Coronary Stents are Implanted for a Lifetime ?
- 1. Intensive Cardiac Therapy Clinic, Chair of Interventional Cardiology and Electrocardiology, Medical University of Lodz, Poland
Abstract
Percutaneous coronary angioplasty (PCI) with stent implantation is widely used method of treatment of coronary artery lesions. Before the era of bioresorbable stents once stent was implanted it stayed for ever in the coronary artery. The most common complications of PCI are coronary artery dissection, stent restenosis or stent thrombosis. Malaposition of stent struts is one of the most important factors of stent thrombosis. Maloposed stent struts may also lead to severe technical difficulties when performing further PCI procedures in the artery..
Keywords
Percutaneous coronary angioplasty, Thrombosis, Obesity
Citation
Kidawa M, Orlowski B, Krauza G (2018) Coronary Stents are Implanted for a Lifetime ? – Not Always. Stent Retrieval With Guidewire, A Case History. J Cardiol Clin Res 6(1): 1128.
CASE PRESENTATION
Retrieval of coronary stent usually refers to retrieval of embolized devices with various techniques [1]. Unintentional retrieval of previously fully expanded and implanted stent is a extremely rare complication usually associated with severe coronary artery traumatization. In these cases previously implanted stent was extracted due to malfunction of cutting balloon during secondary PCI procedure [2]. In presented case stent extraction was unintentionally performed with ……… BMW guidewire alone.
A 69 years old male, nicotine addict with obesity I*, arterial hypertension II* (ESH/ESC), hyperlipidemia, intermittent left bundle branch block (LBBB) and exertional ischemic angina II* CCS with result of Angio CT scan indicating on the presence of significant lesions in circumflex coronary artery was admitted to the Cardiology department for further invasive diagnostic procedures. In initial coronary angiography a borderline lesion in left anterior descending (LAD) and significant lesions in circumflex artery (CX) and Ist marginal branch (IMg) were discovered. To verify LAD lesion significance intravascular ultrasound (IVUS) examination was performed which proved this lesion to be significant (MLA 4,36-4,41mm2/MLD 1,74-1,79/ CSN 78%.). After Heart team consultation patient was referred for scheduled two staged PCI procedure. During first angioplasty in circumflex artery Orsirio DES stent (3.0 x 30 -12atm) and in Ist marginal branch Xience Pro DES (3.0 x 18 12atm) were implanted with good result, TIMI 3 flow in both arteries and with subtle oversizing in Cx artery (Figure).
Double antiplatelet therapy was initiated and patient was scheduled for second stage of PCI. 3 months later patient was admitted for PCI of left anterior descending artery. Transradial approach was used with 6F leading catheter EBU 3,5, Hi-Torque Balance MiddleWeight Universal II guidewire was introduced into distal part of LAD. Because of ostial localization of LAD lesion second guidewire of the same type was used to secure the Cx artery. However during introduction of this guidewire it was jailed under struts of previously implanted Orsirio stent. First unsuccessful attempt to remove jailed guidewire was done with the help of NicNar 0,85 x 10mm PTCA balloon introduced over the guidewire. During second attempt Cook Vascular Retrieval Forceps VRF-3.0- 135 were used, however without effect. In attempt to change Orsirio stent geometry an inflation of semi compliant NC Trek balloon 3,5 x 15 (8 atm) was done, then with forceful steady traction the jailed BMW guidewire was retracted but to the amazement of performing operator with Orsirio stent wiggling on the tip of guidewire. Immediate contrast injection showed that there was no visible circumflex artery damage. However due to suspected, invisible in angiography vascular wall damage, an Orsirio DES 3,5 x 30 (12 atm) was implanted in the replacement of extracted stent. Pictures of the extracted stent and BMW jailed guidewire are presented in (Figures 1,2).
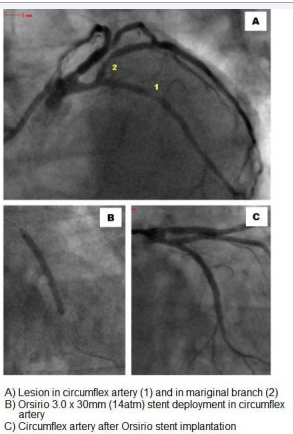
Figure 1 :Initial Angiogram, and first PCI Procedure.
