Statistics of 4,516 Ingrown Nails Noninvasively Treated. Causes and Treatment Outcomes: Nail Length, Nail Shape and Anchor Taping, Acrylic Affixed Gutter Splint and other Modalities
- 1. Arai Dermatology Clinic, Tokyo, Japan
- 2. YOU Dermatology Clinic, Yokohama, Japan
- 3. Division of Dermatology, FukayaRed Cross Hospital Saitama, Japan
- 4. Department of Dermatology, Juntendo University, Japan
- 5. Department of Dermatology, Inselspital, Switzerland and Dermatol Clinic, Germany
Abstract
Background: The treatment of choice for ingrown nail has been surgical rather than non-surgical.
Objective: To evaluate the statistical data of 4,516 non-invasively treated ingrown nail lesions to validate the benefit of non-invasive treatment methods for ingrown nail, and employ the results in the education of appropriate nail trimming by doctors and patients.
Methods: A total of 4,516 ingrown nails non-invasively treated were observed at Arai Dermatology Clinic (1979-2012). Causes and treatment outcome were analyzed mainly by stage, length and shape of the nail, and non-invasive modalities.
Results: Of the total lesions, the average treatment duration was 32.7 days, 3.9 visits, with a cure rate of 91.8%.The taping method is effective for stage 1 and stage 2, and helpful for stage 3. Acrylic affixed gutter splint is very effective for stage 2 and stage 3. These two treatments can successfully treat ingrown nails without invasive surgery.
Improper nail cutting was found in 88% of the cases. In regards to length and shape of the nails, 39.1% were cut short or extremely short and 59.2% were normal length. Meanwhile, 39.5% were cut with corner-drop-off.
Conclusion: Improper nail cutting is the main cause of ingrown nail and should be avoided.
Not only do the length but also the shape of the nail influence and determine the stage and treatment duration of ingrown nail. Non-invasive treatment using anchor taping and acrylic affixed gutter splint are highly effective in the treatment of ingrown nail and should be viewed as the first treatment.
Keywords
- Ingrown nail
- Gutter splint
- Taping
- Anchor taping
- Sculptured nail
Citation
Arai H, Arai T, Arai K, Kinoshita A, Haneke E (2017) Statistics of 4,516 Ingrown Nails Noninvasively Treated. Causes and Treatment Out- comes: Nail Length, Nail Shape and Anchor Taping, Acrylic Affixed Gutter Splint and other Modalities. J Dermatolog Clin Res 5(2): 1099.
ABBREVIATIONS
ODT: Occlusive Dressing Technique
INTRODUCTION
Ingrown nail is a common nail disorder that causes pain, discomfort and restriction of physical activity. For many years, the treatment of choice for ingrown nail has long been invasive surgical therapy due to the misunderstanding of its pathophysiology. Furthermore, invasive treatments may result in post-operative deformities as well as other unexpected adverse effects. Discussion regarding the controversies of invasive vs. non-invasive treatment is a hot topic [1].
Most cases of ingrown nail can be treated easily and successfully using non-invasive treatments of acrylic affixed gutter splint and the anchor taping method, applied singularly or in combination [2-11], sculptured nail, and other treatments that would prevent a foreign body reaction caused by offending nail edges. It is also worth mentioning that patient education is vital in order to prevent this painful condition and its recurrence worldwide (Figure1-3).

Figure 1

Figure 2: Improper nail cutting.
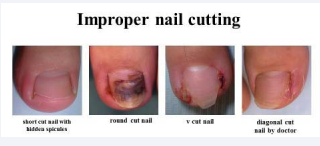
Figure 3: Improper nail cutting.
ETIOLOGY AND PATHOMECHANISM
The etiology of ingrown nail is multifactorial [1], but the primary cause is improper nail cutting [1,11]by patients, caregivers and even doctors [5],as well as small nail trauma, and nail breakages (Figure1,2),[4,5]. Cutting the nail too short, diagonally, round or pointed, can leave behind hidden spicules that offends lateral nail edges, and cause partial nail loss [11] (Figure 2,3,4).
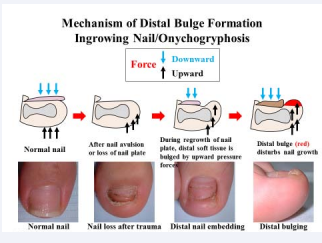
Figure 4: Mechanism of Distal Bulge Formation. Ingrown Nail/ Onychogryphosis.
The irregular nail edges pierce the epidermis of the surrounding soft tissue causing pain, inflammation and granulation tissue due to a chronic foreign body reaction. Furthermore, the nail becomes increasingly macerated and fragile. This results in breakage, where the offending nail edges become loose. Ill-fitting footwear that compressing the distal nail bed against its too-short nail further compounds the problem.
A normal-shaped nail plate of hard keratin exerts counter pressure to the underlying soft tissue while walking (Figure 4) [11,14]. Lack of partial or entire nail plate allows the tip of the toe tissue to be pushed up against at the end of the gait when the entire weight of the body weight plus and the kinetic energy are concentrated on the tip of the big toe. This permits the nail corners or spicules to pierce the tissue, resulting in an ingrowing nail (Figure 4). It also gives rise to the development of a distal nail fold and distal-lateral bulging. Because it lacks no pulp support, it often results in bone changes [12-15] (Figure 4). [11,14] Hypertrophy and hyperkeratosis of the nail folds may occur.
Hypertrophic distal bulging disturbs nail regrowth, leading to distal ingrown nail and onychogryphosis [12-15] (Figure 4).All these events are the results of the vicious cycle of ingrown nails. If the nail is big and long enough, an ingrown nail will not occur because it will support the surrounding soft tissue of the nail tip [13](Figure 5).

Figure 5: Modalities.
TREATMENT
Almost all ingrown nails can be treated non-invasively using the following non-invasive methods (Figure 5). The treatment principle of ingrown nails is to eliminate the cause of ingrown nails, protect the nail fold, and help the regrowth of a normal nail. As it is because the nail plate that grows into the nail fold, the latter has to be protected against the former. This is done by either pulling away the nail fold usingby taping[16] (anchor taping) [2-11], inserting a buffer between them (packing[17]and gutter[18]), or by combining these methods. Such treatments quickly offer reduction of pain, inflammation and granulation tissue, and offers nail fold protection with promising results.
Acrylic affixed sculptured nails and gutter splint act as prosthesis for the lost portion of the nail plate. Other methods used in combination with anchor taping and the gutter splint methods are packing [2,4,9,17] nail ironing,[4,19] plastic nail braces [4,9,20] and shape memory alloy nail wire (super elastic wire [21]) or clips [9,22], occlusive dressing technique [9] with 40%urea paste [23], application of Mohs’ paste for granulation tissue [9,24]and others.
