Gastric Sarcoidosis: An Atypical Presentation of a Rare Disease
- 1. Department of Internal Medicine, Istanbul University, Turkey
- 2. Department of Pulmonary Medicine, Istanbul University, Turkey
- 3. Department of Pathology, Istanbul University, Turkey
Abstract
Sarcoidosis is a multi systemic granulomatous disease characterised by the histologic evidence of granulomas in various organs. Clinically discernible gastric sarcoidosis is extremely rare, reported in less than 1% of the patients. We present a case of gastric sarcoidosis with atypicial manifestations and without current pulmonary disease. The patient was admitted for gastric fullness, anorexia, and weight loss. She had a history of migraine and nodular goiter. Family history revealed bladder carcinoma in the mother and gastric carcinoma in the uncle. Initial laboratory findings and chest x-ray were normal. Biopsies from the gastric mucosa revealed non caseating granulomas with focal multi nucleate giant cells. Six months after the patient was admitted for dry cough and fatigue. Chest x-ray and CT revealed diffuse nodules in the upper and middle lung zones. Trans bronchial biopsy demonstrated noncaseiting granulomas compatible with sarcoidosis. The patient was started on mehtylprednisolone and had a significant improvement in her symptoms.
This case is an unique paradigm for the exceptional presentation of sarcoidosis. Isolated extrapulmonary organ involvement without simultaneous lung disease may be the initial manifestation of sarcoidosis. Meticulous follow-up for sarcoidosis is required for patients presenting with atypical symptoms and noncaseiting granulomas in any extrapulmonary organ.
Keywords
• Gastric sarcoidosis
• Granulomas
• Biopsies
• Sarcoidosis
• Biopsies
Citation
Yanardag H, Tetikkurt C, Bilir M, Kepil N, Verdi Y (2017) Gastric Sarcoidosis: An Atypical Presentation of a Rare Disease. J Autoimmun Res 4(2): 1020.
INTRODUCTION
Sarcoidosis is a chronic systemic disease of unkown etiology characterized by the formation of noncaseiting granulomas in various organs [1]. The clinical manifestations of sarcoidosis are highly variable and nonspecific. Although thoracic involvement occurs in more than 90% of the patients, every organcan be affected [2-4]. Gastrointestinal tract involvement is rare with an incidence of less than %1. Stomach is the most common site but these cases are often clinically silent [5,6]. In literature, there are only few cases of symptomatic gastric sarcoidosis with documented histopathological evidence of noncaseiting granulomas [7]. Diagnosis of isolated gastric sarcoidosis constitutes difficulties for the clinician due to its atypical clinical profile and subclinical occurence.
We report a case of gastric sarcoidosis presenting without initial pulmonary disease. Gastric sarcoidosis is a rare form of extrapulmonary sarcoidosis and clinicians should bear in mind that isolated gastric sarcoidosis may occur without simultaneous pulmonary involvement.
CASE REPORT
A 55 year old Caucasian female was admitted for gastric fullness, anorexia, and weight loss (6 kg) in the last three months. She had a history of migraine and nodular goiter. Her mother had bladder carcinoma and her uncle had died of gastric carcinoma. She was an ex-smoker for 10 years with a previous smoking history of 10p/year. Physical examination was remarkable for mild tenderness in the epigastric area.
Her initial laboratory revealed WBC 5.9X103 /mm3 , hemoglobin 14 g/dl, platelets 288X103 , lymphocytes 1.4X103 , creatinine 0.88 mg/dl, AST 18 IU/L, ALT 20.6 IU/Lmm3 , LDH 201 IU/L, albumine 5.1 gr/dl, CRP 0.5 mg/dl, and calcium 8.9 mg/dl. ECG showed sinus ryhtm.Serum ACE was 18 IU/L. Tuberculine test was negative. Chest x-ray (Figure 1)

Figure 1: Intial normal chest x-ray
was normal. Stool studies were negative for blood, culture, and parasites. Histopathology of the gastric mucosal biopsies taken from the white miliary nodules in the corpus revealed granulomatous gastritis multiple small noncaseiting granulomas composed of epitheloid cells, histiocytes, and multinucleated giant cells (Figure 2,3)
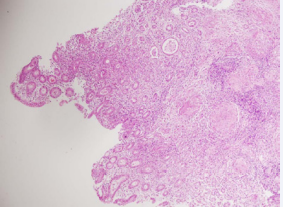
Figure 2: Histopathology of gastric mucosal biopsy showed discreet noncaseiting granulomas composed of epithelial histiocytes and multinucleated giant cells in the lamina propria (HE X100, X400).
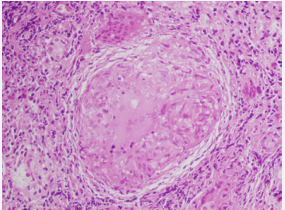
Figure 3: Histopathology of gastric mucosal biopsy showed discreet noncaseiting granulomas composed of epithelial histiocytes and multinucleated giant cells in the lamina propria (HE X100, X400).
while colonoscopic examination was normal. Biopsies stained for Helicobacter pylori, M. tuberculosis, fungal oranisms,and culture of the gastric aspirate were negative. Other laboratory workup to rule out differential granulmatous etiology was not diagnostic. Treatment with proton pump inhibitors was not useful.
Six months later the patient was admitted for dry cough and fatigue. Blood count was WBC 6.2X103 /mm3 , hemoglobin 13.8 g/dl, platelets 284X103 , and lymphocytes 1.6X103 /. creatinine 0.76 mg/dl, AST 20 IU/L, ALT 24IU/Lmm3 , LDH 208 IU/L, albumine 4.2 gr/dl, CRP 0.4 mg/dl, and calcium 8.6 mg/ dl. Urine analysis was normal. Chest x-ray showed bilateral multiple nodules (Figure 4).

