Surgical Outcomes and Complications of Pedicle Screw Fixation in 200 Cases of unstable Cervical Spinal Injuries - Comparison between Plate Systems and Rod Systems
- 1. Department of Orthopedic Surgery, Wakayama Medical University Wakayama, Japan
- 2. Department of Orthopedic Surgery, Chubu Rosai Hospital, Japan
Abstract
Introduction: Surgical outcomes and complications in the patients, who underwent posterior spinal fusion with pedicle screws for unstable cervical spinal injuries, were investigated comparing plate systems and rod systems. The relative merits of plate systems (non-constrained type) and rod systems (constrained type) were discussed.
Summary of Background Data: Cervical pedicle screw fixation is an effective procedure for stabilizing an unstable motion segments, however it has not widely been used because it has generally been considered too risky due to the potential risk for injury neurovascular structures, such as vertebral arteries, spinal cord or nerve roots. The authors reported a study to introduce the imaging technique in which pedicle axis views were obtained using fluoroscope to show the screw entry point matched with trajectory angle.
Discussion and Conclusion: Cervical pedicle screw fixation using a fluoroscopy assisted pedicle axis view technique provided good clinical result in both plate and rod systems. Although 107 of 883 screws demonstrated screw malposition, the incidence of complications associated with instrumentation was relatively low. There were less surgery-related complications in rod systems, comparing plate systems.
Keywords
Pedicle screw fixation; Cervical spine; Spinal injury; Pedicle axis view; Fluoroscope; Placement; Complications.
CITATION
Yukawa Y, Nakashima H, Morita D, Matsumoto T, Ito K, et al. (2018) Surgical Outcomes and Complications of Pedicle Screw Fixation in 200 Cases of unstable Cervical Spinal Injuries - Comparison between Plate Systems and Rod Systems -. JSM Spine 3(1): 1015.
INTRODUCTION
Cervical pedicle screw fixation is superior to other techniques in terms of promoting mechanical strength [9,12]. The concept of pedicle screw fixation for mid- and lower cervical spine reconstruction was introduced by Abumi et al., in 1994. [1,8] Several authors have reported good clinical results and relatively low rates of complications from this procedure [1-3,21,23-25]. However it has the potential to seriously injure the spinal cord, nerve roots or vertebral arteries. Pedicle screw fixation still has been considered a risky surgery in mid- and lower cervical spine. [19] For cases in which posterior wiring or lateral mass platingv cannot be applied [6,20,22], transpedicular fixation may provide optimal stabilisation for an unstable motion segment [9,12,14]. Therefore, if the safety of the procedure is ensured, cervical pedicle screw fixation could become an effective procedure for reconstructing the cervical spine.
`Previous anatomical studies have demonstrated that the small diameter of mid-cervical pedicles, large obliquity of the cervical pedicle axis and individual variations in cervical pedicle size limit the application of pedicle screws for cervical spine reconstruction [10,15,18,21]. Nevertheless, broad guidelines have been developed to successfully locate the entry point for cervical pedicles on the lateral mass [1, 2, 8, 11], and the rate of successful screw placement may be as high as 87.5% [16]. Because of the lack of landmarks and an accurate entrance to the cervical pedicles, direct exposure of the pedicle cavity [1], foraminolaminotomies [7,15] and the use of expensive stereotactic imageguided systems or computed tomography (CT) [13] have been suggested as ways to improve the accuracy of screw placement.
There are few reports that have described the difference by instrumentation systems, in terms of surgical results and clinical complications of pedicle screw fixation. The purpose of this study was to investigate surgical outcomes and complications of pedicle screw fixation for unstable cervical spinal injuries, in the large scale of materials. Also the difference between two techniques; plate system and rod systems were studied.
MATERIALS AND METHODS
Patients
From 1995 to 2014, 200 consecutive patients with unstable cervical spine injuries underwent posterior spinal fixationwith pedicle screw instrumentation. They were 172 males and 28 females and their mean age was 46.9 years (range; 14–90 years). The patients’ neurological status was graded according to the ASIA classification system. There were 74 cases of ASIA A, 15 of ASIA B, 33 of ASIA C, 47 of ASIA D and 31 of ASIA E. The types of fractures and dislocations were categorised according to the mechanistic classification of Allen et al. [4], of the 200 cases, 103 were distractive flexion (DF) injuries, 40 were compressive flexion (CF), 34 were compressive extension (CE), 13 were distractive extension (DE) and 10 were vertical compression (VC).
