Anger: Its Impact on Discrete Emotions and Posttraumatic Stress
- 1. University of Washington Tacoma, Tacoma, USA
- 2. Seattle Pacific University, Seattle, USA
Abstract
Anger is often presumed to be a defensive emotion, masking the ability to feel other discrete emotions. College students (N = 176) were randomly assigned to anger priming via feigned extra credit revocation, autobiographical recall, or no priming. Students then watched the Discrete Emotion Video Clips and reported how much they felt a range of emotions on the Post Film Questionnaire. Those assigned to either of the anger priming conditions reported significantly greater amusement intensity following the associated movie clip viewing than those not anger primed (p < .05). For a subset of participants who completed the Posttraumatic Stress Disorder Checklist (n = 109), amusement negatively predicted Posttraumatic Stress Disorder symptom intensity (r = -.22; p < .05). These findings bring into question the clinical assumption that anger is used to avoid or mask feelings of disgust, fear, or sadness as no relationship was found between anger priming and these negative discrete emotions. Findings also raise important questions for future research.
Keywords
• Anger
• State anger
• Trait anger
• Discrete emotions
• Posttraumatic stress
Citation
Edwards-Stewart A, Keller CJ, Ahmad ZS, June J, Hamann R, McBrearty M (2016) Anger: Its Impact on Discrete Emotions and Posttraumatic Stress. J Behav 1(1): 1001
Abbreviations
EFT: Emotion-focused therapy; ACT: Acceptance and commitment therapy; PTSD: Posttraumatic stress disorder; STAXI-2: State-trait anger expression inventory-2; PCL: Posttraumatic checklist-civilian version; ANOVA: One way analysis of variance; MANOVA: One-way multivariate analysis of varian
INTRODUCTION
Chronic habitual anger may limit an emotional range or dampen an individual’s ability to access other discrete moods, both positive and negative. Discrete emotions are generally agreed to include: joy (sometimes discussed as happiness or amusement), fear, sadness, anger [1,2], contentment, disgust, surprise, and anxiety [3]. The theory that one emotion may function to truncate one’s emotional range (i.e., suppress others) is a phenomenon identified in some cognitive and behavioral therapies, such as Emotion-Focused Therapy (EFT) [4] and Acceptance and Commitment Therapy (ACT) [5].
Problematic anger is the focus of this study. Manifested in several ways, problematic anger includes hate, rage, destructive anger, and rejecting anger [6]. Using an EFT frame, problem anger can develop through many pathogenic pathways. Often maladaptive or inflexible primary emotions originate from childhood where the emotions were once adaptive. For example, if a child learned to feel angry to scare off potential abusers that anger was once very adaptive. In contract, using anger as an adult when not feeling emotionally safe is maladaptive as it no longer advances the relational safety needs of an adult. Therefore, maladaptive emotions are negative emotional experiences that occur repeatedly, are self-perpetuating, and are resistant to change [7]. Both primary and secondary anger may become characterological or a trait, rather than a discrete affective event or a state reaction. For instance, anger can lead to a relational style over time that is fundamentally rejecting of others. Through reinforcement, this pattern becomes a characterological way of being. This phenomenon is often exhibited in individuals with a complex trauma history; habitual anger reflects the emotional pain that has been endured historically while simultaneously serving a protective function by signaling others to keep a distance [8]. Anger, therefore, can manifest as a defensive strategy [6,9].
Within an ACT conceptualization, the emotion of anger may function to avoid a wider range of emotions. Anger may serve to perpetuate cognitive fusion (i.e., being unable to adaptively distance one’s self from thoughts) and experiential avoidance (i.e., pushing away internal or external negative experiences). Problem anger, according to ACT, is understood not so much to be a problem with the emotion of anger but the reactive behaviors typically associated with anger [10]. Accepting the emotion of anger may allow an individual to be more reflective about their experience, cultivating a posture of openness toward other emotions. Through the acceptance of the emotion of anger, individuals can develop psychological flexibility through mindfully focusing on adaptive, value-consistent behaviors. Often avoidant behaviors perpetuate the suppression of emotion requiring ongoing avoidant strategies. Consistent with an ACT perspective, the current investigation hypothesizes that problem anger functions to dampen primary emotions that are both negative and positive.
The goal of this study was to explore the relationship between problematic anger (measured as trait anger) and its impact on ability to feel other discrete emotions. State anger is also measured to induce determine if non-characterological anger alone affects ability to feel other moods. Two hypotheses were explored. The first hypothesis (H1) is that state anger, when primed, reduces reported experiences of positive and negative discrete emotions; the second hypothesis (H2) is that trait anger decreases reported experiences of positive and negative emotions.
