered benign and most are sporadic. The risk of malignant transformation is negligible in small sporadic neurofibromas unlike in large plexiform or diffuse lesions [5].
The incidence rate of intramedullary spinal cord neurofibroma is unknown [1,4,6-8]. The available reported cases occurred in adult patients (20 to 62 years old) with male to female ratio of 4:5 without neurofibromatosis type 1 association (Table 1) [9-16]. Seven reported cases occurred in cervical spinal cord with the remaining two cases in thoracic cord and the conus medullaris. Thus, the cervical spinal cord is probably the most common site of occurrence for these lesions. Our case of an intramedullary spinal cord neurofibroma occurred in an eighteen yours old female at an unusually young age for presentation in comparison to the prior reported cases. However, her symptoms and location of the lesion were similar to the already reported cases.
Many patients initially present with paraesthesia, pain and weakness. Persistence or progression of these symptoms may trigger medical evaluation and subsequent excision of the mass. A definitive diagnosis of intramedullary neurofibroma is made upon pathologic review of the tumor. Postoperatively, a proportion of patients experience persistent neurological symptoms and/or deficits but long term follow up is not currently available (Table 1).
|
Table 1: Table summarizing available literature on intradural intramedullary neurofibromas with available follow up and outcome [9-16]. |
|||||||
|
Author |
Sex |
Age |
Location |
Size |
Symptoms |
Outcome |
Follow up |
|
Young et al |
F |
33 |
Conus medullaris |
- |
Paresthesia and weakness in legs |
Weakness in lower limbs |
4 months |
|
Sharma et al |
M |
27 |
C5-6 |
- |
Weakness in upper & lower limbs |
Partial recovery of strength |
- |
|
Gelabert Gonzalez et al |
F |
29 |
C2-4 |
4x2 cm |
Paresthesia of hands |
Deficit in the left hand |
- |
|
Sharma and Newton et al |
M |
20 |
C7 |
- |
Weakness in upper limbs |
- |
- |
|
Oka et al |
F |
62 |
C3-4 |
- |
Paresthesia of hands/feet |
- |
- |
|
Gelabert et al |
F |
50 |
C2-4 |
- |
Tetraparesia & paresthesia |
Recovery of strength in limbs |
- |
|
Fagundes et al |
M |
24 |
C6-T1 |
5x4x2cm |
Paraparesia, hypoesthesia |
Partial recovery |
18 months |
|
Arishima et al |
M |
52 |
T4-5 |
- |
Paraparesia |
No change |
- |
|
Current case |
F |
18 |
C6-7 |
1.9 cm |
Interscapular pain, paresthesia of hands |
Paresthesia in legs/hands |
6 months |
|
Abbreviations F – Female; M – Male |
|||||||
The surgical management of intramedullary lesions is challenging because the overall outcome depends on the eloquence of the surrounding tissue [2,3]. If the risk of damage to the spinal cord is minimal, a complete resection may be attempted particularly for benign appearing lesions. Modern surgical techniques include microsurgery, which is the mainstay of treatment for intramedullary tumors. However, recurrence and long term prognosis is often dictated by the histologic classification of the tumor and completeness of resection [2,4]. Neurofibromas are considered biologically indolent lesions and none of the nine reported cases of intradural intramedullary neurofibromas showed tumor recurrence after surgical excision (Table 1).









































































































