MATERIALS AND METHODS
From a total of 4,561 lesions (in 3,007 patients, ages 2 months-94 years) of ingrowing nails treated non-invasively at Arai Dermatology Clinic, between April 1979 and December 31, 2012, a full follow-up data spanning over 33 years was obtained. The statistical analysis was retrospectively conducted through medical records, clinical photos, questionnaire, and telephone survey of examined patients. The cohort analysis was also performed on treatment modality, nail shape and length, and treatment duration.
RESULTS AND DISCUSSION
Number of patients and lesions
From April 1979 to December, 31 2012, there were a total of 4,516 lesions in 3,007patients with ingrown nail. All cases were treated non-invasively.
Number of patient and lesions by gender
Number of patients: Male:1,028(34.2%), Female:1,979 (65.8%), number of lesions: Male:1,501 (33.2%), Female:3,015 (66.8%). Gender ratioMale 1: Female 2.
A gender comparison shows that lesions in females doubled those of males (Figure 6).
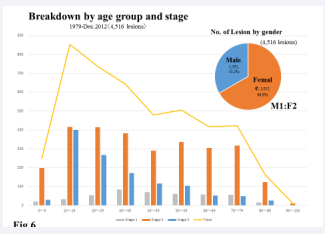
Figure 6: Breakdown by age group and stage , 1979-Dec.2012 (4,516 lesions), No. of Lesion by gender (4,516 lesions)
The number of all patients at Arai Dermatology Clinic reflects the same gender ratio.
Distribution of age group by number of lesion and pathologic stage
In observing the distribution by age and stage among the study population, ingrown nails were seen in all age groups, even in babies and infants (two months) to elderly (94years) (Figure 6). Most cases are seen in ages 10-19, followed by the 20s and 30s age groups. Patients aged 10-39 account for 49.5%, nearly half of all cases. The highly active nature and sports activities of these age groups appear to explain these statistics. Of the total, pediatric cases (15 and under) were 17.4%. The number of ingrown nails increases in older children, and was most frequent in fourteen and fifteen-year olds [11].
Figure (6) also shows the breakdown of pathologic stage (by Heifetz [25])by age group. There are no significant differences in stage 1 levels across all age groups.
Stage 2 sees its highest occurrences in the teens (10-19) and 20s age group, with the 30s groups not far behind, and not much difference from age groups 40 and beyond. However, in stage 3 with granulation tissue, it is worth noting that the largest number of lesions was seen in teens and 20s, followed by 30sgroups. One reason for the high prevalence of stage 3 cases for patients in their teens, especially between the ages of 10-15, may be the higher level of physical activity children undergo at schools [11]. This takes cultural characteristics in Japan into account, where the level of training for school sports is intense while typically lacking an adequate focus on injury prevention and treatment.
Distribution by pathologic stage
The distribution by pathologic stage, according to the classification of Heifetz [25] is presented as the first or acute inflammatory stage: 10.2 (459 lesions), the second or pus- discharging stage: 62.3 (2,815 lesions), and the third or chronic inflammatory and granulation tissue formation stage: 27.2 % (1,227 lesions), and unknown: 0.3% (15 lesions) (Figure 7).
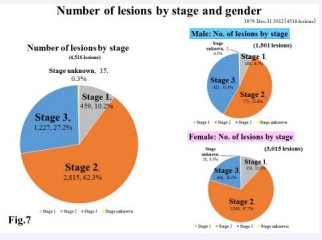
Figure 7: Number of lesions by stage and gender, 1979-Dec.31 2012(4516 lesions), Number of lesions by stage (4,516 lesions), Male: No. of lesions by stage (1,501 lesions), Female: No. of lesions by stage (3,015 lesions)
An overall look at the data shows that about 60% of cases were stage 2, and 30% were stage 3. Few patients sought treatment for stage 1 symptoms, perhaps preferring to take a wait and see approach, or deal with it themselves.
Distribution by stage and gender
A gender and stage comparison shows that for males(1,501 lesions), therewere6.7% (100 lesions) were instage 1, 51.6% (775 lesions) instage 2,41.4% (621 lesions)instage 3, and 0.3% (5 lesions)in stage unknown. For females (3,015 lesions), 11.9% (359 lesions)were in stage 1, 67.7% (2,040 lesions)were in stage 2, 20.1% (606 lesions)were in stage 3 and 0.3% (10 lesions) were of unknown stage.
Over half of the male cases were in stage 2, whilearound40% were in the serious and chronic stage 3 type. For women, stage
- cases accounted for about two thirds of all cases, while stage
- cases made up 1/5 of the lesion. Gender-wise, females showed a tendency to seek treatment during the less advanced stages 1 and 2, while male patients waited until stage 3, when symptoms became severe(Figure 8).
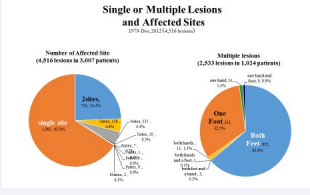
Figure 8: Single or Multiple Lesions and Affected Sites 1979- Dec.2012(4,516 lesions), Number of Affected Site (4,516 lesions in 3,007 patients), Multiple lesions (2,533 lesions in 1,024 patients)
Single or multiple lesions and affected sites
Ingrown nails with single lesions accounted for 65.9% (1,983 lesions in 3,007patients), while patients with multiple lesions of two or more accounted for 34.1% (2,533lesions in 1,024 patients):About2/3 of the patients were single lesion cases, with the remaining 1/3possessing tendencies for multiple lesions.
When looking at patients with several lesions, they were found on both feet in 64% of the patients, and found in one foot in 32.5%, 0.3% displayed lesions in both feet and one hand, 1.3% in both hands, 0.1% in both hands and one foot, and0.9% in one foot and one hand (Figure 9).
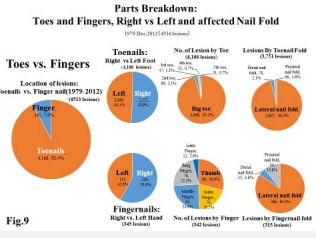
Figure 9: Parts Breakdown: Toes and Fingers, Right vs Left and affected Nail Fold 1979-Dec.2012 (4516 lesions), Toes vs. Fingers Location of lesions: Toenails vs. Finger nail (1979-2012)(4513 lesions), Toenails: Right vs Left Foot (4,168 lesions), No. of Lesion by Toe (4,166 lesions), Lesions by Toenail Fold (3,751 lesions), Fingernails: Right vs. Left Hand (345 lesions), No. of Lesions by Finger (342 lesions), Lesions by Fingernail fold (315 lesions)
Lesion occurrence: Toenails vs. Fingernails
Toe or finger, which nail fold (Toes vs. hands) From the total of 4,513 lesions observed, the vast majority, 92.4 (4,168 lesions) occurred on the toenails (feet), and only7.6 (345 lesions) on the fingernails (hands).
