Full Remission of Brown Tumours after Treatment of Parathyroid Carcinoma
- 1. Endocrinology Department of CHU Ibn Rochd of Casablanca, University Hassan II, Morocco
- 2. Nuclear Medicine Department of CHU Ibn Rochd of Casablanca, University Hassan II, Morocco
Abstract
Parathyroid carcinoma is a rare disease which accounts for less than 1% of all case of primary hyperparathyroidism (HPT) and is usually not detected until the time of surgery or thereafter. Ten to twenty percent of patients with primary HPT have bone diseases. A radical excision remains the standard management.
We report a case of a man of 48 years old who had a past history of pelvis fracture with bone pain, and severe hypercalcaemia without signs of kidney stones. Serum total calcium was markedly elevated at 150 mg/L and intact PTH was 30 times above the normal range. CT scan suggested a right parathyroid mass of 4.12 x 3.85 x 5.42 mm.
Hypercalcaemia was treated with intravenous fluids and hydrocortisone, diuretics and cinacalcet. Surgical exploration and total parathyroidectomy of the tumour was performed; the remaining 3 glands were normal in size and shape. Histology revealed parathyroid carcinoma with foci of capsular and vascular invasion. Parathyroid MIBI scintigraphy was normal and bone scan revealed multiple hyperactive foci. The control bone scintigraphy 6 months after surgery showed a radiological cleanup.
The control after one year showed no recurrence with normal serum calcium levels.
KEYWORDS
• Parathyroid carcinoma
• Hypercalcemia
• Hyperparathyroidism
CITATION
Essabah HN, Siham EA, Amal G, Asma C (2017) Full Remission of Brown Tumours after Treatment of Parathyroid Carcinoma. JSM Thyroid Disord Manag 2(1): 1005.
INTRODUCTION
Parathyroid carcinoma is a rare clinical entity comprising 0.5 to 2% of patients who present with primary hyperparathyroidism [1]. It presents a diagnostic and therapeutic dilemma. Patients usually present with a severe form of hyperparathyroidism at diagnosis, such as bone disease, renal disease, or hypercalcaemic crisis, in contrast to the relatively asymptomatic presentation of benign parathyroid disease [2]. Ten to twenty percent patients with primary HPT have bone diseases
It is generally accepted that surgery is the treatment of choice for parathyroid cancer and bloc resection of the tumor at the time of initial surgery seems to offer the only chance for long-term control of the disease [3].
This case report describes a patient with parathyroid cancer with Brown tumors and his management.
CASE PRESENTATION
Our case is about a man aged 48 years who had a past history of pelvis fracture with bone pain, and severe hypercalcaemia without signs of kidney stones. Serum total calcium was markedly elevated at 150 mg/L and intact PTH was 30 times above the normal range. Examination of the neck was normal and Ultrasound didn’t show any parathyroid mass. No scintigraphy has been performed before the surgery, but the CT scan suggested a right parathyroid mass of 4.12 x 3.85 x 5.42 mm (Figure 1).
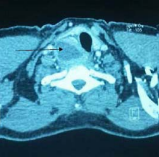
Figure 1 Tomographic scan of the neck showing a right parathyroid mass.
The hypercalcaemia was treated with intravenous fluids and hydrocortisone, loop diuretics and cinacalcet achieving a serum calcium level of 115 mg/l pre-operatively. Surgical exploration and total parathyroidectomy of the tumour was performed; the remaining 3 glands were normal in size and shape. Histology revealed a tumour with foci of capsular and vascular invasion. Postoperatively, the patient developed hypocalcaemia that required treatment with calcium therapy.
Parathyroid MIBI scintigraphy was normal and bone scan revealed multiple hyperactive foci. The control scintigraphy 6 months after surgery showed a radiological cleanup (Figures 2a,2b,3).
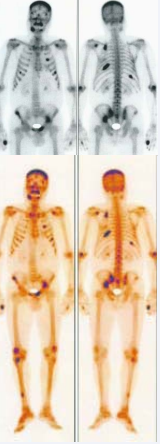
Figure 2 Initial bone scan: multiple hyperactive foci that can be associated with diffuse metastatic calcifications

Figure 3 Bone scan 6 months after surgery a radiological cleanup
The control after one year showed no recurrence with normal serum calcium levels.
DISCUSSION
The causes of primary hyperparathyroidism include parathyroid adenoma (in more than 85% of cases), multigland hyperplasia (in 5% to 10%), and carcinoma (less than 3%). Carcinoma results in severe primary hyperparathyroidism and complications from recurrence and metastatis. However, differentiating carcinoma from benign parathyroid disease is difficult in the preoperative and intraoperative stages, and even after histopathologic evaluation.
Suspicion for malignancy should be high with hypercalcemia greater than 140 mg/L, extremely high serum PTH levels (five times the upper limit of normal), as well as large masses and unilateral vocal cord paralysis [4].
Bone disease appears in 10-20% of patients with primary HPT. Osteoclastoma (also called Brown Tumor, or osteitis fibrosa cystica) consists of a bone cyst in the long bones, ribs, pervis, maxillary mandible, extremities, skull and even the spine
While osteolytic lesions may appear as bone metastases, they can break the cortex, but not generate periostal reaction and do not invade adjacent tissues. Osteoclastomas are considered benign tumors, of the giant cell tumors kind [5].
In order to localize the recurrences or metastatic spread, different modalities of radiological studies can be used. The Sestamibi scan can be very accurate in localizing the local recurrence and lymph node metastasis [6].
It is hard to find characteristics that correlate predictably with the outcome of parathyroid carcinoma, making its prognosis quite variable [7]. Best prognosis seems to be attained with early recognition and complete resection during the initial surgery. A first recurrence occurs on average 3 years after surgery, although there have been reports of 20 years before recurrence [8]. While complete cure becomes unlikely once the tumor has recurred, prolonged survival remains common under these circumstances, with palliative surgery [9]. Five-year survival rates vary from 40- 86% [10].
After parathyroidectomy brown tumors tend to regress. Radiotherapy and chemotherapy are not effective in PTC management.
CONCLUSION
Parathyroid carcinoma is a very rare disease and probably an under diagnosed pathology. The association with brown tumors is common. After parathyroidectomy brown tumors tend to regress. Patients should undergo a lifetime follow up to detect recurrence.








































































































































