Erythroderma - The First Manifestation of Lepromatous Leprosy or Unsuspected Drug Reaction
- 1. Department of Dermatology, Acapulco Guerrero General Hospital, Mexico
- 2. Section of Mycology, General Hospital Dr. Manuel Gea González, Mexico
- 3. Dermatopathologist, General Hospital Dr. Manuel Gea González, Mexico
- 4. Epidemiologist, General Hospital of Acapulco, Guerrero, Secretary of Health, Mexico
Abstract
Leprosy, a neglected tropical disease continues to be a global health problem. In 2017 Mexico ranked sixth in prevalence and eighth in new cases. Erythroderma is an inflammatory skin syndrome, in adults its etiology is multifactorial, frequently associated with exacerbation of pre-existing dermatosis and secondly to an adverse drug reaction. We present a 64-year-old man with erythroderma and lepromatous leprosy, both confirmed by histopathology. Leprosy was unnoticed and the erythroderma was rapid and transitory, without being able to determine if it was drug induced.
Keywords
Lepromatous leprosy, Neglected tropical disease (NTD), Erythroderma, Inflammatory syndrome, Psoriasis, Adverse drug reaction
Citation
Romero M, Arenas R, Vega E, Juárez-Durán ER, Castillo A (2020) Erythroderma - The First Manifestation of Lepromatous Leprosy or Unsuspected Drug Reaction? J Dermatolog Clin Res 8(2): 1135.
INTRODUCTION
Leprosy is considered by the World Health Organization (WHO) as a neglected tropical disease of mandatory notification [1]. In Mexico it is endemic and continues to be a public health problem. In the other hand, erythroderma is an inflammatory syndrome of the skin characterized by erythema and scaling on more than 90% of the body surface, its presentation can be acute and chronic. In adults its etiology is multifactorial, the most frequent causes are due to a complication of a previous dermatosis, such as psoriasis, atopic dermatitis, lymphoproliferative diseases, drug-related, or idiopathic [2-4]. We present a case of leprosy and erythroderma both confirmed by histopathology.
CASE PRESENTATION
A 64-year-old man farmer, resident of “Parotas” Municipality of Tecpan de Galeana, Guerrero (Mexico). The patient has a history of type 2 diabetes mellitus controlled with glibenclamide for 12 years, intake of alcoholic beverages once a week, denies a history of allergies to medications.
He attended to our clinic for evaluation of an asymptomatic dermatosis with a tendency to generalization consisting of erythema, scaling, irregular infiltrated plaques and others with psoriasiform appearance, respecting the face at the frontal region, axillary folds, genital area, ankles and both feet (Figures 1-4).

Figure 1 A. Erythroderma with infiltrated plaques. B. Infiltrated plaques in thorax.

Figure 2 Psoriasiform plaques with erythema and scales.
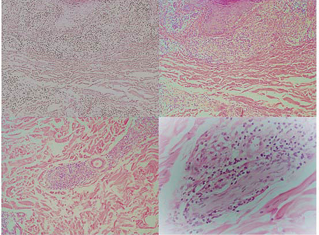
Figure 3 A. Histopathological examination showed epidermis with acanthosis and spongiosis, in the superficial dermis a moderate perivascular lymphohistiocytic infiltrate. (Hematoxylin-eosin stain 20x). B.- In the superficial and middle dermis, the inflammatory infiltrate was nodular, around the nerves, annexes, and the blood vessels, with vacuolated histiocytic cells. (Hematoxylin-eosin stain 20x).
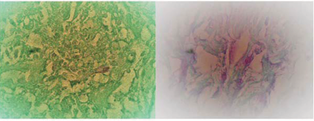
Figure 4 A. Close up. The inflammatory infiltrate around the nerve. (Hematoxylin-eosin stain x60). B.- Fite-Faraco stain was positive for few bacilli (100x).
He refers a 3-month history with asymptomatic “small rashes” in the chest and back.
The patient was initially managed with antihistamines drugs but no improvement was observed, and after 15 days he had a very severe erythematous hot skin. In a second time the patient was started on a regimen of oral montelukast 10mg, levocetirizine 5mg, deflazacort 6mg, fluconazole 150mg, and tacrolimus ointment 0.1%.
Skin biopsy for histopathological examination was performed with clinical diagnosis of erythroderma secondary to psoriasis or lymphoproliferative process.
Histopathological examination showed the epidermis with spongiosis, in the superficial dermis edema between the collagen fibers and a moderate perivascular lymphohistiocytic infiltrate.
In the superficial and middle dermis, the inflammatory infiltrate was nodular, around the nerves, annexes and the blood vessels, with vacuolated histiocytic cells. In the subcutaneous cellular tissue, there was a granulomatous infiltrate with giant cells.
Fite-Faraco staining was positive for few bacilli. The diagnosis of erythroderma and lepromatous leprosy was integrated.
At the moment of clinical examination there were no apparent manifestations of leprosy and the patient has not a familial history of leprosy.
Later the patient was admitted to a military hospital in Mexico City where his erythroderma was solved. Upon discharge, he went to a first-level health care center, where he underwent acid fast bacilli (AFB) on smear of cutaneous lymph, which was positive (+++). Multi drug therapy (MDT) for leprosy (dapsone, clofazimine and rifampicin) was provided. Clinical manifestations of erythroderma improved after suspending all previous medications, and after 3 months of MDT, leprosy showed a good evolution with a negative AFB smear. He is currently under epidemiological surveillance.
REFERENCES
2. Arenas R. Dermatología Atlas diagnóstico y tratamiento. McGraw-Hill. 7 edn. México. 2019.
3. Secretaria de Salud. Manual de Procedimientos Estandarizados para la Vigilancia Epidemiológica de las Micobacteriosis [Tuberculosis y Lepra]. 2019.
5. World Health Organization. Global leprosy update, 2017: reducing the disease burden due to leprosy. Weekly epidemiological record. 2018; 35 445-456.
6. World Health Organization. Table 7. Global leprosy situation by WHO región, country and territories 2017. Weekly epidemiological record. 2018; 35: 445-456.
7. Secretaria de Salud. Anuarios de morbilidad. Incidencia de Lepra (A30) por grupos de edad Estados Unidos Mexicanos 2018. Población General.
15.Li J, Zheng HY. Erythroderma: A Clinical and Prognostic Study. Dermatology. 2012; 225: 154–162.
20.Khan DA. Cutaneous drug reactions. J Allergy Clinic Immunol. 2012; 130: 1225–1225.







































































































