Toenail lesions
Of the 4,168 lesions on the feet, the right vs. left ratio for toenails was nearly the same.
Out of these 3,007 patients, there were 21.7 (654patients) with concurrent lesions on both feet. As for the part breakdown lesion count by toe, of the 4,166 total, the majority of the lesions 95.2%(3,968) occurred on the big toe. Regarding the nail fold affected, of the 3,751 total lesions on the foot, the vast majority (96.2%, 3,607 lesions) occurred on the lateral nail fold, followed by the distal nail fold (2.1%,78 lesions)and on the proximal nail fold or retronychia [26] (1.8%,66lesions)(Figure 9).
Fingernail lesions
With regard to 345lesions on fingernails, the right vs. left ratio for fingernails slightly favored the right hand. Only 1.3% (13patients) had concurrent cases on both hands.
As for the part breakdown lesion count by fingers, the thumb saw most lesions at 28.9% (99), but there was no large difference among the index finger, middle finger, and ring finger.
The little finger had the fewest lesions. In regard to which nail fold was affected, of the 315 total lesions on the fingers, 84.4% or 266 lesions occurred on the lateral nail fold, followed by the distal nail fold (4.8%, 15 lesions) and on the proximal nail fold or retronychia [26] (10.8%, 34 lesions) (Figure 9).
Number of lesions combined with over-curved or pincer nail
Over-curved or pincer nail (Figure 10)
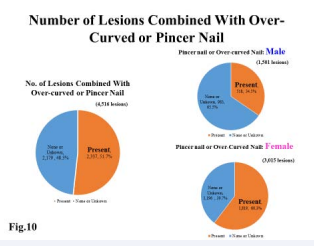
Figure 10: Number of Lesions Combined With Over-Curved or Pincer Nail, No. of Lesions Combined with Over-curved or Pincer Nail (4,516 lesions), Pincer nail or Over-curved Nail: Male (1,501 lesions), Pincer nail or Over-Curved Nail: Female (3,015 lesions)
From the total of 4,516 lesions, concerning curvature of nail plate, around half of all the lesions observed (51.7%, 2,337 lesions) exhibited some type of nail curvature or folding such as over-curved or pincer nails, involved (omega or trumpet) nails, or the in-bent or folded staple type. Gender-wise, with 60.3% or1,819 lesions, females showed a tendency to have more over-curved or pincer nails, while males accounted for 34.5%,518lesions. Women had about double the number of men.
THE CAUSE AND MECHANISM OF INGROWN NAIL
Ingrown nail is multifactorial, however, its main causes are improper nail cutting and nail breakage or nail trauma, compounded by ill-fitting footwear and others (Figure 11).
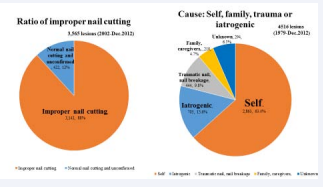
Figure 11: Ratio of improper nail cutting 3,565 lesions (2002- Dec.2012), Cause: Self, family, trauma or iatrogenic 4516 lesions (1979-Dec.2012)
Who cut the nails or whether they were due to natural trauma(Figure 11).
Of the total 4,516 lesions examined, we found that 63.4% (2,863lesions) had cut their own nails and 4.7% (210 lesions) by family or care givers. 9.8percent (444 lesions) were due to broken nails and external injuries. Iatrogenic nail cutting or post- operative deformity was seen in about 15.6% (705 lesions).
9.1.1. Iatrogenic causes: Among these 705 lesions (15.6%) that were thought to have been iatrogenic, there were 455 lesions of iatrogenic nail cutting, and nail avulsion accounted for 33 lesions. There were166 lesions due to post-operative deformation and 51 lesions where phenolization was used. In regarding to the stage, iatrogenic cases were found in 25.6% (309/1,227 lesions) in Stage 3, 12.8% (357/2,815 lesions) in Stage2 and 8.6% (39/459 lesions) in stage1.
Improper nail cutting
With regards to nail cutting, the total lesions (3,565, 2002- 2012)(investigation was based on photographs taken at the clinic),the vast majority of lesions (88.2% or 3,143 lesions) had improper nail cuttings, length or shape.
Regarding nail cutting, nail length/nail shape and stage (Figure12,13).
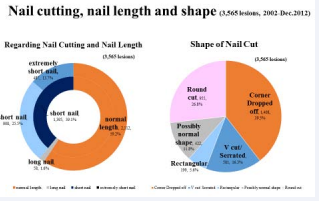
Figure 12: Nail cutting, nail length and shape (3,565 lesions, 2002- Dec.2012), Regarding Nail Cutting and Nail Length(3,565 lesions), Shape of Nail Cut (3,565 lesions)
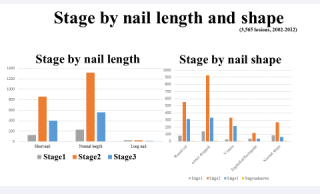
Figure 13: Stage by nail length and shape (3,565 lesions, 2002-2012) Stage by nail length, Stage by nail shape
Nail length and stage: The nail length was measured at the longest part of the nail plate. Short and extremely short nails accounted for about 40 % of the lesions (39.1% or 1,395 lesions), while 60% (59.2% or 2,112 lesions) had normal nail length. We can see that a large number of ingrown nails occurred on nails of cut,” were seen the most often, seen with around 39.5% (1,408 lesions).The next most frequently seen cut was the “round cut,” with 26.8% (955 lesions), “V cut,” or nails cut either at sharp diagonal angles, in a stair-like, or serrated fashion, accounting made up for 16.3% (581 lesions), while those cut into a vertically rectangular shape accounted for 5.6% (199 lesions). Normal shaped nail accounted for 11.8% (422 lesions).
The relationship between nail cut (nail length and shape) and stage of ingrown nail, treatment duration, and prognosis is listed in Table (3,4).