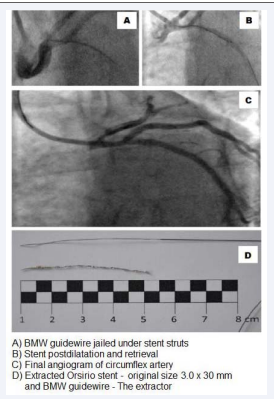
Figure 2: Second procedure and Stent RetrievaL
The stent elongated up to 50mm from original length of 30mm. There is also visible damage to the radioopaque 30mm tip of the guidewire, which was almost broken in two localizations.
During the procedure patient was in stable clinical condition, without any chest pain, total fluoroscopy time was 24 min wit EFD of 2694 mGy, dye administration was 280 ml of Iomeron contrast agent. During in hospital follow up significant rise of cardiac troponin and CK-MB markers was observed (TnT = 866,90 ng/l, CKMB=28 U/l) without any chest pain, ECG changes nor new contractility disorders in echocardiography, therefore myocardial infarction type 4a was not diagnosed. Patient was discharged from the hospital after 72 hours in good clinical shape, with scheduled PCI of LAD in 1 month time.
DISCUSSION
The case history described in our manuscript documents a complication of PCI - an unintended stent extraction. In the modern era of interventional cardiology unintended extraction of previously implanted coronary stent is an extremely rare finding. In PubMed database it is mainly reported in case of repeated PCI because of in stent restenosis. During these procedures an attempt of balloon dilatation of previously implanted stent, with subsequent device dysfunction during retrieval, leaded to unintended stent extraction [2,3 ]. Second most often reason of stent retrieval is it’s embolisation, migration, or deployment failure during PCI procedure [4 ]. However constant development of new materials and introduction of new generations of stents and postdilatation with noncompliant balloons reduced this issue. Dislocated stent may lead to serious complications including cerebral embolism, myocardial infarction or even artery perforation. In the case of stent migration several techniques are recommended to retrieve of the loose stent [1,4-6 ].
Since the beginning of interventional cardiology, the main drawback of angioplasty was an restenosis. To overcome this problem stents were introduced. Subsequently to reduce in stent restenosis drug eluting stents were developed. Antiproliferative substances which elute from DES stents inhibit endothelial hyperplasia, therefore they prolong healing process stopping restenosis. Restenosis ratios with DES significantly lowered but stent thrombosis rates increased mainly due to stent malaposition. Malaposition term refers to phenomenon of stents struts being separated from vessel wall. This may be caused by epicardial coronary spasm during PCI, that can lead to an underestimation of the coronary artery diameter and – as a result - implantation of an undersized stent. As the vessel relaxes, vessel diameter increases resulting in further expansion of this gap. In patients with acute coronary syndrome artery wall may be obscured by thrombus, as this thrombus dissolves over time, the gap between the stent and the wall forms, causing stent malaposition. In the presented case malaposition was the most probable initiator of the complication. Therefore an attempt to introduce BMW guidewire into circumflex artery finished up with jailing the guidewire tip between stent struts. There is no specific guidelines describing how to deal with such a situation, therefore operator used retrieval forceps but without any effect. In that moment senior cardiologist decided to introduce second guidewire into CX. After preshaping the end of the second BMW guidewire, it was introduced into distal part of CX artery. Then postilatation of the stent struts was performed in order to change stent geometry. With the use of constant outward force the guidewire was retracted but as occurred with the stent.
Overall the procedure was successful however there were several moments that might have led to further mishaps. Pulling out the guidewire with constant force may have led to another serious complications including guidewire rupture. Moreover at the same time guiding catheter was deeply intubating the left main stem with the risk of dissection. Fortunately none of the complications developed. Authors decided to pull out the guidewire with constant force, risking its destruction with possibility that some parts could have been left under the stent. Another unused options were to use snare or microcatheters what could minimize chances of artery dissection.
The most amazing finding was the fact that there was no visible damage to the artery after stent extraction. In previously reported cases forceful stent extraction almost often caused major vascular dissection. Therefore this finding supports theory of stent malaposition with the gap between stent struts and CX wall.
This case history serves as an educational example that even “simple” angioplasty could lead into potentially life threatening complications. The end of the procedure was successful however the damage to the guidewire and stent showed that the equipment used, was pushed close to its endurance limits.









































































































