These 200 patients were retrospectively enrolled in the present study. This study was ethically approved by institutional research committee (201409-04). Radiography (AP, lateral and oblique views), CT and magnetic resonance imaging (MRI) was performed in all patients preoperatively. Pedicle morphology and the medial inclination of the pedicle axis were evaluated upon CT examination. CT angiography was routinely obtained in most of cases to observe patency of vertebral arteries, with the exception of emergency case or allergy of contrast agent.
The surgeries were performed by one of the three attending and certified spine surgeons who were well experienced with the thoraco-lumbar pedicle screw fixation. All surgeries were done with pedicle axis view technique by fluoroscope which was previously reported [24,25]. Five different instrumentation systems were used: Axis screw fixation (100 cases), Olerud cervical system (3), Vertex system (1), OASYS system (79) and Synapse system (17). Representative surgical cases of both plate and rod systems were shown in (Figure 1,2).
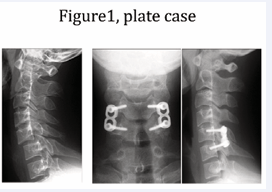
Figure 1: Representative plate case. Left; preoperative lateral X-ray, Middle and Right; postoperative AP and lateral X-ray.
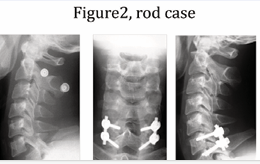
Figure 2: Representative rod case. Left; preoperative lateral X-ray, Middle and Right; postoperative AP and lateral X-ray.
The patients began postoperative rehabilitation within a few days after surgery. A Philadelphia collar was worn for approximately one month, but no external fixation was applied to the patients with ASIA A or B neurological deficit.
Neurological complications were assessed by reviewing preoperative, immediate postoperative and follow-up neurological examinations. Postoperative infection and vascular complications were evaluated by reviewing operative reports, patients’ medical records and clinical notes. Instrumentation failure was reviewed using postoperative radiographs and CT scans. Bony union was investigated with flexion-extension radiographs at the final follow up. No apparent motion between adjacent spinous processes or bony bridges between facets was considered to be fused. The sagittal alignment of the cervical vertebrae around the injured segment was measured on pre- and postoperative lateral radiographs.
The accuracy of the placement of the pedicle screws into the medial/lateral pedicle walls was evaluated on axial CT scans, whereas superior/inferior pedicle wall screw location was examined on oblique radiographs. The position of the cervical pedicle screws was assessed by independent radiologists. Incorrect screw placement was classified as either Grade I;
screw exposure or Grade II; pedicle perforation. [23] A screw exposure was assumed if a screw broke the pedicle wall but more than 50% of the screw diameter remained within the pedicle. A pedicle perforation occurred if it breached the pedicle wall and more than 50% of the screw diameter was outside the pedicle. The latter indicated a potential risk for neurovascular injury (Figure 3).
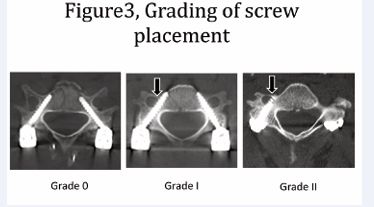
Figure 3: Grading of screw placement.Screw placement was classified as Grade 0; intact, Grade I; screw exposure and Grade II; pedicle perforation. Grade I (screw exposure) was assumed if a screw broke the pedicle wall but more than 50% of the screw diameter remained within the pedicle. Grade ii (pedicle perforation) occurred if it breached the pedicle wall and more than 50% of the screw diameter was outside the pedicle.24
Statistical Analysis
The data were analyzed using the SPSS version 13.0 software (SPSS Inc., Chicago, IL). Descriptive statistics were calculated for all subjects and separately for plates and rods systems in the form of mean value and standard deviation. Comparison between the plate system and the rod system was carried out byχ2 test and un-paired Student t tests. Statistical significance was set at a level of P <0.05.