Table 3: Treatment duration, visits and cure rate (3,565 lesions, 2002-2012), Treatment outcome: Nail length.
|
|
|
|
Total lesions |
|
|
|
Stage1 |
|
|
|
Stage2 |
|
|
|
Stage3 |
|
|
|
Nail length |
No. of Cases |
Ratio |
Treat- ment dura- tion |
Visits |
Cure rate |
No. of Cases |
Treat- ment dura- tion |
Visits |
Cure rate |
No. of Cases |
Treat- ment dura- tion |
Visits |
Cure rate |
No. of Cases |
Treat- ment dura- tion |
Visits |
Cure rate |
|
extremely short nail |
487 |
13.7% |
35.3 |
4.1 |
88.9% |
31 |
15.5 |
2.2 |
77.4% |
287 |
27.1 |
3.2 |
88.5% |
167 |
52.6 |
5.9 |
91.6% |
|
short nail |
908 |
25.5% |
29.2 |
3.6 |
90.5% |
97 |
16.0 |
2.0 |
86.6% |
575 |
26.1 |
3.4 |
92.7% |
232 |
42.8 |
4.9 |
86.6% |
|
normal length |
2,112 |
59.2% |
31.3 |
3.9 |
90.0% |
229 |
17.9 |
2.5 |
80.4% |
1,315 |
25.2 |
3.2 |
91.6% |
560 |
51.1 |
6.2 |
90.2% |
|
long nail |
58 |
1.6% |
24.3 |
3.3 |
87.9% |
23 |
17.8 |
2.9 |
87.0% |
25 |
27.3 |
3.1 |
84.0% |
10 |
31.6 |
4.4 |
100.0% |
|
Total |
3,565 |
100.0% |
31.2 |
3.9 |
90.0% |
380 |
17.2 |
2.4 |
82.1% |
2,202 |
25.7 |
3.3 |
91.4% |
969 |
49.2 |
5.8 |
89.7% |
Table 4: Treatment duration, visits and cure rate (3,565 lesions, 2002-2012), Treatment outcomes: Nail shape.
|
|
|
|
Total lesions |
|
|
|
Stage1 |
|
|
|
Stage2 |
|
|
|
Stage3 |
|
|
|
Nail shape |
No. of Cases |
Ratio |
Treatment duration |
Visits |
Cure rate |
No. of Cases |
Treatment duration |
Visits |
Cure rate |
No. of Cases |
Treatment duration |
Visits |
Cure rate |
No. of Cases |
Treatment duration |
Visits |
Cure rate |
|
Round cut |
955 |
26.8% |
29.1 |
3.7 |
90.6% |
82 |
13.1 |
1.9 |
79.3% |
554 |
24.5 |
3.2 |
92.4% |
317 |
41.5 |
5.0 |
90.2% |
|
Corner cut |
1,408 |
39.5% |
30.9 |
3.8 |
90.2% |
144 |
15.0 |
2.2 |
80.6% |
929 |
25.1 |
3.3 |
92.4% |
333 |
53.7 |
6.2 |
88.3% |
|
V cut/ Serrated |
581 |
16.3% |
37.2 |
4.4 |
91.1% |
31 |
21.8 |
2.7 |
74.2% |
332 |
26.6 |
3.2 |
92.5% |
216 |
55.2 |
6.5 |
91.2% |
|
Rectangular |
199 |
5.6% |
33.2 |
3.8 |
88.4% |
39 |
19.6 |
2.7 |
87.2% |
120 |
27.8 |
3.2 |
88.3% |
40 |
62.9 |
6.6 |
90.0% |
|
Possibly normal |
422 |
11.8% |
27.6 |
3.5 |
87.0% |
84 |
22.1 |
2.8 |
88.1% |
267 |
28.2 |
3.4 |
86.1% |
63 |
34.5 |
4.9 |
88.9% |
|
Total |
3,565 |
100.0% |
31.2 |
3.9 |
90.0% |
380 |
17.2 |
2.4 |
82.1% |
2,202 |
25.7 |
3.3 |
91.4% |
969 |
49.2 |
5.8 |
89.7% |
TREATMENT PROGNOSIS
Prognosis / Cure rate by stage:
Of the total of 4516 lesions, regarding the prognosis following conservative treatment of ingrown nails in average, 91.1% (4,114 lesions) were cured, 1.8% (81 lesions) experienced improvement, and 7.1% (321 lesions) were classified as unknown. There were 282 recurrent lesions (6.2%).
Treatment outcome
Treatment duration visits and cure rate (Table 1): Of the 4,516 lesions treated, the average treatment duration of all lesions was 32.7 days, 3.9 visits with a 91.8% cure rate. In stage 1, the average treatment duration was 16.5 days, 2.3 visits, with an 83.7% cure rate. In stage 2, it was 27.5days, 3.3 visits with a 92.5% cure rate. In stage 3, the average treatment duration was 50.7 days, 5.7 visits with a 90.7% cure rate. Cure rate is about the same in stages 2 and 3. Some cases were lost in stage 1 due to patients not returning to the clinic (Table 1).
Table 1: Table 5: No. of lesions per nail shape and length in Stage 2. (1,365 lesions).
|
Stage |
|
Total cases |
|
|
|
|
No. of Lesion |
Treatment Duration (Days) |
Visits (Number) |
Cure Rate |
|
Stage 1 |
459 |
16.5 |
2.3 |
83.7% |
|
Stage 2 |
2,815 |
27.5 |
3.3 |
92.5% |
|
Stage 3 |
1,227 |
50.7 |
5.7 |
90.7% |
|
unknown |
15 |
25.4 |
3.1 |
93.3% |
|
Total |
4,516 |
32.7 |
3.9 |
91.8% |
|
Stage, nail shape and length: Big toe |
||||
Comparison of treatment outcomes by various non- invasive modalities (Table 2): Breakdown of non-invasive modalities used is shown in Figure (14).Distribution by stage and treatment modalities are shown in Table (2).
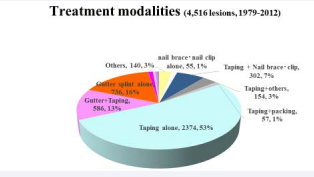
Figure 14: Treatment modalities (4,516 lesions, 1979-2012).