Figure 4: Chest x-ray showed bilateral micronodular opacities
Thorax CT revealed micro nodular centrilobular nodules, thickened interlobular septa,and ground glass opacities in both upper and middle zones (Figure 5,6).

Figure 5: Computed tomography of the thorax revealed micronodular centrilobular nodules and thickened interlobular septa in both upper and middle zones.
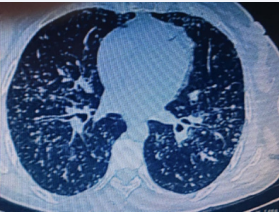
Figure 6: Computed tomography of the thorax revealed micronodular centrilobular nodules and thickened interlobular septa in both upper and middle zones.
Serum angiotensin-converting enzyme level was 76 IU/L. Smear and culture of BAL sample was negative for bacteria, fungus and mycobacteria. Histopathologic examination of the bronchoscopic mucosal biopsy samples revealed non caseiting granulomatous inflammation with histiocytes, epitheloid, and multinucleated giant cells. A diagnosis of sarcoidosis with gastric involvement was made. A twelve month course of methylprednisolone treatment led to complete resolution of gastric and pulmonary symptoms.
DISCUSSION
The disease course in sarcoidosis is highly variable. Although the lungs are the most commonly affected organ, concomitant involvement of extrapulmonary organs can be seen in up to 50% of cases [8]. On the other hand, GI tract involvement is uncommon and extremely rare. It is reported in less than 1% of the patients [1]. True incidence may be unknown due to the great number of asymptomatic patients [5]. We present a case of gastric sarcoidosis presenting with atypical symptoms and histopatologic evidence of noncaseiting granulomatous inflammation of the corpus without lung involvement.
Diagnosis of sarcoidosis is based upon a compatible history, the presence of granulomas in at least two organs, negative staining or culture for acid fast bacilli, and lack of exposure to toxins or drugs. Granulomatous inflammation only in one organ is not diagnostic of sarcoidosis. Histologic confirmation may not be required in a second organ if the alternative causes of granulomatous inflammation is excluded [1,6,9,10]. Clinical presentation of gastric sarcoidosis varies depending on the intensity of granulomatous inflammation. The disease usually manifests itself as gastric ulcer or diffuse infiltration of gastric mucosa with granulomas causing luminal narrowing [5,6,11]. In our case, the patient had white miliary nodules in the corpus. The initial symptoms, presentation,clinical manifestations,and the laboratory findings were not compatible with sarcoidosis. Only the gastric mucosa biopsy revealed noncaseiting granulomatous inflammation that may be associated with variousgranulomatous diseases including sarcoidosis. There was no lung or any other extrapulmonary organ involvement pointing out to sarcoidosis initially. The diagnosis was confirmed six months later by transbronchial biopsy when the patient presented with dry cough, fatigue,and nodules in the chest CT.
Our case presented with an unusual manifestation of sarcoidosis having an isolated and a rare organ involvement. Clinically recognizable GI involvement is uncommon occuring in less than %1 of the patients, although the incidence of subclinical disease may be much higher [1,12,13]. On the other hand, granulomas in the gastric biopsy specimens are extremely rare and are mostly associated with Crohn’s disease, tuberculosis, histoplasmosis, isolated granulomatous gastritis, vasculitis, and lymphoma [7,14-16]. Second the symptoms were exceptional. Third, lung disease occured six months later than the gastric involvement. Fourth, fhe laboratory results were indecisive and nonspecific. The patient did not have any respiratory symptoms initially and thorax CT was not performed. It may be considered unusual for a patient with a normal chest x-ray to develop stage III disease after six months. If CT had been done at admission the lung parenchyma would be much more delineated. Consequently, the final diagnosis was conclusive.
Clinicians should bear in mind that sarcoidosis may present with an isolated and an unusual organ involvement without clinical evidence of current lung disease that may lead to a diagnostic dilemma. Follow up of such patients constitutes a crucial and critical step for final diagnosis.






































































































