RESULTS
The mean operative time was 111 minutes (range, 52–377 minutes) and the mean blood loss was 184 ml (range, 10–2100 ml). Four anterior reconstructive surgeries with iliac bone grafts and 25 posterior decompressive surgeries were performed simultaneously. Local sagittal alignment around the injured lesion measured 5.9° of kyphosis preoperatively and 6.7° of lordosis at the last follow-up. Eight hundred eighty three pedicle screws were used in total; 71 (8.0%) showed Grade I (screw exposure) and 36 (4.1%) demonstrated Grade II (pedicle perforation). Of these 107 screws, 34 (32%) breached the medial pedicle wall, 72 (67%) the lateral wall, and 1 (1%) the infra lateral wall (Table 1).
|
Table1: Clinical outcomes and accuracy of screw placement in both plate and rod systems.?Comparison between the plate system and the rod system was carried out byχ2 test for number of screws and un-paired Student t tests for operative time and bleeding. Statistical significance was set at a level of P <0.05. |
|||
|
|
Plate system |
Rod system |
P value |
|
Cases |
100 |
100 |
|
|
Operative time |
97.6±38.2 |
125.2±49.1 |
<0.001 |
|
Bleeding during surgery |
221 ± 243 |
147 ± 168 |
0.014 |
|
Average fixation levels |
1.5 |
1.6 |
|
|
Number of screws |
403 |
480 |
|
|
Grade I (screw exposure) |
41 (10.2%) |
30 (6.3%) |
NS (<0.1) |
|
Grade II (pedicle perforation) |
17 (4.2%) |
19 (4.0%) |
NS |
|
malposition |
58 (14.3%) |
49 (10.2%) |
NS (<0.1) |
There were 3 cases with intraoperative complications: 2 cases with a penetration of the pedicle probe into the vertebral artery and one with transient radiculopathy. The bleeding from the vertebral artery was easily stopped with bone wax and there were no further complications postoperatively. Because one patient had pedicle and articular process fractures caused by the presenting trauma, it was difficult to control the trajectory of the probe into the broken pedicle during surgery; however, radicular pain was gradually relieved with time. Eleven postoperative complications occurred: 4 cases associated with loss of correction due to instrumentation failure (screw dislodgement, breakage and loosening), 4 cases with loss of correction (more than 10 degrees) and 3 deep wound infections. These 8 cases with instrumentation failure or correction loss were firstly treated with screw- plate system (non-constrained fixation) in 6 cases (6%) and screw-rod system (constrained fixation) in 2 cases (2%). Only 1 case with screw – rod dislodgement underwent revision surgery with same rod system. Remaining 7 cases obtained the bony fusion in situ. The postoperative deep infection was successfully managed by surgical debridement, continuous irrigation and intravenous administration of antibiotics without the need to remove the hardware (Table 2).
|
Table2: Complications in both plate and rod systems.Comparison between the plate system and the rod system was carried out byχ2 test. Statistical significance was set at a level of P <0.05. |
|||
|
|
Plate system |
Rod system |
P value |
|
Cases |
100 |
100 |
|
|
VA penetration |
1 |
1 |
NS |
|
Nerve root injury |
1 |
0 |
NS |
|
Spinal cord injury |
0 |
0 |
NS |
|
Wound infection |
2 |
1 |
NS |
|
Implant failure |
3 |
1 |
NS |
|
Correction loss (>10 degrees) |
3 |
1 |
NS |
|
Dead cases |
3 |
1 |
NS |
|
Total # of complications |
13 |
5 |
NS (<0.1) |
Four patients died of renal failure (n=1), pneumonia (n=2), or pulmonary embolism (n=1) within 2 months of surgery. All of these patients suffered from ASIA A neurological injury above C5 level. The remaining 196 patients were followed up for more than 6 months after surgery. The mean follow-up duration was 22.7±24.6 months. Good cervical vertebrae alignment was maintained at final follow-up in 188 of the 196 patients (96%). Finally the bony fusion was obtained in all cases. Pre- and postoperative tracheotomy was required in 27(13.5%) of the 200 patients. Because the patients underwent posterior surgery alone without postoperative external fixation, the tracheotomies were easily performed.
DISCUSSION
Cervical pedicle screw fixation has been shown to be the most stable form of cervical instrumentation [9,12,14]. However, due to the close proximity of the spinal cord, nerve roots and vertebral arteries, this type of surgery is generally considered too risky [19]. The purpose of the present study was to investigate the clinical outcomes and complications in both plate and rod systems of pedicle screw fixation and compare those two systems.Cervical pedicle screw fixation with both plate and rod systems provided good clinical results. Although 107 of 883 screws demonstrated screw malposition, the incidence of serious complications associated with instrumentation was relatively low. We found that it was much easier to perform a tracheotomy in patients treated with posterior cervical pedicle screw fixation than in those treated with anterior cervical surgery or Halo vest fixation [17].