Because defensive anger has been noted to be associated with trauma [8], the PCL-C was given to 109 of the participants. For these participants, two additional hypotheses were investigated: (H3) Posttraumatic Stress Disorder (PTSD) symptoms, when primed with state anger, reduce reported experiences of positive and negative discrete emotions and (H4) PTSD symptoms and trait anger impact ability to feel both positive and negative discrete emotions. This secondary study used the same methodology as the first with the inclusion of a self-report assessment of PTSD symptoms.
MATERIALS AND METHODS
Participants
Participants in the present study were undergraduate students recruited from a large public state university in Western Washington. Students were invited from several subject areas (including psychology and mathematics) and given extra credit in exchange for their participation. The majority of students in invited classes participated. Participants ranged in age from 18 to 49 with a mean age of 23. The majority of the sample was Caucasian (49%) followed by 40% African American, 5% Asian, and 5% biracial. The sample was 52% women.
Procedure
This study was approved by the University of Washington Institutional Review Board. The study consisted of 176 participants. Participants reported to a sign up table and were given a consent form and time to individually ask questions about the study. Participants were randomly assigned to one of three conditions. The first condition aimed to induce anger by telling students they did a poor job interpreting a poem and would therefore lose extra credit points (a novel anger induction that was found in the below manipulation check to induce state anger). The second condition was also an anger induction condition which had participants recall an autobiographical time of anger (a common form of mood induction) [11] and the third condition was the control. Two forms of anger priming were used to determine whether deception in anger induction might be more effective than recall of anger. While the deception method might have also elicited other emotions (depression, anxiety, etc.), state anger was found in the below manipulation check to be present. The procedure varied based on condition, however all conditions included: initial priming or no priming state (priming conditions are described below), completing a demographic questionnaire, viewing seven movie clips designed to elicit different mood states and completing the Post Film Questionnaire [3], completing the State-Trait Anger Expression Inventory-2 (STAXI-2), and being debriefed on the actual nature of the study.
Participants in condition one were asked to write a response essay to a poem (Fire and Ice, by Robert Frost) and were informed that the quality of their response (rated as ‘good,’ ‘neutral,’ or ‘poor’) would determine the amount of extra credit they received. In this condition, state anger was invoked by each participant receiving a “poor” grade for their essay, regardless of the quality of their essay. Specifically, participants received a sealed envelope informing them of both their ‘poor’ work and decreased amount of extra credit (5 out of the possible 10). In the second condition, participants were asked to write a brief essay recalling an auto-biographical experience of anger. Participants were asked to try and feel those angry feelings in the present. In the third, control condition, participants received the same poem as in condition one and were asked to write an essay in response to the poem. However, in this condition, they were not given feedback on their written response nor were they told that their essays would be graded.
Of the total of 176 participants, 109 participants completed the Posttraumatic Checklist-Civilian Version (PCL-C) following their completion of the STAXI-2 and before they were debriefed. Sixty-seven participants did not complete the PCL-C.
Instruments
Demographic questionnaire: Participants completed a brief demographic questionnaire asking for the participant’s age, gender, race, current class standing in college, relationship status, and religious affiliation.
State-trait anger. The STAXI-2 consists of 57 items, with six scales, five subscales, and an Anger Expression Index. It was created to provide a measure of expression and control of anger. This measure was developed to assess anger as it distinguishes between expressions of normal versus abnormal anger and serves as a way to measure various aspects of anger as related to various medical conditions shown to relate to anger. Alpha co-efficient measures of internal consistency identified consistently good reliability across all scales and sub-scales (.84 or higher with a median of .88) and validity was also found to be appropriately established [12].
Discrete emotion video clips: Gross and Levenson (1995) created a series of eight film clips to elicit emotional responses in a laboratory setting. These emotional states are: amusement, anger, contentment, disgust, fear, neutral, sadness, and surprise. Each clip was determined to have varying statistical ability to induce the target emotion (entitled the clips “hit rate”) which was determined using the Post Film Questionnaire. This questionnaire consists of a list of various emotion states. The participant is asked to rate how much they felt each emotion while watching the film according to a 9-point Likert scale ranging from 0 (not at all/none) to 8 (extremely/a great deal). For the present study, all 8 clips were shown, but only four were used for analysis due to their relevance to the current topic and their high hit rate, as determined in the original study. Specifically, for amusement, the When Harry Met Sally “discussion of orgasm in café” had a hit rate of 93.1; for disgust, the Pink Flamingos “person eats dog feces” had a hit rate of 84.9; for sadness, The Champ “boy cries at father’s death” had a hit rate of 94.2; and for fear, The Shining “boy playing in hallway” had a hit rate of 71.2.
