TEVAR for Treatment of Metallic Pedicle Screw Penetrating the Thoracic Aorta
- 1. Sanger Heart and Vascular Institute, Atrium Health, USA
Abstract
Iatrogenic aortic injuries are a rare complication of spinal surgery. While there is no consensus on the best treatment for these patients, there have been successful reports of both open and endovascular techniques. We report a case of delayed thoracic iatrogenic aortic injury following spinal surgery that was treated with TEVAR and screw removal. A pedicle screw that was placed during treatment of a compression fracture was found, three years later, to be piercing the thoracic aorta. A 28mm x 28 mm x 100mm thoracic stent graft was deployed in standard fashion to cover the area of injury, and the screw was removed. The operation was successful and patient was followed for one year with no complications relating to her repair. TEVAR prior to the screw removal provides appropriate coverage of the injury and appears to be a safe and durable option.
Keywords
Endovascular; Aortic; Spinal; Fixation; Screw; Iatrogenic
Citation
Yammine H, Ballast JK, Boyes C, Arko FR (2018) TEVAR for Treatment of Metallic Pedicle Screw Penetrating the Thoracic Aorta. J Cardiol Clin Res 6(2): 1132.
ABBREVIATIONS
TEVAR: Thoracic Aortic Endovascular Repair; LSA: Left Subclavian Artery; IVUS: Intravascular Ultrasound; CTA: Computed Tomography Angiography; ICU: Intensive Care Unit
INTRODUCTION
Iatrogenic aortic injuries are a rare complication of spinal surgery [1]. Because of the proximity of the thoracic aorta to the spine, malpositioned pedicle screws have the potential to cause serious injury both intraoperatively and years later [2]. While there is no consensus on the best treatment for these patients, there have been successful reports of both open and endovascular techniques [3]. We report a case of delayed thoracic iatrogenic aortic injury following spinal surgery that was treated with TEVAR.
CASE PRESENTATION
A woman with a T4 compression fracture underwent thoracic fusion T6-11 with posterior instrument hardware. Three years later, at 59 years of age, she presented to her neurosurgeon with increasing back pain. A CTA was performed, revealing that a malpositioned pedicle screw was piercing the thoracic aorta so the patient was referred to vascular surgery (Figure 1).

Figure 1 :Preoperative CTA demonstrating pedicle screw (arrow) penetrating into the lumen of the aorta
On evaluation, the patient was complaining of back pain but was otherwise healthy. Findings were discussed with the patient and a plan was made for operative intervention: TEVAR to repair the aorta, followed by surgical removal of the screw by neurosurgery.
The procedure was done in two stages. First the patient was placed in supine position. An incision was made in the right groin and the right common femoral artery was dissected out, and an 8 French sheath was placed. A Glidewire was placed in the ascending aorta over a wire and then exchanged into a stiff wire. The left groin was accessed under ultrasound guidance and a 5 French sheath was placed. A pigtail catheter was placed over a wire in the ascending aorta. IVUS was used first and it demonstrated clear evidence of a screw penetrating the thoracic aorta approximately 5 cm distal to the left subclavian (Figure 2).
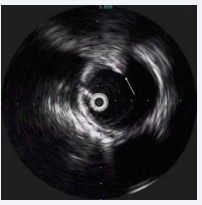
Figure 2: Intraoperative IVUS demonstrating pedicle screw (arrow) penetrating into the lumen of the aorta
Aortography did not show any extravasation (Figure 3).
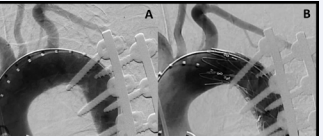
Figure 3: (A) – preoperative aortography with no extravasation. (B) –successful deployment of stent graft with minimal indenting. It is worth noting that due to the overlay of images, aortography is not a dependable method for accurately presenting the true relationship between screw and aorta
Aortic diameter was measured on IVUS and a 28mm x 28 mm x 100mm Valiant™ thoracic stent graft (Medtronic Inc, Santa Rosa, CA) was deployed in standard fashion to cover the area of injury. Completion arteriography as well as IVUS demonstrated complete coverage of the pedicle screw, with only mild indenting of the stent graft (Figure 3B). Once the aortic stage of the procedure was done, the patient was positioned prone and the screws were removed.
The patient was transferred out of the ICU on post-operative day 1 and was discharged home on post-op day 2. At 6-week follow-up, she was doing well with no new or worsening back pain. Patient has been followed for one year with no complications relating to her repair.