In this study, cervical pedicle screw fixation provided good correction of sagittal alignment, a high fusion rate and only a few surgical complications. Several authors reported their surgical outcomes and complications using pedicle screw technique. However there was no comparative study comparing different instrumentation system like as screw & plate systems and screw & rod systems. Screw & plate systems were semi-constrained instrumentations and screw & rod systems were constrained (rigid) ones. We have experienced four cases of instrumentation failure and four cases of large correction loss in these series. Screw – plate system was used in 6 cases of these 8cases. The average surgical time was shorter in screw & plate systems than that in screw & rod systems, due to the simplicity of connection. Screw & rod systems provided more rigid strength and reduced the incidence of instrumentation failure and correction loss. As there was 9 years interval of initiation of both procedures, some improvement of fixation strength might be added in subsequent systems.
Anatomically, the cervical pedicle diameter is smaller than the thoraco-lumbar pedicle, and the pedicle axis is largely inclined in the transverse plane [7,10,11,15,18,21]. Successful placement of pedicle screws requires an accurate identification of the pedicle axis. If an accurate entry point that coincided with the correct trajectory angle is determined during surgery, it would vastly improve the accuracy of screw placement. Fluoroscopic lateral imaging was recommended in a study describing the conventional technique [1], but this method only provides information regarding the vertical plane and not the horizontal plane. Sometimes in lateral images, the pedicles in the lower cervical spine are difficult to visualise due to the overlying shoulders, but we had no such problem in locating the correct entry points using the pedicle axis view technique. Although cadaver studies have described detailed surface landmarks for a posterior cervical pedicle entrance, the cervical lateral masses have small bony undulations that differ from the thoracic or lumbar spine [11,15]. In fact, during surgery, there are fewer morphometric landmarks than in cadaver demonstrations. Furthermore, the location of the pedicle entrance is unique to each level of the cervical vertebra and large variations are found among individuals even at the same vertebral level [11,15]. A computer-guided surgical navigation system has been reported to improve the accuracy of screw placement. However these systems are cumbersome, time consuming and not easily equipped due to expensive price [5,13,16]. Navigation system provides virtual reality images (= memorised images), and sometimes needs correction by the realtime images to adjust gap between virtual reality and actuality.
The fluoroscopy-assisted pedicle axis view technique helped to determine the appropriate entry point that coincided with the correct trajectory angle for each cervical vertebra in both sagittal and transverse planes. The strength of this technique is indicating both inserting point and trajectory angle of screws simultaneously. If each of them is not correct, pedicle perforation are likely to occur. The all-manual-procedure without usage of a power drill, which the authors employed, caused only a few neurovascular complicationswithout any severe after-trouble. Vertebral arteries occupy 27-36% of transverse foramen between C3 and C6 levels [26]. Fortunately all pedicle screws were clinically silent in these series, despite some rate of screw dislodgement.
There are a few limitations in this paper. First the materials of each group are not equivalent. The patients in plate system underwent surgery from 1995 to 2003, and those in rod system from 2004 to 2014. There is an apparent difference in surgeon’s experience and instrumental advancement between former plate system and latter rod system. However the surgeons have a lot of experience in spinal instrumentation surgery, and the surgical technique of inserting pedicle screws are almost similar.
CONCLUSIONS
In the present study, pedicle screw fixation provided good reduction, a high fusion rate and relatively few complications in the treatment of cervical spine injury. Of the 883 cervical pedicle screws, 71 (8.0%) demonstrated screw exposure and 36 (4.1%) pedicle perforation. Rod & screw systems are likely to have stable fixation and less postoperative complications, comparing with plate & screw system.
REFERENCES
19.Roy-Camille R. Rationale and Techniques of Internal Fixation in Trauma of the Cervical Spine. In Errico T, Bauer RD, Waugh T (eds). Spinal Trauma. Philadelphia, JB Lippincott 163-191, 1991









































































































































