Dermoscope for Histologic Examination of Basal Cell Carcinoma
- 1. Eduardo T. Weiss
- 2. Department of Dermatology, Larkin Community Hospital, USA
- 3. Dermatology & Cutaneous Surgery, University of Miami, USA
Abstract
A dermoscope may serve as a useful emergency backup in the absence of conventional light microscopy. A DermLite DL3 was used to examine a frozen section histology slide. In this case, the technique was a quick and efficient technique to identify positive tumor margins. Dermatologists frequently carry dermoscopes and this technique may be useful for rapid examination of slides in austere conditions or when a conventional microscope is not available.
Keywords
Mohs, Basal cell, Dermoscopy
Citation
Mattei PL, Reed AM, Weiss ET (2017) Dermoscope for Histologic Examination of Basal Cell Carcinoma. J Dermatolog Clin Res 5(1): 1094.
INTRODUCTION
Non melanoma skin cancer presents a tremendous burden to the American health care system. Current incidence of this most common skin cancer is estimated at 2-3 million cases per year in the United States and is estimated to be increasing [1]. Mohs micrographic surgery is a technique that offers superior cure rates for many skin tumors. Margins for standard excision are often 4mm for nodular BCC, however, mohs micrographic surgery is performed by taking multiple sections in order to achieve total margin control and individual cases vary in the margins necessary for extirpation. 5 year recurrence rates for basal cell carcinoma treated using the mohs technique are estimated at less than 1% [2]. In the Mohs technique, tissue is collected and processed using frozen sections and cut in a way to reveal the entire tumor margin. These frozen sections are usually evaluated with microscopes having 2.5x, 4x, 10x, and 40x magnification. We present a case in which a microscope malfunction resulted in the inability to utilize conventional light microscopy.
METHODS
A 75 year old man was referred to the office for a Mohs micrographic surgery of a biopsy proven nodular basal cell carcinoma of the right cheek. On clinical examination, a 15mm red pearly telangiectatic plaque was noted on the right cheek. The surgical site was confirmed by the patient and also with a clinical photograph. The first stage was taken using 2mm margins and the histologic specimen was prepared for examination. However, upon examination, the microscope appeared to be malfunctioning and the slides were unable to be read. The slides were placed on a white background and a dermoscope was used to examine them.
RESULTS
Examination with dermoscope revealed, distinct basophilic islands with stromal retraction from 9 O’clock to 12 O’clock (Figure 1);
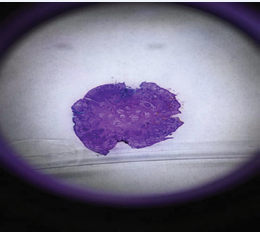
Figure 1 Frozen Section of first stage mohs layer taken with DermLight DL3 and iphone 5s showing islands of basaloid cells from 9 O’Clock to 12 O’Clock.
the remainder of the slide appeared negative. Following identification of the positive margin, a second stage was taken in the same manner and a histologic specimen prepared. We reviewed the specimen using the same technique and the surgical margins were negative (Figure 2).
Figure 2 Frozen Section of second stage mohs layer taken with DermLight DL3 and iphone 5s showing no residual basal cell carcinoma.
A complex linear closure was used to repair the defect. The slides were later reviewed using conventional microscopy which confirmed the dermoscope findings in both settings.
CONCLUSIONS
In this case a dermoscope served as a useful emergency backup in the absence of conventional light microscopy. ADermLite DL3 was used which has a high quality, four-element, 25 mm, 10x lens per manufacturer specifications [5]. In our case, this technique was a quick and efficient technique to identify positive tumor margins. Dermatologists frequently carry dermatoscopes and they are often used to diagnose tumors in vivo [3,4]. Our described technique may be useful for rapid examination of slides in austere conditions or when a conventional microscope is not available. More subtle features may not be apparent using this technique. Very small tumor islands or infiltrative pattern tumors may be difficult to visualize with the dermoscopic technique and as such the slides were later reviewed with conventional light microscopy when a functional microscope became available. We present this case out of interest and suggest that conventional light microscopy remain standard of care.
DISCUSSION
Basal cell carcinoma is the most common malignancy in man. Dermatologic surgeons often encounter these lesions and may employ mohs micrographic surgery to excise these tumors. The mohs micrographic technique relies on rapidly processed frozen sections which can be read while the patient waits, eliminating the need for multiple visits in the event of positive margins. Conventional light microscopy is the preferred technique for interpreting these frozen sections, however, in the event of microscope failure; a dermoscope could serve as an emergency backup provided the sections were later confirmed by conventional light microscopy.
REFERENCES
2. Mohs FE. Chemosurgery: a method for microscopically controlled excision of external cancer. Clin Med. 1955; 2: 781-784.









































































































