DISCUSSION
Spinal fixation with pedicle screws has been found to be a relatively safe procedure [4]. However, accurate placement of pedicle screws is known to be challenging, with the rate of pedicle screw malposition reported at 1.5% to 23% [4,5]. In fact, a recent retrospective chart review of 2724 screws placed in 127 patients found that only about 18% of patients had all screws placed accurately [6]. The proximity of the aorta to the spine leaves it vulnerable to potential injury during spinal surgery, especially in patients with spinal deformities [7,8]. Several studies have found that 1.8% to 14.2% of screws demonstrated aortic abutment, and a 2014 study that examined 964 patients who received 6816 freehand-placed pedicle screws found that 0.29% of thoracic pedicle screws encroached on the aorta [9-11]. Overall, the incidence of iatrogenic injury to major vascular structures after spinal surgery is quite rare, reported in <1% of operations [12].
Most commonly, these injuries affect the lower abdominal aorta or proximal iliac vessels, but thoracic aortic injuries have also been described in multiple case reports [3,13].
The presentation of such injuries varies widely. Some may be dramatic: a perforation or rupture resulting in hemodynamic instability, acute hemorrhage, and rapid hematoma formation [14-16]. Others are characterized by the eventual development of a pseudo aneurysm at the point of contact, while many cases have been identified in patients with pain, or on routine CT follow-up [17-19]. Iatrogenic injuries can occur at any point during or after surgery, and cases have been reported even at 20 years after initial spinal surgery [19-21].
The treatment of iatrogenic thoracic aortic injury as a result of thoracic pedicle screws varies, with successful utilization of both endovascular and open strategies [3,18]. We described a case of endovascular repair, which is gaining attention as more procedures are performed successfully [3].
The best approach in terms of when to remove the screw (if at all) in relation to the timing of the stent graft deployment is difficult to determine due to the paucity of these cases. Clarke et al describe a case where they removed the screw with the intent to perform an angiogram prior to deployment of a stent graft [22]. However, once the screw was removed, there was a gush of blood from the hole and they had to insert a replacement screw to staunch the flow from the hole prior to delivering the aortic stent [22]. Simultaneous removal of the screws with deployment of endograft has also been reported, due to concern that the screws would damage the endograft if it was deployed prior to removal of the screws [21,23]. This technique requires incredibly tight cooperation between neurology and vascular surgeons and positioning of the patient in left lateral or left thoracotomy position.
Our patient, on the other hand, underwent endovascular stenting prior to removal of the screw as a measure to prevent hemorrhage. In our case, as described above, the patient had the TEVAR performed prior to removal of the screw, during the same operation. This was similar to cases described by Pesenti, Hu, Lagios, and Rabellino, among others [24-27]. The outcomes have been positive in the cases that report this technique, but it should be noted that vascular and spine teams still need a high level of cooperation. Repositioning of the patient between the vascular and spinal portions of the procedure was required in most of the procedures reported. Some endovascular procedures have also been performed without removal of the impinging screw, with positive outcomes [19,20].
We are not aware of any series that has looked at rates of spinal ischemia after TEVAR for patients with iatrogenic aortic injury. However, the results of the RESCUE trial examining TEVAR in patients with blunt thoracic aortic injuries suggest that the risk may be low: out of the 50 patients included in the prospective trial, there were no cases of spinal cord injury through 1 year [28]. Studies have found that length of coverage may be a predictor of spinal cord ischemia after TEVAR, so the ability to use a single short stent graft in these cases suggests that spinal ischemia may not be a major concern in the treatment of patients with iatrogenic aortic injuries [29].
CONCLUSION
Aortic injury due to malposition of spinal screws is a very rare but potentially fatal complication. TEVAR prior to the screw removal provides appropriate coverage of the injury and appears to be a safe and durable option. We recommend use of IVUS intraoperatively in addition to angiography, as preoperative CT scans may not provide clear imaging due to metal artifact. It is also worth noting that over sizing of stent grafts is not needed in these cases because the aorta may be otherwise normal. We also recommend using the shortest graft available order to limit risk of spinal cord ischemia.









































































































