Table 2: Treatment duration, visits and cure rate (4,516 lesions), Treatment outcome:
|
|
|
|
Total cases |
|
|
|
Stage1 |
|
|
|
Stage2 |
|
|
|
Stage3 |
|
|
|
Modalities |
No. of le- sion |
Ratio |
Treat- ment dura- tion (days) |
visits (num- ber) |
Cure rate |
No. of le- sion |
Treat- ment dura- tion- days) |
visits (num- ber) |
Cure rate |
No. of le- sion |
Treat- ment dura- tion (days) |
visits (num- ber) |
Cure rate |
No. of lesion |
Treat- ment dura- tion (days) |
visits (num- ber) |
Cure rate |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
(days) |
|
|
|
Total cases |
4,516 |
|
32.7 |
3.9 |
91.8% |
459 |
16.5 |
2.3 |
83.7% |
2,815 |
27.5 |
3.3 |
92.5% |
1,227 |
50.7 |
5.7 |
90.7% |
|
Taping +sculp- tured nail |
30 |
0.7% |
34.4 |
4.3 |
100.0% |
4 |
74.0 |
9.0 |
100.0% |
19 |
26.6 |
3.4 |
100.0% |
7 |
33.0 |
4.2 |
100.0% |
|
sculptured nail alone |
22 |
0.5% |
47.6 |
3.1 |
95.5% |
1 |
49.0 |
4.0 |
100.0% |
18 |
45.4 |
2.9 |
94.4% |
3 |
60.3 |
3.7 |
100.0% |
|
Gutter + sculp- tured nail |
51 |
1.1% |
65.4 |
5.2 |
98.0% |
0 |
0.0 |
0.0 |
0.0% |
25 |
47.6 |
4.0 |
96.0% |
26 |
82.4 |
6.4 |
100.0% |
|
Gutter splint alone |
736 |
16.3% |
47 |
5.1 |
95.4% |
6 |
7.5 |
1.7 |
100.0% |
406 |
39.4 |
4.6 |
98.0% |
321 |
57.7 |
5.8 |
91.9% |
|
Gutter+Taping |
586 |
13.0% |
63.9 |
7.3 |
92.3% |
0 |
0.0 |
0.0 |
0.0% |
141 |
49.1 |
5.6 |
95.0% |
443 |
68.6 |
7.9 |
91.4% |
|
Taping alone |
2,374 |
52.6% |
21.5 |
2.8 |
89.8% |
274 |
12.9 |
1.9 |
81.4% |
1,716 |
22.3 |
2.9 |
90.5% |
377 |
24.7 |
3.3 |
88.9% |
|
Taping+packing |
57 |
1.3% |
27.6 |
3.4 |
97.0% |
8 |
24.5 |
2.9 |
100.0% |
49 |
28.1 |
3.4 |
96.9% |
0 |
0.0 |
0.0 |
0.0% |
|
Taping+others |
154 |
3.4% |
23.2 |
3.1 |
91.6% |
31 |
16.5 |
2.4 |
77.4% |
103 |
23.1 |
3.0 |
94.2% |
19 |
34.8 |
5.0 |
100.0% |
|
Taping + Nail brace clip |
302 |
6.7% |
29.1 |
3.4 |
93.4% |
76 |
22.3 |
2.9 |
85.5% |
210 |
30.8 |
3.6 |
95.7% |
14 |
40.6 |
4.2 |
100.0% |
|
nail brace nail clip alone |
55 |
1.2% |
37.4 |
3.6 |
89.1% |
30 |
32.5 |
3.1 |
90.0% |
24 |
43.9 |
4.3 |
87.5% |
1 |
30.0 |
3.0 |
100.0% |
|
Others |
140 |
3.1% |
19.4 |
2.4 |
88.6% |
28 |
9.5 |
1.7 |
96.4% |
98 |
23.8 |
2.6 |
90.8% |
14 |
8.9 |
1.9 |
57.1% |
|
Unknown, others |
9 |
0.2% |
3.6 |
1.2 |
22.2% |
1 |
1.0 |
1.0 |
0.0% |
6 |
5.3 |
1.3 |
33.3% |
2 |
1.0 |
1.0 |
0.0% |
All lesions were treated with non-invasive modalities mainly using taping and gutter splint singularly or in combination. Furthermore, various combinations of other treatments as described below were flexibly performed depending on the condition, and their outcomes are compared and discussed by stage. Table (2) shows the treatment results by each non-invasive treatment modality observed as well as the comparison of the treatment outcomes.
Treatment modalities used were mainly anchor taping and acrylic affixed gutter splint. Other modalities include sculptured nail, packing, nail braces, nail clips, nail ironing, ODT with 40% urea paste, Mohs’ paste, antibiotics, steroids, and others combinations thereof (Figure 15).
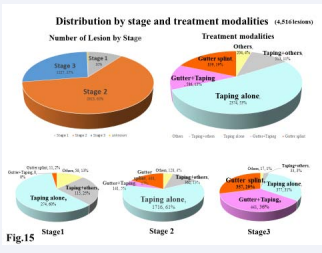
Figure 15: Distribution by stage and treatment modalities (4,516 lesions).
Number of Lesion by Stage Treatment modalities
Stage1
Stage2
Stage3
Distribution of pathologic stage and comparison of treatment modalities by stage: Precise data of treatment outcome of each modality is presented in Table (2).
In (Figure15), the 2 top pie charts show the distribution of lesions by stage and the treatment methods used. The bottom charts are the treatment methods used in each lesion stage. We can see here that: In stage 1, many cases can be treated with taping alone. In stage 2, taping is the main treatment method, but conditions improve faster when combined with the gutter splint treatment. In stage 3, it is better to use gutter splint as the main treatment method, and supplement with taping. Taping can be used with severe inflammations and hypertrophy of the nail fold, and can be extremely helpful.
Comparison of nail length and shape, and treatment outcome: Treatment outcome: Treatment duration, visits and cure rate by nail length and nail shape and pathologic stage are presented in Table (3,4).
Treatment outcome: Nail length,Treatment duration, Visits and Cure rate(3,565lesions)(Table 3).
In average, the treatment duration was 31.2days, with 3.9visits and 90.0% cure rate.
Extremely short nails required, 35.3days, 4.11 visits, 88.9% cure rate. Short nails showed 29.2 days, 3.6 visits, 90.5%cure rate. Normal length nail showed 31.3 days, 3.9visits with 90.0% cure rate. Long nail showed 24.3 days, 3.3 visits and 87.9% cure rate.
Among nails of all lengths, not much difference was seen in the treatment duration or number of visits in stage 1 and 2. Extremely short nails required 10 days longer than long nails in average and required 21days longer than long nail in stage 3.
Treatment outcome: Nail shape, treatment duration, visits, and cure rate (Table 4).
With regards to nail shape, nails with lacking corners were most frequently observed (approx. 40%). The treatment duration was longest in V-cut and serrated nails (37.2 days) followed by nails with corners cut-off in a rectangular shape (rectangular cut) (33.2 days). Treatment duration for normal nails was 27.6 days. This suggests a correlation to the length of the nail loss.
In stage 1 and 2 there was no significant difference in the nail shape. In stage 3, rectangular cut required the longest treatment duration (62.9 days and 6.6 visits), 13.7 days or around two weeks more than average and 28.4 days or around four weeks more than normal shaped nail.
