Acute Coronary Syndrome after Treatment of Coronary Subclavian Steal Syndrome
- 1. Department of Cardiology, Bülent Ecevit University, Turkey
Abstract
Left Subclavian artery stenosis can be a cause of recurrent angina after coronary artery bypass grafting in patients with a coronary steal. These patients may suffer claudication in the left arm and angina pectoris when using their left arm. The subclavian artery shows retrograde filling with use of a left internal mammary artery graft, which can cause coronary ischemia depending on blood flow. This is a report of a patient who presented with coronary subclavian steal syndrome and underwent percutaneous implantation of a stent in the left subclavian artery. However, the patient was readmitted with acute coronary syndrome 1 year later. An angiogram showed an unexpected decrease in anterograde flow in the left internal mammary artery graft after stenting the subclavian artery.
Keywords
Acute coronary syndrome, Subclavian artery, Coronary artery bypass grafting
Citation
Kalayci B, Kalayci S (2016) Acute Coronary Syndrome after Treatment of Coronary Subclavian Steal Syndrome. J Cardiol Clin Res 4(8): 1088.
INTRODUCTION
Left subclavian artery stenosis is a cause of recurrent angina after coronary artery bypass grafting (CABG) in patients with coronary steal syndrome. The patients can suffer claudication in the left arm and angina pectoris when using their left arm. The subclavian artery shows retrograde filling when a left internal mammary artery (LIMA) graft is used, which can cause coronary ischemia depending on blood flow. Herein, we report a case of coronary subclavian steal syndrome (CSSS) in a male patient who underwent percutaneous implantation of a stent into the left subclavian artery. However, the patient was re-admitted with acute coronary syndrome 1 year later. Angiography showed an unexpected decrease in anterograde flow in the LIMA graft after stenting the subclavian artery.
Recurrent angina can occur as a result of atherosclerotic progression of coronary lesions after CABG [1]. Left subclavian artery stenosis proximal to the LIMA graft is a rare and critical cause of angina following CABG. Therefore, CSSS should be considered in patients with claudication in the left arm and angina pectoris when using their left arm. Retrograde filling may result from circulation from the LIMA to the left subclavian artery depending on the coronary blood flow and may cause myocardial ischemia and thereby CSSS eventually.
CASE PRESENTATION
A 57-year-old male smoker with hypertension and a history of coronary artery disease was admitted to our clinic. He had undergone CABG 7 years previously. He was being re admitted for angina pectoris and a painful left arm when in use, particularly when carrying bags. The angina had progressively worsened, occurring during mild efforts and posing some limitations on his daily activities, but it resolved with rest. The patient was not suspected of having arm paresthesia. Physical examination findings were normal except a distinct difference in blood pressure (i.e., 20 mmHg) between the two arms. Electrocardiography, echocardiography, and laboratory studies were unremarkable on admission. Coronary angiography and bypass graft imaging revealed mild to moderate coronary stenosis in the mid-region of the left anterior descending (LAD) artery and retrograde filling of the LIMA bypass. Retrograde flow in the LIMA graft was revealed by angiography obtained from the LAD artery to the left subclavian and left vertebral artery (Figure 1).
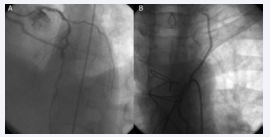
Figure 1: Left coronary coronarography reveals stenos is in the left anterior descending (LAD) artery and retrograde filling of the left internal mammary artery (LIMA) graft (A). Retrograde flow from the LAD to left subclavian and left vertebral arteries (B)
The saphenous vein graft to the left circumflex artery and right coronary artery was nearly normal. Significant stenosis of the left subclavian artery proximal to the origin of the LIMA was detected by angiography (Figure 2).
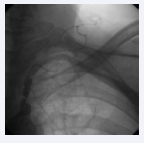
Figure 2: Severe subclavian artery stenosis before stenting
Based on these findings, we recommended percutaneous treatment. However, the patient rejected treatment. A percutaneous stent was implanted into the left subclavian artery 1 month later at another clinic. Clopidogrel was added to his treatment regimen. The patient had an uneventful course following stent implantation but was admitted to the emergency department 1 year later with unstable angina. Coronary angiography revealed reduced retrograde flow in the LIMA from the LAD artery (Figure 3A).
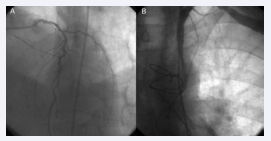
Figure 3: Subclavian artery (A) and decreased anterograde blood flow in the left internal mammary artery (LIMA) after stenting the subclavian artery (B).
Anterograde flow in the LIMA was also reduced unexpectedly as a result of flow competition between the LAD artery and LIMA (Figure 3B). Subclavian angiography revealed a patent subclavian artery stent. As a result, the patient was scheduled for follow-up visits under pharmacological therapy.
DISCUSSION
CSSS is defined by a reversal of coronary flow in the LIMA caused by proximal subclavian artery stenos is [2,3] .Its diagnosis is determined easily by angiography [3].The clinical spectrum of CSSS is broad and includes stable angina, silent ischemia, or acute coronary syndrome [4,5]
Reversed flow in the subclavian artery is usually part of the cause of significant stenosis in the LAD artery. However, flow may rarely reach the subclavian artery because of the blood flow from the native vessel and the peripheral vascular resistance of the subclavian artery [4]. As a result, myocardial ischemia may develop upon use of the left arm as a result of a blood flow shift from the LAD artery to the subclavian artery. These patients are often admitted with stable angina. However, they may also present with acute coronary syndrome [5,6] .
The treatment for CSSS is revascularization of the subclavian artery. The subclavian artery and anterograde LIMA flow may increase following a successful subclavian angioplasty [3]. However, the anterograde flow in the LIMA graft may decrease following percutaneous treatment of the competing flow.
Acute coronary syndrome was diagnosed for multiple reasons in our case. One possible mechanism is plaque destabilization in the native coronary, subclavian artery, or coronary grafts with distal micro-embolization. Endothelial dysfunction or microvascular disease may also cause unstable angina [2]. Another mechanism is increased peripheral vascular resistance of the subclavian artery following angioplasty, as in our case.
In conclusion, CSSS can be treated successfully by subclavian angioplasty. However, these patients may encounter recurrent cardiac events due to diffuse atherosclerotic plaques. They may be admitted with acute coronary syndrome following percutaneous treatment. The culprit lesion was a challenge to identify in the present case. Although the subclavian stent was patent, the LIMA graft was recognized as the culprit lesion.









































































































































