The Role of Metabolites in Addiction to Dopaminergic Substances
- 1. Cornell University, United States
Abstract
The United States currently suffers from a mass drug addiction issue. Though various strategies have been put into place to battle this problem, there are still some holes in the knowledge we have of the mechanisms underlying addiction-specifically, the role that metabolism plays in addiction. This study aims to explore the potentially essential part that such metabolites play in the acquisition of addiction, aiming to raise attention to the topic for further laboratory experiments.
Keywords
• Drug addiction
• Dopamine receptors
• Monoamine neurotransmitters
• Psychoactive drugs
• Antidepressant drugs
• Drug metabolism
Citation
Selim M (2020) The Role of Metabolites in Addiction to Dopaminergic Substances. J Behav 3(1): 1016.
INTRODUCTION
Cocaine is a psychoactive drug that produces its behavioral and physiological actions by blocking the three monoamine NTs: dopamine, norepinephrine, and serotonin [1]. Notably, cocaine increases extracellular dopamine levels by binding to the dopamine transporter (DAT) and blocking its function. Researchers claim that the increase of mesolimbic dopamine transmission to the nucleus accumbens (NAc.) is the defining feature of the initiation and maintenance of physical dependence on cocaine [2]. However, several other drugs also exert their effects by blocking the DAT, yet they do not exhibit the euphoric and addictive properties of cocaine. In this study, we will specifically take a look at the neuropharmacology of bupropion, a well-known anti-depressant that produces its effects through blocking the DAT.
Though cocaine and bupropion share this critical feature of blocking the DAT, they could not be more different pharmacologically. As a result of this observation, this study aims to show the “missing link” that is causing severe cocaine dependence. Though it is well-established that physical dependence is initiated through enhanced dopamine release in the VTA-NAc [2], it is hypothesized that the maintenance of addiction is a result of the compounds formed as cocaine is metabolized-its metabolites. This should be tested by assessing the pharmacokinetics of said metabolites, specifically Norcocaine, and comparing them to the metabolites of Wellbutrin and their effects.
SIGNIFICANCE
The National Institute on Drug Abuse reported that, in 2014, about 913,000 Americans met the DSM-IV criteria for cocaine dependence and this rate of addiction has remained pretty steady in following years [3]. Currently, there are no approved drugs for the treatment of cocaine dependence and this is primarily a result of the limited knowledge we have on the neuropharmacological mechanisms behind behavioral and physiological changes associated with cocaine administration. Coming to understand all the small facets of addiction formation will bring us one step closer to helping those struggling with addiction recover.
Several researchers highlight the importance of the dopamine pathway when discussing cocaine dependence. The NAc. Is most commonly incriminated of being the “universal addiction site” due to its role in activating the reward system and, therefore increasing cocaine craving and initiating dependence as a result of increased dopamine neurotransmission [4]. However, emerging studies have indicated that while dopamine release is critical, it is not the only component of cocaine addiction. A recent study showed that mice bred to lack the glutamatergic mGluR5 receptor do not self-administer cocaine, despite the increased dopamine levels in the NAc.-showing that there are other factors determining this neurological change [5]. This same study showed that even with this additional information on the role glutamate plays, neither GABA agonists nor dopamine antagonists have been able to significantly reduce the euphoric effects that come with cocaine in controlled studies. These findings show that there is a missing link between cocaine and addiction that has not yet been addressed, or at least discovered, in research.
Bupropion is another drug that exerts its actions through blockage of the dopamine transporter. This is its main differing feature from other antidepressants as it is approximately 2 fold more potent as an inhibitor of dopamine uptake into striatal synaptosomes than as an inhibitor of norepinephrine (NE) uptake into hypothalamic synaptosomes [6]. However, it does not produce the euphoric or addictive effects seen in cocaine administration that are often attributed to blockage of dopamine reuptake.
Interestingly, however, there have been recent, unprecedented outbreaks of bupropion abuse in Toronto. Those using it in this addictive manner claim that when administered intravenously (IV), bupropion produces effects similar to that of “crack” at a much cheaper price [7]. This rapid onset of the drug effects as a result of the IV administration produced pharmacokinetics far different from what is seen when it is administered orally, as recommended.
Cocaine, when taken recreationally, is most often administered intranasally. This already presents a major differing factor from Bupropion which serves as a potential theory for the differing effects. Since oral administration results in slow absorption of the drug, there is, consequently, slow drug availability to the brain. On the other hand, drugs with a faster onset, produce higher drug bioavailability, and put the user at higher risk of addiction1. Though intranasal administration moves the drug very rapidly, the difference between orally- and intranasally-administered is not significant. In a study examining this phenomenon, it was found that peak plasma levels after intranasal crystalline cocaine occurred at an average of 35 minutes, while oral administered cocaine took about 30 minutes to become detectable and then reached peak levels after 64 minutes [8]. Despite this, both routes of administration showed roughly the same rate of metabolization, as shown in figure 1,
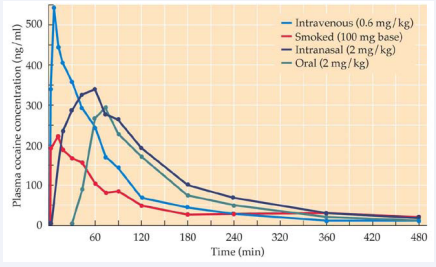
Figure 1 Plasma cocaine concentration from 0 to 480 minutes after cocaine administration, comparing the pharmacokinetics of the four different methods of administration
which suggests that the effects are similar in potency.
The results of previous studies support the idea that metabolites play a critical role in drug action. While Cocaine can be metabolized within a matter of 60 to 90 minutes, its metabolites may stay in the system for a couple of days1. This corroborates this study’s hypothesis of metabolites’ potential role in maintaining cocaine addiction as their effects are present for much longer than that of cocaine itself. The most prominent metabolites of cocaine are norcocaine, benzoylecgonine, and Cocaethylene while norcocaine is the only pharmacologically active metabolite [9].
Norcocaine, an N-demethylated metabolite of cocaine that has been identified in several species, produces several of its own effects past cocaine metabolism. Research has found it to be just as active as cocaine in inhibiting NE uptake by hypothalamic synaptosomes and actually produces greater local anesthetic potency than cocaine9. Nevertheless, studies have not indicated any change in dopamine levels. Its strong anesthetic properties, however, lead to the hypothesis that norcocaine may have reinforcing effects as previous studies have found local anesthetics, other than cocaine, to be preferred in a drug discrimination paradigm [10]. This is all suggestive that drug addiction may have less to do with activation of the dopamine pathway as previously thought and that drug metabolism may play a much bigger role than currently shown in research.
CONCLUSION
Given the lack of knowledge on several parts of this study, there are several limitations that must be addressed. Though mice tend to provide accurate results with high predictive validity for humans-especially in drug administration tests-it is a point that must be addressed since we were not able to directly test effects on humans. Moreover, the lab environment further limits our understanding of what the average cocaine user is experiencing since street dealers tend to mix cocaine with other drugs, such as amphetamines and synthetic opioids, which would produce different metabolites and, therefore, cannot be attributed to the findings of this study [3]. Though there is currently a lack of understanding about the complete mechanism underlying addiction to dopaminergic substances, the differences in the processes of metabolism is explanatory of the a large chunk of it though and this is a topic that must be further explored in future experiments.









































































































































{kind=link}