RECURRENT CASES
From the total of 4,516 lesions, when looking at the nails of the 282 recurrent lesions (6.2%), around half maintained a normal length, with the remaining half having extremely short or short nails. Treatment duration for these patients was the same as their previous nail lesions, as they had not improved their nail shape or length.
IN TERMS OF FAMILY TENDENCIES
Among the 3,007 patients, 22 patients were a part of a total of 10 families. Combinations were parent and child or siblings. This shows that ingrown nail is not hereditary, but rather, issues related to nail cutting and/or failing to change their nail cutting habits and footwear.
COHORT ANALYSIS FOR INGROWN NAIL DATA
Cohort analysis for ingrown nail data was performed after cleaning the data for standardization. Analysis focused on only adult-onset cases, lesions of the lateral nail folds of big toes, and stage2 and stage3 cases (Table 5,6).
Table 5 No.of lesions per nail shape and length in stage2.(1,365 lesions), Stage, nail shape and length: Big toe.
|
|
Extremely short |
Short |
Long |
Normal |
Total |
|
Corner cut |
54 |
167 |
19 |
498 |
738 |
|
Round cut |
84 |
115 |
1 |
71 |
271 |
|
Angle, diagonal, rectangular, serrated, spear |
16 |
49 |
2 |
215 |
282 |
|
Straight across |
26 |
10 |
24 |
14 |
74 |
|
Total |
180 |
341 |
46 |
798 |
1365 |
Table 6: No.of lesions per nail shape and length in stage3.(570 lesions), Stage, nail shape and length: Big toe
|
|
Extremely short |
Short |
Long |
Normal |
Total |
|
Corner cut |
25 |
56 |
7 |
123 |
211 |
|
Round cut |
34 |
44 |
0 |
38 |
116 |
|
Angle, diagonal, rectangular, serrated, spear |
18 |
49 |
4 |
143 |
213 |
|
Straight across |
11 |
14 |
4 |
1 |
30 |
|
Total |
88 |
163 |
15 |
304 |
570 |
The treatment modality and treatment duration, nail cutting and nail shape and length were analyzed. Hazard rate here means short treatment duration until the nail is cured. A hazard rate greater than 1, means the ingrown nail will heal in a short period. A hazard rate less than 1, means longer treatment duration will be needed.
Nail length and shape
(Table 7)
Results: Shape of Nail plate and length
Table 7: Hazard rate of Shape of Nail plate and length
|
|
Hazard Rate |
95%CI lower |
95%CI Upper |
P - value |
|
|
Corner dropped off, Normal |
Pivot |
|
|
|
|
|
Corner dropped off, Ext, Short |
0.7445 |
0.6591 |
0.841 |
0.0155 |
* |
|
Corner dropped off, Short |
0.9964 |
0.9184 |
1.081 |
0.9649 |
|
|
Corner dropped off, Long |
1.3098 |
1.07 |
1.6035 |
0.1821 |
|
|
Round, Normal |
0.8329 |
0.7464 |
0.9294 |
0.0952 |
. |
|
Round, Ext, Short |
0.8298 |
0.5473 |
1.2581 |
0.1149 |
|
|
Round, Short |
0.7616 |
0.5405 |
1.0733 |
0.5721 |
|
|
Round, Long |
1.5593 |
0.4079 |
5.9615 |
0.7285 |
|
|
V cut, Normal |
0.9519 |
0.8825 |
1.0268 |
0.5149 |
|
|
V cut, Ext, Short |
0.9906 |
0.6516 |
1.5059 |
0.1301 |
|
|
V cut, Short |
0.9809 |
0.7282 |
1.3212 |
0.811 |
|
|
V cut, Long |
1.0686 |
0.4699 |
2.43 |
0.7766 |
|
|
Horizontal, Normal |
1.7402 |
1.3347 |
2.2689 |
0.0368 |
* |
|
Horizontal, Ext, Short |
1.0303 |
0.5018 |
2.1153 |
0.4903 |
|
|
Horizontal, Short |
0.9952 |
0.4962 |
1.9961 |
0.1119 |
|
|
Horizontal, Long |
0.5132 |
0.2192 |
1.2012 |
0.0001 |
*** |
|
*Hazard rate > 1 means ingrown nail will heal in a short period. |
|||||
|
*Hazard rate <1 : longer treatment duration will be needed. |
|||||
For any shape, cases of longer nail length tend to cure sooner.
Normal shaped nails with sufficient length tend to heal sooner, and in contrast, short nails with partial nail loss take longer to heal (Table 8).
Table 8: Hazard rate of Causes
|
|
Hazard Rate |
95%CI lower |
95%CI Upper |
P - value |
|
Cause: Self (Pivot) |
Pivot |
|
|
|
|
Iatrogenic |
0.9066 |
0.8497 |
0.9673 |
0.1304 |
|
Family |
1.0785 |
0.7508 |
1.5492 |
0.8348 |
|
Nail breakage/External trauma |
0.8525 |
0.7764 |
0.9361 |
0.0879 |
|
*Hazard rate < 1: longer treatment duration will be needed. |
|
|
|
|
Concerning the Results: Cause
Though there are no significant differences, cases of ingrown nail caused by traumatic nail/nail breakage tend to cure slower than others. While it does not seem as significant through this analysis, there is a tendency that nails cut drastically by doctors, or iatrogenic nail cutting, and nail trauma take longer to heal.
Modalities (Table 9)
Results: Treatment Methods
Table 9 Hazard rate of treatment methods
|
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
In treatment modalities, the hazard rate is higher for taping and the combination with taping compared to other treatment methods, and it significantly effects treatment duration. The hazard rate is lower for sculptured nails, and cases treated with it tend to be slow to cure. This is because sculptured nails were applied only to large nail loss, thus requiring a longer treatment period.
SUMMARY
Statistics
The total number of ingrown nails observed at Arai Dermatology Clinic (1979 – 2012) was 4,516 lesions in 3,007 patients, of which 786 lesions were pediatric cases (17.4%). Of the total, 92.4% occurred in toes and 7.6% occurred in fingernails. Of the ingrown toenail cases 95.2% occurred in the big toe, in which the vast majority (96.2%) concerned the lateral nail fold, followed by distal nail embedding (2.1%) and proximal nail fold or retronychia (1.8%). The highest numbers of cases are seen in ages 10-19, followed by the 20s and 30s age groups and especially in stage 3 with granulation tissue the same tendency was observed.