Posttraumatic Checklist-Civilian Version (PCL-C): The PCL-C [13] is a 17-item self-report measure of posttraumatic stress symptoms reflecting DSM-IV criteria for PTSD. The questions in the civilian version of this measure ask about generic stressful experiences and are meant to be used with any population. Participants rated how much they had been bothered by each symptom in the past month on a 5-point scale ranging from 1 (Not at all) to 5 (Extremely). Scores range from a 17 to 85.
RESULTS
Preliminary Analyses/Manipulation Check
A manipulation check was conducted to determine if the priming conditions induced state anger as proposed. A one-way analysis of variance (ANOVA) was conducted. The independent variable was condition and therefore had three levels: condition 1 (extra credit anger), condition 2 (autobiographical anger), and condition 3 (control condition). The dependent variable was state anger as measured by the STAXI-2. The ANOVA was significant, F(2, 167) = 4.76, p = .01, η² = .05. The strength of the relationship between condition and state anger was relatively small overall, only accounting for 5% of the variance. Follow-up tests were conducted to evaluate pairwise differences among the means (see Table 1). There was a significant difference between condition 1 and condition 3, as well as condition 2 and condition 3. This indicates that both condition 1 and 2 created elevated state anger compared to the control.
Main Analysis
H1. A one-way ANOVA was conducted to evaluate the mean difference between condition and the positive discrete emotion, amusement. In all hypotheses, the positive discrete emotion (amusement) was explored separately from the three negative emotions (disgust, fear, and sadness). This was done due to the varying valence between positive and negative emotions. The independent variable, conditions, had three levels. The dependent variable was level of amusement reported. The ANOVA was significant, F(2, 168) = 3.27, p < .05, η² = .04. The strength of relationship between condition and reported level of amusement (as assessed by η²) was small with the condition accounting for four percent of the variance in level of reported amusement.
Follow-up tests were conducted to evaluate pairwise differences among the means. There was a significant difference in means between both conditions 1 and 2 compared to condition 3. Both conditions showed increased reported levels of amusement compared to the control. There was no significant difference between conditions 1 and 2. The pairwise differences in means and standard deviations for the three conditions by amusement are reported in Figure 1.
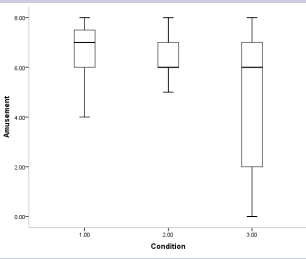
Figure 1: Changes in reported amusement levels by conditio
A one-way multivariate analysis of variance (MANOVA) was conducted to determine the effect of conditions on the three dependent variables of disgust, fear, and sadness. No significant differences were found among the conditions on the dependent measures, Wilks’s Λ = .95, F(2,164) = 1.43, p = .20. The multivariate η² based on Wilks’s Λ was small (.03).
H2. A series of linear regression analyses were conducted to evaluate the prediction that trait anger would have an impact on ability to feel the discrete emotions currently under investigation (amusement, disgust, fear, and sadness). None of the regressions were significant (see Table 2).
H3. This hypothesis seeks to explore if PTSD symptoms impact ability to experience various discrete emotions. Given this and the method used in the current study, an initial correlation was conducted between PTSD symptoms and state anger to identify if this might confound the measurement of PTSD symptoms as they relate to primed anger. The correlation coefficient computed between PTSD symptoms and state anger was .14, displaying a minimal positive, linear relationship between PTSD symptoms and state anger. This finding was not significant, p = .15.
PCL scores range from 17 to 85 with a mean score of 35 and standard deviation of 15. Five linear regression analyses were conducted to predict PCL scores impact on level of reported discrete emotions. The analysis including amusement was significant while the others comprised of anger, disgust, fear, and sadness were not significant (see Table 3 for non-significant regression equations). Anger was included in this analysis to determine if experience of anger was different based on PCL-C scores. Experience of anger was collected by the Discrete Emotion Video Clips by Gross and Levenson (1995) as was the case for all participants.
