Giant Right Atrial Myxoma
- 1. Department of Internal Medicine, Memorial University, Canada
- 2. Division of Cardiology, Memorial University, Canada
- 3. Department of Surgery, Memorial University, Canada
Citation
Pirzada A, Hayley B, Adams C (2018) Giant Right Atrial Myxoma. J Cardiol Clin Res 6(1): 1126.
CLINICAL IMAGE
We present the unique case of a 51 year old female with three month history of dyspnea (New York heart association class III symptoms), new onset rapid atrial fibrillation, and an intracardiac mass on surface echocardiography. Past medical history is significant for primary biliary cholangitis. Despite maintaining a high level of function, the patient had increasing lower leg edema, new onset of 20 kg weight gain, and recurrent assessments in the emergency department for shortness of breath. There was no family history of cardiac tumours or Carney syndrome. Physical examination showed rapid atrial fibrillation which was treated with rate control and anticoagulation. The patient had an irregular rhythm with a normal sounding S1 and S2; no addition hearts sounds or murmurs were detected. She had severe ascites and diffuse anasarca up to the level of her umbilicus. Transthoracic echocardiogram revealed a massive intracardiac mass which completely filled the right atrium and went into the right ventricle (Figure 1).
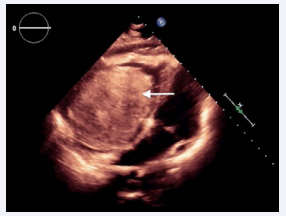
Figure 1: Transthoracic echocardiogram in subcostal view. Right atrial myxoma abutting intraatrial septum (white arrow).
Contrast-enhanced CT confirmed a 9.2 x 8.0 x 7.9cm right atrial mass which extended into the right ventricle and abutted the interatrial septum (Figure 2).

Figure 2 :Contrast-enhanced CT chest in coronal plane. Right atrial myxoma (white arrow).
The mass weighed 167g and was confirmed to have pathological features of an atrial myxoma without any nuclear atypia or mitoses. The patient underwent successful removal, patch repair of the atrial septum and repair of the tricuspid valve via median sternotomy with cardiopulmonary bypass techniques. Immediately after removal the patient had severe right ventricular dysfunction and pulmonary edema and subsequently required veno-arterial extracorporeal membrane oxygenation (ECMO) for three days. Upon successful explant from ECMO, ventricular function returned to normal. However, the patient experienced a complicated postoperative course and developed a severe fungemia with overwhelming sepsis and died of multi-organ failure six weeks post-operation.
Myxomas are the most common primary tumour of the heart, with over 75% originating in the left atrium [1]. Right atrial myxomas are exceedingly rare and present with nonspecific signs and symptoms not limited to weight loss/gain, dyspnea, fatigue, peripheral edema, syncope and pleurisy [2]. Myxomas can vary in size, as demonstrated by a report describing the average diameter to be 5.1 x 1.8cm [3]. The largest portion of the right atrial myxoma surgically excised in this case was 13.7 x 8.2 x 5.3cm. To the best of our knowledge, this is one of the largest right atrial myxomas described in the literature and has several unique features. It is imperative to keep obstructing cardiac mass as part of the differential diagnosis for a patient presenting with recurrent dyspnea and vague symptoms.









































































































