Treatment outcome was observed by stages of disease and treatment methods. Of all the 4,516 lesions, the average treatment duration was 32.7 days, 3.9 visits, with a cure rate of 91.8%.Of the cases that were treated mostly with taping (52.6%, 2,374 lesions), the average treatment duration was 21.5 days,
2.8 visits, with a cure rate of 89.2%. In cases treated mostly with gutter splint method (16.3%, 736 lesions), the average treatment duration was 47.0 days, 5.1 visits, with a cure rate of 95.4%. Of the total of 4,516 lesions, there were 228 recurrent lesions (6.2%).
Regarding the length and shape of the nails, of the 3,565lesions with descriptions, of the total of 1,395 lesions described39.1% were cut short or extremely short and 59.2%were cut normally. Meanwhile, in regards to the nail shape, 39.5%were corner dropped off cut, 26.8%were round-cut,16.3% were in an angle/ steps/blade/V shape cut, 5.6% were longitudinal/rectangular cut, and11.8% were possibly normal shape. The nails in most cases (88.2%) were cut in problematic ways. Of all 4,516 lesions, nails were cut or injured by self (63.4%), by family or caregivers (4.7%), by doctors (15.6%) and by nail breakage and nail trauma (9.8%).
Cohort analysis also found that for any shapes, cases of longer length tend to cure sooner. Normal shaped nails with sufficient length tends to heal sooner, and in contrast, short nails with partial nail loss take longer to heal.
Through the experiences and statistics of ingrown nail treatment over the past 33years, we learned that ingrown nail can be successfully treated with non-invasive methods. Anchor taping method is effective for stage 1 and stage 2 ingrown nails, and is also helpful for stage 3 combined with the acrylic affixed gutter splint.The acrylic affixed gutter splint is very effective for stage 2 and stage 3.
These two treatments can successfully treat ingrown nails without having to conduct invasive surgery.
DISCUSSION
We have observed that ingrown nail is a common and painful nail disorder in all ages that restricts physical and social activity.
Ingrown nails are simple mechanical and physical nail disorder caused either naturally (nail breakage, nail trauma) or artificially (improper nail cutting - too short or too deep).
The causes and pathophysiology are described above.
In our investigation, ingrown nail was most often seenin normal length nails (in around 60%) and in nails where corners are dropped off(in around 40%).The shape of how the nails are cut determines the onset of ingrown nails. However, short nails or extremely short nails determine treatment duration. In terms of treatment duration and number of treatments, data suggests that the shape and amount of the nail loss (cut diagonally, rectangular or v-cut) and length of the nail loss are involved.
For any shapes, cases of longer length tend to cure sooner. Normal shaped nails with sufficient length tend to heal sooner, and in contrast, short nails with partial nail loss take longer to heal.
With these facts in mind, we should remind ourselves of the crucial role of mechanoreceptors in ingrown nails and over- curved nail and the reason why the nails have to be cut properly.
Relationship between mechanoreceptor in thebig toe and ingrown nail caused by improper nail cutting
Numerous mechanoreceptors exist in the skin of the sole of the foot, such as Meissner corpuscles and Pacinian corpuscle end- organs, and are especially concentrated on the big toe [27-29].
Mechanoreceptor is an inclusive term describing receptor organs, where once a mechanical stimulus is received, triggers the onset of afferent impulses. It involves sensations such as touch, pressure, stretching, vibration, gravity, equilibrium, temperature, and others.
The mechanoreceptors on the sole of the foot are instrumental in coordinating sense and motion, to control one’s posture in an upright position, balance, and exercise [27-29]. This is done when mechanoreceptors accumulate pressure information from the ground in contact and transmit cutaneous afferent impulses, which are then integrated and organized in the central nervous system. Furthermore, the big toe has the highest sensitivity on the sole of the foot [27-29].The nail apparatus is an important site that should not be damaged, thus a non-invasive treatment is desired.
The nail plate has a natural curve along the toe and fingers, and in the case of the toe, the tread when walking creates a reactive force (floor reaction force) that maintains a natural curve as if by ironing from the sole as well as pressure from above, a downward pressure of body weight and force. When an individual stop to tread, such as when they no longer want to or are able to tread, are in a wheelchair, or suffer from paralytic diseases, the nail plate gradually or rapidly increases its curvature.
When the nail is cut too short, especially when the nail corner is cut off or rounded, the mechanoreceptor for pain or wounding immediately and unconsciously reacts when taking a step. In response, one does not step strongly, creating a smaller floor reaction force, and starts an onset of ingrown nail and over- curving of the nail plate.
When the curvature increases due to factors described above, the nail causes pressure on the skin when walking, causing mechanoreceptors to feel pain or pressure. As a result, one unconsciously takes restrained, light steps (not stepping too strongly), creating less floor reaction force, increasing curvature, and developing over-curved nail and ingrown nail.
Therefore, it is important that the size of the nail plate, the continuity between the nail plate and nail fold, the configuration of nail apparatus (nail unit, nail apparatus) and toes are normal and healthy. This includes avoiding treatments that are damaging to the nail plate and nail apparatus.
Concerning the treatment, data has shown that the treatment of choice for ingrown nail in every stage is conservative therapy, using the anchor taping and acrylic affixed gutter splint methods, singularly or in combination.
With conservative treatment methods, the size and width of the nail plate are maintained. The nail cures naturally without deformation. It is able to return to its original state without inflammation. Conservative treatment methods are outstanding from physiological, functional and aesthetical point of view. Furthermore, these methods are inexpensive, making them especially attractive for poorer countries.
On the other hand, removal of spicules or nail plate, nail avulsion and wedge-shaped excision as treatment are a kind of artificial injuries. Other treatments that destruct the nail matrix (such as phenol, other chemicals and laser) and remove nail folds make the nail plate narrow, adversely affecting the ability of the nail to support body weight [8,15]. In addition, because the lateral nail fold and the nail edge are no longer connected, the nail plate cannot support the pressure of the body weight and walking motion applied to the big toe [15].
In our data, of the total 4,516 lesions examined, 705 lesions (15.6%) that were thought to have been iatrogenic. In regard to the stage, iatrogenic cases were found in 25.6% in Stage 3, 12.8% in Stage 2 and 8.6% in stage 1. We doctors should be responsible about our patients and our treatment results.
Ingrown toenail surgery carries a significant recurrence and
re-operation rate [30]. Of a total of 880 procedures performed on 414 patients (median age 8.5), almost half (48%) of the children underwent two or more procedures. The high recurrence rates and their expected cosmetic end results are important details influencing patients and patients’ parents to discuss surgical options prior to treatment.
The outcomes and long term prognosis of invasive surgeries of ingrown nail depend on the techniques of doctors.
Although the short-term outcomes of surgery are positive, the long-term results of recurrent ingrown nailsmay create multiple problems for children and adults at a time when restricting their movement is not only inconvenient, but harmful for their growing bodies.