The scatterplot for the PCL and amusement indicates that the two variables are linearly related such that as PCL scores increase amusement decreases. The regression equation was significant, R2 = .05, F(1,106) = 5.14, p < .05. The regression equation for predicting the overall injury index is
Predicted Overall PCL Score = -.05 Overall Amusement = 7.9
The 95% confidence interval for the slope, -.10 to -.01, does not contain the value of zero, therefore the PCL is significantly related to amusement. The correlation between PCL and amusement was -.22. Approximately five percent of the variance of amusement was accounted for by its linear relationship with PCL scores.
H4. A correlation coefficient was computed between PTSD symptoms and trait anger to confirm past research findings that the two variables were related. The results were statistically significant (r = .37, p < .01.
A series of linear regression analyses were conducted to evaluate the prediction that PTSD symptoms and trait anger would have an impact on ability to feel the discrete emotions currently under investigation (amusement and disgust, fear, and sadness). None of the regressions were significant (see Table 4).
Tables 1: 95% Confidence intervals of pairwise differences in mean changes in state anger
| Conditions | M | SD | Condition 1 | Condition 2 |
| Condition 1 | 49.37 | .94 | ||
| Condition 2 | 50.68 | .96 | ||
| Condition 3 | 46.49 | .99 | .17 to 5.59 | 1.46 to 6.93 |
| Abbreviations: M: Mean; SD: Standard Deviation | ||||
Table 2: Regression equations of trait anger by discrete emotion
| Discrete emotion | R | F | df | p value |
| Amusement | 0.03 | 0.15 | -1,167 | 0.69 |
| Disgust | 0.01 | 0.01 | -1,167 | 0.94 |
| Fear | 0.02 | 0.05 | -1,165 | 0.82 |
| Sadness | 0.04 | 0.3 | -1,164 | 0.58 |
Table 3: Non-significant regression equations for PCL by negative discrete emotion
| Discrete emotion | R | F | df | p value |
| Amusement | .09 | .92 | (1,105) | .34 |
| Disgust | .01 | .02 | (1,105) | .89 |
| Fear | .06 | .38 | (1,105) | .54 |
| Sadness | .13 | 1.74 | (1,105) | .19 |
Table 4: Non-significant regression equations of PTSD symptoms and trait anger by discrete emotion
| Discrete emotion | R | F | df | p value |
| Amusement | .15 | 1.19 | (2,103) | .31 |
| Disgust | .11 | .60 | (2,102) | .55 |
| Fear | .13 | .90 | (2,102) | .41 |
| Sadness | .15 | 1.19 | (2,102) | .31 |
DISCUSSION
This study explored how anger, state and trait, influenced reported experiences of various discrete emotions. We explored both positive and negative emotions. We predicted that primed anger would decrease reported experiences of negative emotions such as fear or sadness. If such a relationship is present, it arguably could differ for non-clinical groups versus clinical groups. However, for the initial exploration of this assumption, a non-clinical group was chosen to determine if this was a typical experience for any individual regardless of diagnosis or syndrome. Further research would need to explore this assumption by including different clinical populations in the sample. Positive emotions are not typically identified in any assumptions on anger and discrete emotions but the present study wished to explore this dimension. If anger does indeed dampen various negative emotions, perhaps it also affects the experience of positive ones. This exploration was indeed the most interesting in the present study, as amusement was the only significant variable regardless of the independent variable.
In regards to state anger, it appears that when a non-clinical group is primed, they experience higher levels of amusement than if they were not. While the explained variance between the variables is small, meaning there are other variables that impact amusement levels beyond state anger, it appears that higher state anger shortened the reported range of experience of amusement. When considering Figure A, it appears that individuals in conditions 1 and 2 all reported amusement in response to the video stimuli where condition 3, the control, had a full range of reported amusement. While the mean levels of amusement were significantly different between the primed and control, a few individuals in the control reported no amusement when viewing the stimulus which was not the case in the primed conditions. A possible explanation for this finding could be that emotions, physiologically speaking, are indistinct. It is only cognitions and interpretation of emotional stimuli that differentiate the different mood states. Therefore, anger is similar to amusement in that one likely experiencing increased heart rate, breathing, and muscle tension while having these emotions and to be primed to feel anger can easily be confused with experiencing amusement when the stimulus changes.
In terms of problematic or trait anger and its impact on positive and negative discrete emotions, there were no significant results. This indicates that characterological anger that was represented in the current sample (trait anger had a range of T scores from 74-32 with a mean of 48), does not appear to have a dampening relationship with reported experiences of the explored positive and negative emotions. Given the theoretic assumptions around problematic anger and its impact on other negative mood states, it appears that for a non-clinical population, simply priming those with and without problematic/trait anger does not globally diminish ability to feel these emotions. These results could be artifacts of an experimental design, where discrete emotions were elicited outside of a personally meaningful context that did not naturally trigger defensive anger.