CONCLUSION
When looking from this perspective, we can see that we must take great care when cutting nails, educate children and adults on proper nail cutting and care, and should discourage iatrogenic nail cutting to prevent the occurrence and recurrence of ingrown nail, over-curved nail and pincer nail. A well-designed conservative treatment based on proper understanding of the anatomy, the cause, pathophysiology and mechanism of the disease, is necessary to attain success in promoting complete remission.
ACKNOWLEDGEMENT
We would like to acknowledge and at the same time personally thank the co-operation given by our patients, staff members, family and friends in the creation of this publication.
REFERENCES
- Haneke E. Controversies in the treatment of ingrown nails. Dermatol Res Practice. 2012; 1-12.
- Arai H, Arai T, Nakajima H. Conservative outpatient treatment of ingrowing nail - Gutter treatment combined with the application of acrylic resin for sculptured nail and sculptured artificial nail. Hifubyoh-Shinryoh. 1999; 21: 1159-1166.
- Arai H, Arai T, Nakajima H, Haneke E. Simple and highly effective treatment for ingrowing nail – Gutter treatment with acrylic fixation, acrylic artificial nail and taping. Jap J Clin Dermatol. 2002; 71: 31-35.
- Arai H, Arai T, Nakajima H, Haneke E. Improved conservative treatment of ingrowing nail-acrylic affixed gutter treatment, sculptured nail, taping, antibiotic impregnated gauze packing, plastic nail brace, and nail ironing. Rinsho Hifuka. 2003; 57: 110-119.
- Arai H, Arai T, Nakajima H, Haneke E. Formable acrylic treatment for ingrowing nail with gutter splint and sculptured nail. Int J Dermatol. 2004; 43: 759-765.
- Arai H, Arai T, Nakajima H, Haneke E. Treatment of ingrowing nail in children, acrylic affixed gutter splint, sculptured nail and taping. J Pediat Dermatol. 2004; 23: 67-72.
- Arai H, Arai T. Anchor taping for ingrown nail. J Jpn Hair Sci Assoc. 2008; 40: 72-77.
- Arai H, Arai T. We recommend conservative treatment methods for ingrown nails. Stop invasive surgery now!. J Visual Dermatol. 2008; 7: 1052-1054.
- Arai H, Arai T, Haneke E. Simple and effective non-invasive treatment methods for ingrown nail and pincer nail including acrylic affixed gutter splint, anchor taping, sculptured nails, shape memory alloy and plastic nail braces as well as 40% urea paste. J Kochi Med Ass. 2011; 16: 37-56.
- Arai H, Arai T, Haneke E. Anchor taping method for the treatment of ingrown nail, nail trauma and other nail disorders. Jap J Clin Dermatol. 2012; 29: 007-0013.
- Arai H, Haneke E. Noninvasive treatment for ingrown nail: Anchor taping, Acrylic Affixed Gutter Splint, Sculptured Nail, and Others. Pediatric Nail Disorders Edited by Robert Baran, Smail Hadj-Rabia, Robert Silverman. 2016, P253-274, CRC Press Taylor & Francis Group Boca Raton London New York.
- Fowler AW. Excision of the germinal matrix: a unified treatment for embedded toe-nail and onychogryphosis. Br J Surg. 1958; 45: 382- 387.
- Higashi N, Matsumura T. The etiology of onychogryphosis of the great toenail and of ingrowing nail. Skin Res. 1988; 30: 620-625.
- Higashi N, Kume A, Ueda K. Treatment of nail deformity with sculptured nail. Skin Res. 1996; 38: 296-300.
- Higashi N. Ingrown nail plate. MB Derma. 2003; 81: 188-194.
- Nishioka K, Katayama I, Kobayashi Y, Takijiri C, Nishioka K. Taping for embedded toenails. Br J Dermatol. 1985; 113: 246-247.
- Nakajima A. Non-invasive treatment for ingrown nail. Rinsho derma (Tokyo). 1977; 19: 153.
- Wallace W, Milne DD, Andrew T. Gutter treatment for ingrowing toenails. Br Med J. 1979; 21: 168-171.
- Narita H. Radical operation of pincer nail. Rinsho Hifuka. 2001; 55: 154-159.
- Effendy I, Ossowski B, Happle R. Zangennagel. Konservative Korrektur durch Aufkleben einer Kunststoffspange. Hautarzt. 1993; 44: 800-802.
- Egawa M. Treatment of ingrowing toenails using a super elastic wire. J Osaka Med Ass. 2001; 35: 76-78.
- Ishibashi M, Tabata N, Suetake T, Omori T, Sutou Y, Kainuma, et al. A simple method to treat an ingrowing nail with a shape-memory alloy device. J Dermatol Treatment. 2008; 19: 291-292.
- Baran R, Dawber RDR, Tosti A, Haneke E. Treatment of common nail disorders. A Text Atlas of Nail Disorders Techniques in Investigation and Diagnosis, 3rd ed. 2003. Martin Dunitz, Tailor & Francis Group London NewYork. 231.
- Takahashi M, Ogata M, Urushibata M, Hino H. Case reports: Four cases treated with Mohs’ ointment. Rinsho derma (Tokyo) 2012; 54: 287- 291.
- Heifetz CJ. Ingrown toe-nail. Am J Surg. 1937; 38: 298-315.
- de Berker DA, Richert B, Duhard E, Piraccini BM, André J, Baran R. Retronychia: proximal ingrowing of the nail plate. J AM Acad Dermatol. 2008; 58: 978-983.
- Ihara H. Mechanoreceptor in sole, Joint training, revision 2nd edition, Neuromotor coordinated training, Cooperative Medical Publisher. Tokyo. 2006; 91-95.
- Hervéou C, Messéan L. New nerves in the knees, ankle joints, and feet – Mechanoreceptor, Translated by Ihara H, Nakayama S, Ishiyaku Publiching. Tokyo. 1985; 2-4.
- Motobe S. Research on the morphology and distribution of nerve ending near the soft tissue of the plantar region. Jl JapOrthopaed Surg Soc. 1967; 41: 275-287.
- Mitchell S, Jackson CR, Wilson-Storey D. Surgical treatment of ingrown toenails in children: what is best practice?. Ann R Coll Surg Engl. 2011; 93: 99-102.









































































































