In regards to the second aim of this study and the relationship between PTSD symptoms and discrete emotions, it appears that as PCL scores increase, reported amusement decreases. This indicates that something about PTSD symptoms, in a non-clinical population, has the opposite impact on amusement than primed state anger alone. It appears that the indistinct view of emotions postulated above might not apply to a group with PTSD symptoms. This may be due to the diagnostic criteria for PTSD that identifies a persistent inability to experience positive emotions. The explained variance in this study was small, however, indicating that other variables likely explain reported experiences of amusement other than PTSD symptoms.
It was interesting that reported experiences of disgust, fear, or sadness were not influenced by increases in PTSD symptoms. This simply indicates that as PTSD symptoms increase, this nonclinical group did not report higher or lower experiences of negative discrete emotions than those with no PTSD symptoms. While this finding is interesting because it is the first of its kind, it much also be treated with caution. This data is inherently limited as it was explored among a non-clinical population, thereby the actual amount of those with PTSD symptoms were small (a total of 21 participants out of 109 had a PCL-C score of 50 or above), and the methodology of this study was also designed with a priming condition of state anger. The current exploration should therefore be explored with a clinical group.
Finally, the current study supports past research that trait anger has a positive relationship with PTSD symptoms [14]. However, it does not appear that defensive or trait anger and PTSD symptoms influence reported experiences of any of the positive or negative discrete emotions currently under investigation. This indicates that trait anger and PTSD symptoms do not appear to have an impact on experiences of amusement, anger, disgust, fear, or sadness.
CONCLUSION
The limitations of the current study are the relatively small effect sizes. To the authors’ knowledge, this study is the first of its kind, and thereby important to the field. There are, however, other factors that likely explain an individual’s ability to feel amusement in any given moment. Therefore, the present study can only serve to illuminate a novel concept that has not been previously investigated. This study should not be considered as fully elucidating the relationship between state and trait anger, nor the relationship between defensive anger and ability to feel discrete emotions. Further limitations involve the method used in the current study. Anger could not be measured before priming since deception was used in one of the priming conditions. Doing so would have made the participants aware of the context of the study, and at least for condition 1, this could not occur. Since it appears that condition 1 and 2 were comparable in priming anger, this deception might not be necessary. In future research defensive anger should be explored with different clinical samples to identify if primed defensive anger can affect ability to feel other vulnerable negative mood states such as shame. For a non-clinical group, primed defensive anger does not appear to have this kind of global impact on negative emotions.
In summary, this study was the first to investigate this theoretical concept experimentally and therefore has value but follow-up research is needed to explore the relationship between problematic or trait anger in a clinical population, using priming conditions that elicit personally meaningful defensive anger, and its impact on ability to feel other discrete emotions.
DISCLOSURE
The authors declare no conflicts of interest.
REFERENCES
1. Frijda NH. Emotion, cognitive structure, and action tendency. Cognition Emotion. 1987; 1: 115-143.
3. Gross JJ, Levenson RW. Emotion elicitation using films. Cognition Emotion. 1995; 9: 87-108.
4. Greenberg LS. Emotion-focused Therapy. Clin Psychol Psychot. 2004; 11: 3-16.
7. Greenberg LS, Paivio SC. Working with emotions in psychotherapy. New York: Guilford Press; 1997.
About the Corresponding Author
Dr. Amanda Edwards-Stewart
Summary of background:
Clinical Psychologist currently working for a Department of Defense organization. Also, works as adjunct faculty at Northwest University and maintains a private practice in Seattle, WA.
Current research focus:
• Media contagion
• Virtual reality exposure therapy
• The use of technology to improve service members behavioral health,and posttraumatic stress outcomes in outpatient military behavioralhealth clinics
Websites
ResearchGate - https://www.researchgate.net/profile/Amanda_ Edwards-Stewart
LinkedIn - https://www.linkedin.com/in/amanda-stewart-729b1355
Permanent e-mail address: amandaedwardsstewart@gmail.com









































































































































{kind=link}